The rates of cases are certainly plateauing. This CDC site — 2014 Ebola Outbreak in West Africa – Cumulative Reported Cases Graphs — has a review of the cases as they behaved in different countries over the past several months.
Source: www.cdc.gov
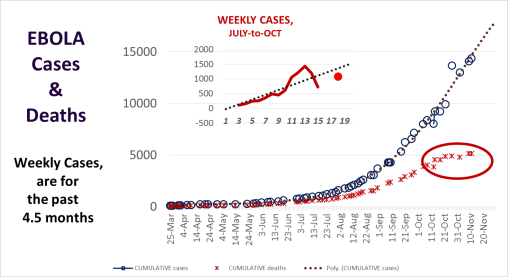
I posted a statement claiming that plateauing had commenced about a week ago, with the numbers evidence for my claim (although early, after just 2.5-3 weeks of leveled numbers in a row). A number of months ago, my model stated this would happen in mid-October, which I correct the the end of October a month later as more weekly values could be evaluated. My model suggests complete reductions due to a saturation of the population, resulting in an impact of the most susceptible followed by a loss in diffusion potentials. This assumed there is no new population impacted, located in a very different part of the world like Europe or the United States.
The model I use is a very basic deterministic model, which accounts for systems behavior, not innovative diffusion patterns like the more stochastic/probabilistic models like to depend upon. Since Ebola is in its first pre-pandemic period, this is very much like the first years and diffusion of the earliest Cholera pandemic year–1832 about. Models of that disease pattern published in the 1960s and 1970s demonstrated that a non-hierarchical behavior prevailed in the way the disease impacted the rest of the region infected.
The second time through however in 1849/50 demonstrated a hierarchical diffusion pattern, in which the disease traveled great distances and impacted newer, uninfected populations far away from the source. The future of these hierarchical diffusion processes are predetermined by certain human and natural ecological features, a product of the pathogen’s evolution and ecological history, in combination with climatic and seasonal weather patterns (in the extreme sense, El Nino and global warming impacts, latitude-linked isothermal lines, and the like). Human migration helps the disease to spread, but its potential for become endemic to a region or naturalized is almost completely environmentally based, and heavily dependent upon zoonotic features (for both Cholera and Ebola).
See Gerald F. Pyle’s Applied Medical Geography (Scripta Technica, 1979) for more detailed applications of this method for analyzing spatial disease patterns.
See on Scoop.it – Medical GIS Guide
