I recently completed a major portion of an ongoing research project I have been involved with over the years–the evaluation of the cost of long term care to epileptics in the past, and how we can use it to predict the cost for epilepsy care for upcoming decades.
My method of analysis was quite simple. I took the historical data for specific case(s) and then used the consumer price indexing adjustment formula for inflation to adjust all past costs to the present. I then took the real case data, which resulted in very low risk of need for future care once the “crisis” was complete soon after the age of 45, and expanded it by creating a slightly riskier pre-catastrophic event period (no high cost events) and an ongoing post-crisis/catastrophic event period, with similar activities as those of the previous years, leading up to high cost long term care accomodations.
This methodology is based in part upon methods used to perform a similar analysis back in the late 1990s. I added to this technique, more data on the costs for health care visits, screenings, labs, prescription drugs, CNS testing, emergent care events, etc., etc. than utilized in previously published studies. I also engaged in a full cost analysis of living costs, assuming the patient had no other health condition that might impact results as a covariant.
The emergent care event(s), and subsequent crisis for these cases was a neurosurgical process (left anteromesial temporal lobectomy, applied to this diagnosis for child and adults with the implied CPS or TLE ICD noted in the graphs above.)
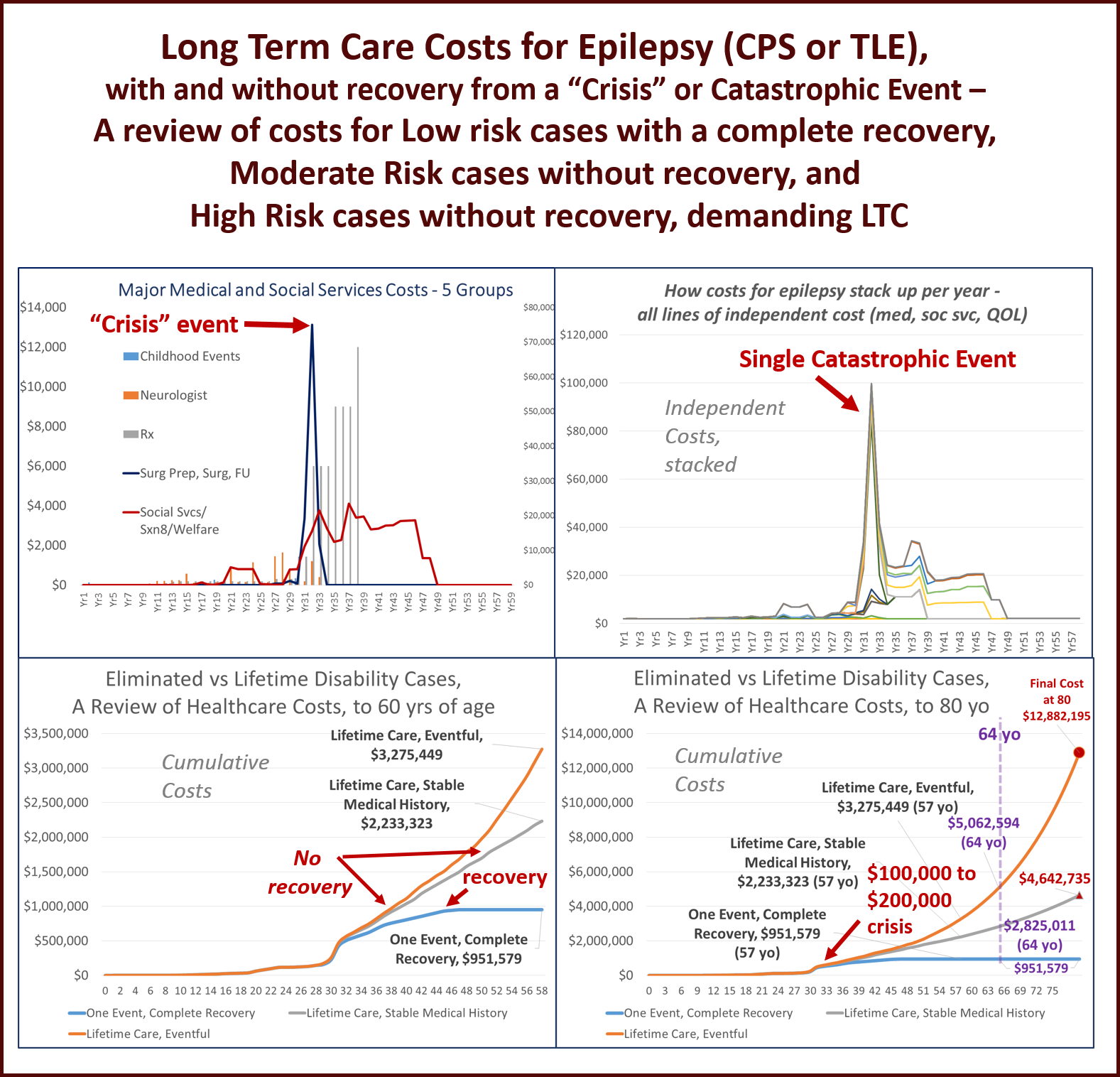
For the baseline case, the surgical process is assumed to be 100% effective, performed at the midlife of the patient’s life. This lowest risk case is also assumed to recover completely from the crisis and return to education and/or work without further complications (essentially representing a “cure”).
The moderate risk case continues to experience post-surgical seizure events, although less at first, but over time requires new testing, new medications, further tests and screening, changes in therapies, etc.
The high risk case is assumed to have ongoing debilitating conditions develop even after the surgery is completed, as the seizures recur and reduce quality of life over the next 20 years.
The costs for each of these cases up until the age of 57/58 yo were then reviewed (again. starting with real time/life costs for care data for the baseline case). The other two were then evaluated.
Based on changes in cost over time, and their linear versus polynomial form, a prediction modeling equation could defined for each of the moderate and high risk cases (formulas were different), to determine how much ongoing medical care for this health status would cost the system ,first by the age of 65 (retirement year, if any were still employed), and finally, by the age of 80.
The results of this study demonstrated that the long term cost for lifetime care for a patient with epilepsy, who reaches the age of 80, but requires special housing in the later years due to long term complications, could easily reach 10 MILLION DOLLARS (much of this due to long term care demands).
(All additional costs were not CPI adjusted for future inflation, but the prediction model equation takes much of the trend with inflation into account).
The moderate risk cases (presumably the majority of cases in this age range), cost the taxpayer-funded healthcare system (preretirement years=Medicaid; post-retirement=Medicare) a little less than five million dollars.
What makes this analysis different is the inclusion of costs for social services related services and intervention events, for all stages in the a patient’s life, from childhood years through college and early employment years, into hospitalization and post-hospitalization/post-surgical years (counseling, neurosurgical counseling, neurosurgical testing, WAIS, and post-surgical occupational and cognitive speech therapy reviews were included.)
Each of these two types of patients was also assumed to receive continued MCD/MCR assistance for the rest of his/her life, including Section 8 and Food Stamps coverage, to name a few of the additional costs not fully evaluated in the older forms of this study performed back in the late 1990s.
No early mortality was assumed for these cases. Since people with active, ongoing epilepsy are normally assumed to demonstrate a reduced lifespan of about 10-20 years, this could be considered the one flaw in this analysis. With such a reduction in longevity, a significant number of these two high cost groups would die off well before the age of 70.
Nevertheless, this provides a reason for engaging in more aggressive, early interventions into epilepsy care. The recovered individual cost the system nearly a half-million dollars in real money, a little less than one-million dollars once these costs are CPI adjusted. And such an outcome (“the cure”) is an infrequent event.
In sum, the moderate case can cost anywhere from 4 to 5 times more than the recovered epileptic.
The highest risk cases can cost the system as much as 12-fold, according to this analyses. Even if we cut this amount in half, we are still talking about an additional 6 million dollars in cost of care over time.
These amounts per patient by the way represent costs per year that are higher than what most individuals earn in these same age groups, were they employed.
Each case therefore represents a reduction in taxpayer income for the country, with each dollar traded over for each dollar required of the medicaid or medicare systems. This amount doubles for high risk patients.
More importantly, the cost for caring for a typical high risk patient between 70 and 80 years of age will cost the system about a quarter million dollars per year.
The total cost for the care of retired people with epilepsy in upcoming years has been estimated to be in the billions, with about one million people who are now eligible for this health care assistance, should they still be around about 20 to 25 years from now.
For more on this study, go to https://altonenb.wordpress.com/
See on Scoop.it – Global∑os® (GlobalEOS)
