USA Today Editorial states: “Last year, the U.S. saw 668 cases. Midway through 2015, about 180 people across half the states have been sickened. Many cases were linked to an outbreak at California’s Disneyland, and most of those who’ve fallen ill were never vaccinated. Last week, Washington state reported the first death from measles in the U.S. in 12 years.” and “States that still allow easy opt-outs should follow Vermont and California. . . . “
Sourced through Scoop.it from: www.usatoday.com
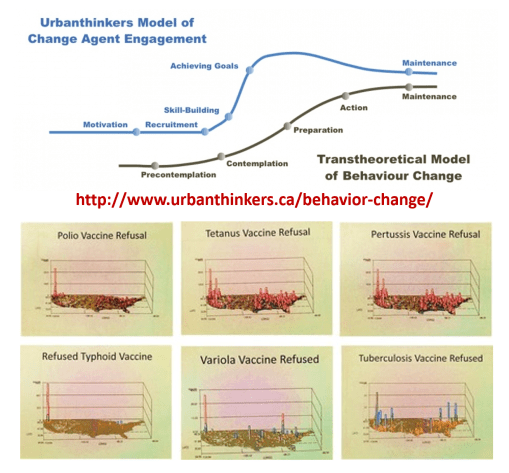
Let’s apply Prochaska’s Transtheoretical Model of Behavioral Change to this public health/healthcare administration problem.
The healthcare programs in the US are for the most part either in the pre-contemplative or contemplative stage for GIS implementation. The more engaged programs are focused on skill building. Utilization of just a simple spatial program to map your data is early "Preparation" Unless you have a GIS established that deals with all QIAs, PIPs, MUs, Chronic Diseases, and the majority of HEDIS metrics, reported yearly, your agency, company, or facility is not in the Action stage.
Based on my national GIS/NPHG study outcomes, my recommendations are as follows:
#1 – regarding refusals to immunize, focus on the Seattle, Portland, San Francisco, and maybe Los Angeles areas.
#2 – approach insurance companies and physicians’ businesses in the Pacific NW urban settings and ask them why they have facilitated this problem for 25 years.
#3 – develop mandatory rural health monitoring programs for the Pacific Northwest
#4 – research the in-migration track from NYC to Albany where the hot spots develop due to tourism and immigration.
#5 – improve public health security programs designed to prevent the spread of immunizable diseases into Canada via the Buffalo area and other Great Lakes related paths into Canada; apply this to all other high fatality diseases capable of crossing borders (this is possibly the chief route for unexpected yellow fever entry).
#6 – continue to vamp up Mex-Tex border security, and establish plans for the south the north route these individual take with their disease, from the border to Midwestern cities along the Mississippi and Chicago.
#7 – increase public health security along the Haiti/Cuba-to-Florida route (chikungunya and naturalized Ebola/Ebola host routes).
#8 – set up a plan for potential polio re-emergence around the Great Lakes; consider Canada or Chicago a possible direct or indirect (via NYC) point of entry.
#9 – require the largest health insurance companies like Aetna, Anthem BCBS, Blue Cross Blue Shield, Cambia, Cigna, Emblem, Fortis, Kaiser Permanente, UnitedHealth, to initiate a medical GIS program immediately, that is capable of working in 9 months, to begin quarterly reporting in 12 months.
#10 – Retire all CIOs, CTOs, Directors, VPs, managers, in charge of IT/HIT/QI/QA, who lack spatial epidemiological background and experience, and have not published or presented a demonstration of their unique skills by the implementation of new programs and/or publication of spatial epidemiology results that are more than just descriptive statistics.
For those highly adventurous, I recommend:
#11 develop a program that separates and spatially evaluates sociocultural and socioeconomic classes of diseases and quality of care (in descending order of priority) for: lowest income classes, highest cost CDMs, african/african-american, hispanic and subgroups, asian/asian-american, native american groups.
See on Scoop.it – Medical GIS Guide
