In a recent re-review of infibulation in the U.S., in particular a section of it that is predominantly black, with hundreds of thousands or people of the right descent, I uncovered ICD evidence for 4000 patients from a population of just about 160,000. I then evaluated the age profile of these patients, and duplicated my findings from 7 and 10 years ago. The most important repeated finding was that about 0.5% of these 4,000 were under 18 years of age, with the lowest frequency of events noted for the 12 year olds. How do we interpret these findings?
My interpretation of these findings is that the four peak ages for infibulation (ca. 1 year old, 3-4, 7, and 13-14–this graph not displayed) suggests the following:
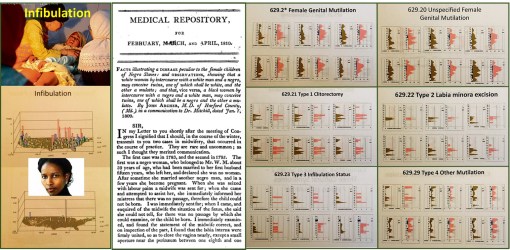
1. that there are at least two kinds of infibulation being performed on children (four are differentiated with the version 9 ICDs); the younger ones do get the less traumatic form perhaps, because of its potential fatalities.
2. Children who undergo this process are the fewest at 12 years of age (in fact pretty much nil), because they are sen to their family’s homeland for the process to be performed–it is illegal to perform in the U.S.
3. The 1, 3-4, 7 and maybe even some of the 13 year old children who are noted as having endured this process, and are now U.S. citizens, may have in fact received that procedure in the U.S. The younger the victim identified in this study, the more likely this practice was performed in the United States, and again–illegally.
There are cultural explanations for the 1, 3-4 and 7 years old procedures. The 3-4 year olds stand out however, because they are the years just before pre-schooling and public schooling.
The number of patients who may have had this process performed in the U.S. is about 160 out of the 200, who are under 18 years of age and have this diagnosis in their EMRs. Even if half of those very young cases were performed outside the U.S., this means that 80 were still illegally performed in the U.S.
So, there’s no getting around this point: there are individuals in the U.S. who may be performing/practicing infibulation on very young girls, because the parents (and perhaps mostly the father) believe this cultural belief is essential, because she (the daughter) cannot be trusted, and must be taught how to remain a virgin until her “culturally appropriate” marriage.
One of the most incredible rates of change for this practice in the 4,000 women identified and researched for this study, the escalation in numbers (percents) of cases between 15 and 25 years of age is phenomenal. If your people, family, believe it must be practiced, then there is no way around this sociocultural requirement for growing up.
This study duplicates my past reviews of this most controversial issue, which I predict will increase several fold over the next several years. The events that will increase the most are the illegal performance of this practice is certain communities, rather than send the 11 or 12 years old girl back to the homelands. (See a recent news story on this issue, related to Pakistan: Send Girls Off to Learn, Not Off to Marry, Says 13-Year-Old Pakistani Activist–http://news.yahoo.com/send-girls-off-learn-not-off-marry-says-211504295.html ) The field of medicine, and even the government offices that oversee health matters, haven’t the knowledge base, know-how or ability to manage these back room illegal practices that go on in culturally defined medical practices.
Medicine is often treated like religion by certain government services. Some forms of health care practice are based on belief and cultural acceptance. We do not intervene in these practices; the leaders turn their heads away from watching them happen. “Politically correct” is a must for some religions, some medical philosophies. In the case of infibulation, the patient’s rights are being ignored each and every time we let that happen, making it possible for physicians from other traditions to engage in a practice that is typically taboo and considered cruel to patients when engaged in the U.S., and most developed country settings.
WHO does not support infibulation. Neither should we.
My stats tell me that from one to five of these events occur every month in the region I am studying.
For more on this process, my past videos and maps of its happening across the U.S., based on an evaluation of 50-60M people, go to:
3 videos of the map of the U.S., depicting these cases (my 3D rotating map images of the US):
www.youtube.com/watch?v=0A95jfeAScw
www.youtube.com/watch?v=mNGxDzOkl_Q
A page with links to the Youtube videos on this controversial topic:
https://www.youtube.com/playlist?list=PLCu236rTh0duC4Euag8Fpz7JW19c2LPCr
See on Scoop.it – Medical GIS Guide
