From 1987 to 2000 I ran a lab at the local university that specialized in testing phytochemicals. My focus was on my own “discovery” of the local yew tree as a source for a new treatment for breast cancer, which would be marketed several years later as Taxol. That study was second to my study of benzylisoquinoline (BIQ) alkaloids, metabolically active selective toxins capable of being applied as medicines. I also monitored OTC herbal products for adulteration and counterfeits, and occasionally followed up on complaints of toxicity.
Sourced through Scoop.it from: www.newsweek.com
This current argument, pertaining to antioxidants, mimics similar events that ensued in the late 1980s for Echinacea, when it was promoted for treating AIDs. Many herbal medicines are potential victims of this slippery slope error, usually made by their most devoted (and highly biased) advocates.
During my 20 years working as a phytochemist and phytotaxonomist specialized in the pathways for developing new products, I attended hundreds of presentations, classroom teachings, and other public events about the new claims to herbal medicines arising over the years.
Echinacea was the first attack I would make on these claims, as the researcher, lecturer and professor in natural products chemistry from 1989 to 2000. The primary individual promoting Echinacea at this time recommended it for treating AIDs. Attending one of his sessions, I asked about its mechanisms of action; he was unfamiliar with the contradictory nature of his claim, which stated that an herb stimulating the immune system would help “cure” or minimize AIDs related complications because of its non-specific “immunogenic” effect. (Lucky guess on which pathways to take, I guess.)
For the next decade we contested each other’s claims about what is “efficaciousness”, when it came to herbal medications and their nutriceuticals. Ultimately, some people in this profession developed a better understanding of the immune system processes, and the varying pharmaceutical nature of the ‘Chemicals in Plants’ (the name of my most popular course at PSU for 15 years).
Also note, these same incompletely researched arguments have been made for plant seed oils, in particular arguments that posed ideas about prostaglandins and prostacyclins, not to mention the other arachidonates and EPAs. Such arguments claimed that generically assisting the body in its chemical processes somehow results in a therapeutic effect because nature selects the right side of the pathway to health for its plant chemicals to take. (Or maybe it’s simple “luck of the draw”!)
Similarly, herbalists rarely take into account the opposing natures by which black cohosh and blue cohosh on uterine muscle and blood vessel walls; the effects of the two, when taken together, are in opposition to each other in some cases.
Over the years, I demonstrated that one of the most embarassing things about phytochemical drug related claims is what little herbalists know about the chemical nature and chemical history of some of their most popular products.
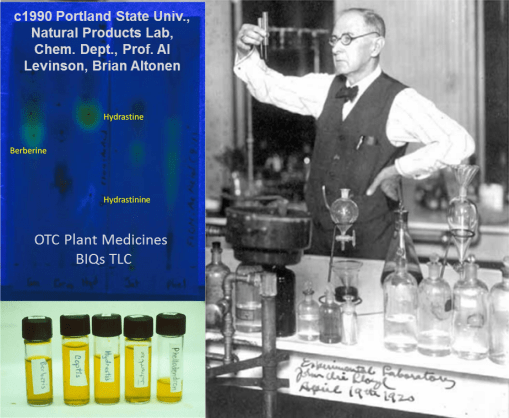
Since I specialized in BIQ alkaloids back then, I reviewed the “curative” BIQs purportedly in Goldenseal (Hydrastis canadensis) from 1990 to 1993; I presented these findings several times, including at OAS. I found that hydrastine (green to gold on the TLC) rapidly decays to produce hydrastinine (sky blue). Different products had different amounts of hydrastinine produced, indicating substantial irregularities within the herbal medicine trade.
That second product (light blue hydrastinine) is a result of the oxidation of hydrastine to hydrastinine, by light, heat, exposure to oxygen, free radicalization, etc. This chemical conversion also changes the questionably-proven antibiotic Goldenseal powder into a better-documented smooth muscle relaxant (see ‘The Merck Index’, 1970s). Since the half life of hydrastine (the desired antibiotic chemical) is a just few months in powdered products, this means the capsules, teas, and such that are made from golden seal powder may be totally “ineffective” in therapy in overpriced in terms of their hydrastine content. [Take them for your IBS instead; I explain all of this on part of my resume/autobiographical page, at https://brianaltonenmph.com/tag/selective-toxicity/ ].
During the 1990s, some of the OTC industries made corrections for these inconsistencies and even tried standardizing the testing of their alkaloids, flavonoids, and other forms of phytochemical content.
But similar problems ensued. Concerns about the substitution of Devil’s Claw with a closely related “unofficial” species (but perhaps allowable) is currently a major concern. Since the 1920s, there has been this ongoing problem for identifying the right “Pau d’Arco”. Adulteration is also still a problem with herbal medicines, for example, the many “legal highs” may be totally bogus, questionably effective neurotonics. Likewise, the use of “scullcap” for epilepsy has had its non Scutellaria substitutes found in the batches instead. One Uva Ursi (Arctostaphylos uva-ursi) produce sent to me by an Alaskan herbalist ended up being boxwood (Buxus) shrub instead, alkaloids and all. (Grossly, it is a lookalike at first, and so was perhaps gathered by mistake.)
And as usual, poor management of OTC the plant product manufacturing industry remains a major problem with this unmonitored profession. Last week, the story was once again countering the Echinacea immunogenic theory claims.
Finally, I find this problem to be very much like another series of legal cases I managed from 1989 to 1990, involving the Oregon patients who took the first bioengineered version of the OTC nutrichemical, tryptophan (TRP). It was produced by the Japanese company Showa Denko, using aggregate cell culturing (“bacillus soup”) techniques (one of my first professors was Abe Krikorian, who sent the Daucus carota to the Moon and back during one of those Apollo missions, in aggregate rootcap bioengineered form; the cell aggregates survived and produced new plants on earth).
This attempt to make a bioengineered form of TRP for the first time unknowingly resulted in the production of di-TRP, which was undetected, since it never existed before, and found to be neuromyotoxic on skeletal (esp. leg) muscle. [See http://www.nemsn.org/Articles/summary_tryptophan%20Fagan.htm ]
The misfortune there is that this enabled the FDA to regulate TRP rather than require it be tested and monitored for public health safety. That move was obviously one of a political nature, not intended to be solely of a public health nature.
Remember, as a medicine, the herb is what you make of it. As a source for chemicals, however, there’s more to a plant than just a list of compounds, some of which have possible effects.
If only we paid more attention to the highly detailed alchemical history of what’s in a plant.
So many compounds, so many theories. (“So that’s why it worked!”)
PS: Don’t forget the ZMAPP project! This Ebola drug was bioengineered using Tobacco Plant, and the rights to its product and the genetic engineering processes are patented. So this process and its unexpected problems it may cause at times may very well continue. See my related ScoopIt! at http://www.scoop.it/t/episurveillance/p/4026182931/2014/08/12/zmapp-and-the-treatment-of-the-spanish-priest-in-the-madrid-hospital-for-ebola
See on Scoop.it – Episurveillance
