Introduction
With the migration of settlers from the Middle East, Arabic medicine will soon be impacting Western medicine or allopathy. This influence will be in the form of Unani-Tibbs medical practices.
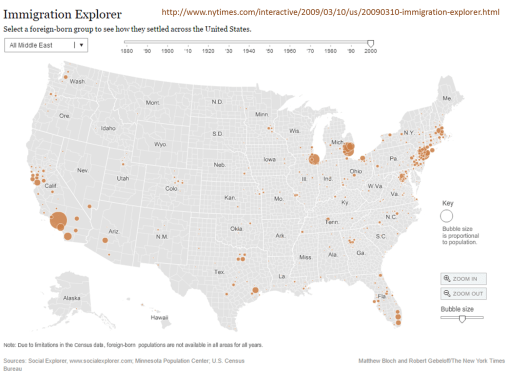
To understand this impact of a newly arriving medical belief, consider the impact that Asian migration has had on the U.S healthcare system since 1830. Whereas there was plenty of migration between the mid-1800s and late 1800s, it wasn’t until well established oriental communities were formed in urban settings, with enough local consumers, in the form of Asian families, available to support a growing medical business devoted to traditional Chinese medicine.
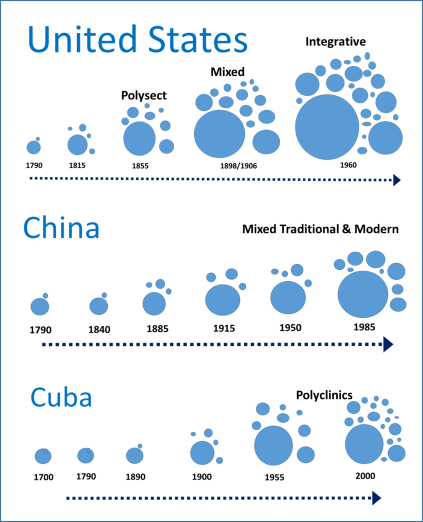
From an older essay comparing these three programs
Oriental Medicine in the US
Within western cultural settings, there have been several stages when parts of the oriental philosophies came to be common practice by western doctors. Most of these methods tried and accepted required some form of western philosophical paradigm to improve their likelihood for acceptance and integration into Western Medicine practice. The most recent examples of these many non-Asian United States citizens are aware of, like the practice of acupuncture and acupressure, the use of ginseng for strengthening the body, ginkgo for the mind.
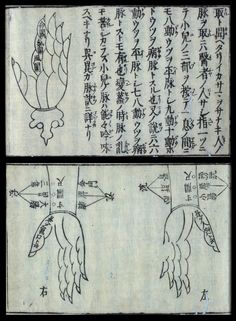
Yet there are parts of the Oriental philosophy which we struggled to develop philosophical interpretations for. One of the earliest Oriental practices noted and almost accepted in western European writings was the use of moxi, a smoldering stick consisted of pressed sage leaves that maintained the fire but not the flame—its purpose: to heat a specific area of the skin, add energy or chi, and improve the vitality of the body there, assist in the flow of its energy from one part of the body to the next, through this area that served as a node or place where such flow could be strengthened.
The acceptance of moxi, more as a curiosity noted in the earliest oriental travelers recounts, initiated as early as 1650. To make sense of it in the traditional four humours paradigm of western medical philosophy, the writers termed it a way to add fire to the four elements that needed to be in balance within. Yet, there were other theories that could be used to explain how Oriental medical practices made sense, many based on the observations made about electricity and the body.
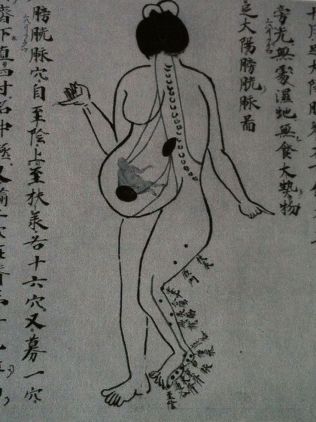
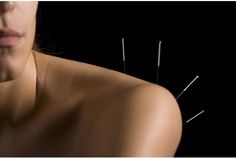
The other practice sometimes reviewed by writers in their recounts of China was acupuncture. To understand acupuncture required a knowledge fo the how the body was shaped, and then how these particular moxi points were distributed across the body surface, and how without heat, but only through the use of a very thin needle, these points could be changed with a barely visible perforation of the skin. This view of the acupuncture needle process seemed counter to the much cruder, more injuring practice of lancing the body, in order to let the blood flow, in the form of the practice of bleeding or bloodletting.
The Western paradigm stated that a certain amount of blood had to be removed, to remove the bad humours within and give room for newer, more healthy humours to form and fill this empty space in the vessels. That philosophy was much easier to visualize and understood, and was accepted as true by Western Doctors, whereas the acupuncture theory that was suggestive of energy flow rather than fluid blood flow, had less evidence to base itself upon. Lanced blood was more convincing than theoretical energy released and allowed to flow freely elsewhere in the living body.
When electrotherapy had its first discoveries, the similarity of these early phenomena to the claims linked to moxi-generated heat and acupuncture-generated energy could be equated with parts of the western medical theory for electric cure. The first form of electricity this related to was equivalent to the concept of the battery, with energy stored in the form of static electric change, stored and held by the Leyden jar, an early form of the capacitor. If one grasped the right wire atop the Jar, a shock was felt, an electric charge, that could in theory “revitalize” the body, and in the realest sense, recharge a heart that has stopped beating. The witnessed evidence that leyden jar and static electric charge production and discharge could revitalize a living thing, was the use of static electric generators to cause a muscle to twitch, to make a seeming dead muscle in a young child paralyzed by a disease like spinal meningitis contract again, offering help to the crippled child and his parents.
The Oriental philosophy of how energy worked in the body, the power of Chi, wasn’t exactly equivalent to the Western medical paradigms upon which certain regimens were discovered and then added to the philosophy at hand. It wasn’t until the 1830s that later stages in the development of the use of electricity, in particular in the form of stored galvanic electricity, led to another rendering of the use of acupuncture to help patients. The acupuncture needle became a medium through which energy flowed, out and across the chi pathway in the sense of oriental methods for its use, from the energy source into the body in the allopathic electric cure sense.
The other forms of Chinese medicine that came to be popular were mostly related to herbs. Ginseng was mostly worth what it was to the Chinese people. But similar tonics could be found in United States treatments that were akin to the Chinese tonic medicines. The occasional overlap between Chinese medicine and Allopathic medicine did happen in the early 19th century, but its impact on the acceptance of traditional Chinese philosophy in general was minimal. Oriental medicines like the Ailanthus glandulosa (Tree of Heaven) became popular because its stench worked against the miasma, not due to an energy it helped to generate in the body to help heal the patient and strengthen a patients defense again sickness. The Chinese ginseng had its American equivalents, but they cost the price of a great medicine, not an aged root worth more than its weight in gold due to its form, age and twisting spiraling nature. A root was simply a root in Western medicine. The purest whitest powder of a starchy Smilax tuber was appreciated due to the nature of it starchy content and its value in preparing formulas, not its symbolic purity.


“Modern” Philosophies and Traditions
The latest rebirths of Oriental medicine, (there were several) came in much the same manner that other forms of “alternative medicine” have come to be practiced. There was this tremendous dissatisfaction with the standard allopathy for the time—people were in need of safer and more trustworthy methods of treatment and cure. During the late 1890s and early 1900s, Oriental medicine was practiced heavily in American office, by Oriental practitioners, sometimes in association with American non-allopathic MDs. The bacterial theory had caused a major eruption in heathcare, enabling non-allopathics to briefly get a hold of the reins once again. If it weren’t for improvements in licensure laws at that time, many of these philosophies might have been here to stay.
But many medicine philosophies were put to the test by the regular medical profession around 1900s. The 1906 Food Act helped further this attitude about health, as did the 1915 Food and Drug Act, which effectively got rid of unfounded or unsupported over the counter drug based remedies (i.e. over the counter opium in treatments for teething babies). Since then, many of the 19th century allopathy skills have since vanished from the medical books. The allopathic standards of leeching, blistering, and bloodletting were the first to go, followed by the excessive use and reliance upon rubefacients and other irritants that in theory were working as “counter irritants”. There was also the reliance upon unusual tools such as the baunscheidtismus contraption, mean to apply the equivalent of many irritants, numerous lances, all in one spot. This elimination of the serious irritant, however, did not completely eliminate the perceived value of the acupuncture needle from Oriental medicine.
When Mao Tse Tung showed the world that acupuncture could be used to perform Open heart surgery in his primary teaching hospitals, the United States and United Nations observers of this practice were not only stunned, they were amazed, and convinced of its success. Chinese medicine has ever since had its periods of acceptance and then rejection by western practitioners, until recently, when allopathy finally decided to include it in the possible treatment paths for specific therapeutic pathways they were unable to be successful with—alcohol abuse, drug abuse being the most prominent, but the treatment of certain chronic diseases like ileal paralysis, chronic back pain and HIV or AIDs infection.

Middle Eastern Unani-Tibbs Medicine
Are the same things that happened with Traditional Chinese Medicine and United States medicine about to happen with Unani-Tibbs medicine?
More than likely yes, but for different reasons.
As the number of families from the Middle East increase, those devoted to practicing their own unique forms of medicine known as Unani-Tibbs will become the standard (if it isn’t already the standard for some community settings). It is possible that the transition of small social settings from western the Sharia Law will provide insights into where these transitions will first take place, and where they will first have their impacts on patients receiving both Unani-Tibbs and Allopathic forms of medical care.
The most important parts of these other forms of medicine that may become a standard in some western medical-integrated healthcare systems are the ways in which some diseases are interpreted, etiologically explained, and then treated. What we learn from how Chinese medicine was introduced into Western Medical practice paradigms may relate to how we should view, study and interpret what events are happening as Unani-Tibbs medicine becomes more popular, and more common.
Like Chinese medicine, Unani-Tibbs medicine does have its own unique way of interpreting the cause of disease, the meaning of diseases, the developmental processes responsible for disease onset, and how to treat and eliminate the disease. Like Chinese medicine, Unani medicine has its more direct, and perhaps reliable and trustworthy applications, at the cultural level, treating behavioral health and psychologically related or induced states, by basing these treatments upon traditional cultural paradigms.
But what about diseases that are mindbody-like in their behavior, those which during the 1940s and 1950 (and even 1960s) we called “psychosomatic diseases”? Irritable Bowel Disease and Fibromyalgia are two very common examples of this. Might other versions of treatment for these long-lasting chronic conditions be beneficial to some patients?
One of the best examples of these conditions which has a very social and cultural definition attached to its seriousness and meaning is Epilepsy. Epilepsy is a prime example of a disease that has different interpretations across different cultures, and perhaps even requires different methods of treatment depending upon the source of the paradigms that guide the lives of specific patients diagnoses with epilepsy.
Djinn, or Jinn
Epilepsy Causality
Like the theory of humours, epilepsy has this long history of definition and redefinition of its cause and treatment over the millennia. Western medicine, Asian medicine, and Middle Eastern medicine have been involved in how we developed our current perceptions of the patient with epilepsy, especially in his or her uncontrollable or intractable state.
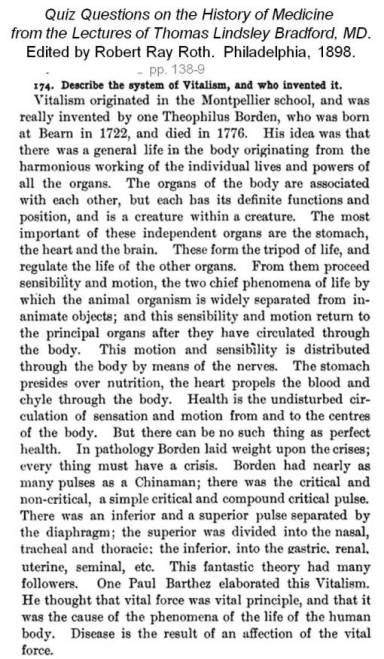
Vitalism – – the Western Medical theory of life energy in 1800 +/- 10 yrs
In the past, western medicine has dealt with the notion that epilepsy is related to some “invasion of spirit concept”. Hippocrates taught that to us, as well as Chinese and Native American doctors and healers. The unexplainable nature of the seizure, and the appearance of the invasion of other beings or demons into the human body, is a cross-cultural paradigm assigned to explaining certain seizure types. The New Testament attests to many examples healed by numbers of healers during their pre-sanctification phase or existence. This same story, so common to most leading religious writings, is curiously absent from the Koran, the reasons for which are in dire need of a professional theological and medical review and the publication of any intense speculation that may arise due to this research by the best scholars in the world.
But until then, we have to deal with the reality of epilepsy—that it exists, and that it impacts Muslims probably as much as it impacts most other populations. If epilepsy is an unusual example of culturally-bound disease pattern, like some of my past writings have suggested, it exists because western medical philosophy allows it to exist, allows for its related behaviors to happen, be interpreted the way they are, and then diagnosed as expected.
As a historian, I always though it curious as to how and why past forms of epilepsy are different from the standards we believe in today. The hysteric convulsion, the French diagnostic categories of seizures were very different from those we believe in right now. They seem to be mostly presentation and symptoms based, relying heavily upon the patient’s appearance and affect during the seizure episode. And when you read some of the severest events as they happen, you have to wonder why they were more often considered a form of sleep walking or somnambulism, or some sort of hallucinatory state like those induced by medicines, or those initiated by the animal spirit in the human body, its emotional system and emotional reaction to the stimuli at large in life, home and society.
Islamic “Treatment of Spirits” (Djinn)
Middle East Interpretations
With patients from the Middle East, they have a unique spiritual and physical medicine interpretation of epilepsy that must be adequately approached by the western physician or neurologist unaware of Islamic beliefs and faith regarding the seizure. That will likely not happen, unless the primary care giver is Islamic himself or herself.
The primary reason a child is brought to the doctor for possible epilepsy, is that the family and closest associates need to know if it is of djinn origins or physical origins.
At first, this seems a very easy problem to deal with. The provider has to convince the parents that the seizure is what s/he (the allopath) thinks or believes it to be. But try to convince a different culture that this interpretation is true.
There is a transition going on in Unani-Tibbs medicine just like there was when Oriental medicine was put under the lens during the late 1800s. We will see transformed Unani-Tibbs trained MDs who are convinced that this traditional path does provide unique opportunities to better a patient’s life. We will also see Unani-Tubbs trained physicians who have moved away from the traditional philosophy and try to lay to rest the fears that riddle the families receiving western medical care who are so concerned about the roles and reasons related to the “evil” forms of disease onset that they experience, and yet no other culture does, in terms of how they interpret it. We will also see traditional MD allopaths, perhaps even of Middle Eastern descent, who haven’t any training in the philosophies of these cultural scientists and medical leaders.
In a recent review of epilepsy cases and their care practices performed in large urban settings, I found that there was a growing number of Middle Eastern parents with children adding to the health care system due to their greater numbers of visits to the provider for children, about their concern that the child might have epilepsy.
By reclassifying the religions noted in their EMR data, I was able to merge the data enough produce classes of religion that could then be used to five major religious groups to each other, and then to several smaller religious or religious-like belief systems that are increasingly popular, and can impact the way patients chose to seek out medical care or not. The final group I defined was the “Unknown” group, patient who had no religious affiliation listed.
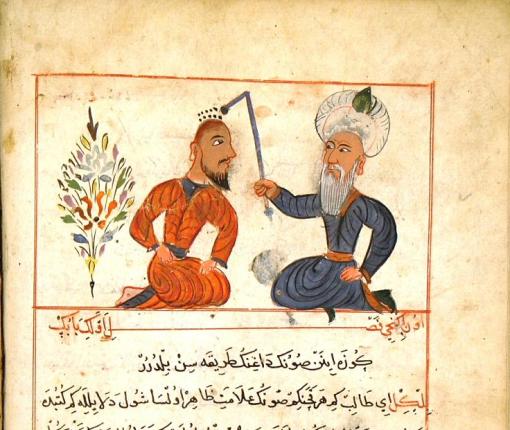
Inoculation discovered – Al Rhazes
Findings
A review of ten groups in terms of the numbers of kids with parents concerned about epilepsy, with the epilepsy ICD in their electronic medical records database, showed that mostly the Middle Eastern families were highly concerned for their child’s welfare when it comes to diagnosing and treating epilepsy for a child who is under the age of 4. They are the only group demonstrating early peaking in visits for this ICD for the one and two year old children, demonstrating aggregate visit rates that more than twice those of any other religious class in the U.S. The summation of these visits for kids by the time the child reached eight years of age, was much greater than the other classes, in particular at the visits and procedures levels. This means that not only were the patients evaluated for possible epilepsy higher in Middle Eastern groups, but also underwent considerable more visits to determine their diagnostic state and many more procedures to confirm the final findings or claims made about a diagnosis.
Equally important to note for this study is that the peak age for children seeking out help or assistance about a possible epilepsy condition is closer to the 8 to 12 year range than the 0-5 year range, like it is with Middle Eastern families. This implies that the non-Middle Eastern families have a wait and see attitude that prevents them from seeking out possible insight into their child’s state, assuming that child even experienced an event that would make the parents be so concerned about epilepsy.
Commentary
The needs for childcare visits for epilepsy for children so young in Middle Eastern families suggests there is a culturally attached belief system feeding into this watching and waiting attitude, avoiding it as much as possible. This could be because the Middle Eastern concerns and judgments about a person who is diagnosed with epilepsy have a much greater impact on that person’s life and the life of his or her family.
One final observation about this Middle Eastern behavior related to seizure related visits and procedures involving very young children is the gender asymmetry of this pattern, with boys receiving this care more than girls. In other cultures, the two genders have equal representation for the most part, with boys sometimes slightly more than girls in early childhood, but with female related visits and procedures performed far outnumbering male visits and procedures for most of the decades to come.
This difference in patients, visits and procedures data for epilepsy related visits, by these ten groups I defined and evaluated for approximately thousands of cases, suggests that this topic is in need of a much more detailed analysis. As the numbers of Middle Eastern patients increase in the years to come, we will most likely see the influences of Unani-Tibbs medicine and philosophy come into play in highly multicultural healthcare settings, in particular the managed care programs.
If the institutions in charge of some managed care system aren’t ready for this change, this could result in less communication between patient and provider in the traditional allopathic healthcare system. We don’t want to see the influx of new cultures lead to the development of another set of new healthcare providers in the United States, not effectively monitored, because the current allopathic system is unable to make the accommodations necessary for this new way f dealing with and interpreting medical history at home, in the doctor’s office, and in the in-patient setting.
From my Pinterest slides on this topic
Recommended Searches to review:
https://www.google.com/search?num=20&espv=2&q=unani+altonen&oq=unani+altonen
https://www.google.com/search?num=20&espv=2&biw=1580&bih=840&q=islamic+epilepsy
https://www.pinterest.com/altonenb/international-health/
