Over the past few weeks I have been ranting about the fact that the current managed care system has advanced little over the past 10 to 15 years. In fact, the first articles on the barriers to developing an electronic medical records system so essential to the managed care environment were published fifteen years ago. Today, many of these problems remain. The only thing that has changed is that information technology software programs and packages have improved, the amount of data that a data warehouse can store has increased significantly, and the speed at which ‘Big Data’ analyses can be carried out has improved substantially.
When you turn to the LinkedIn posting on IT, you’re left with the impression that this is a rapidly advancing field, with the ability to bring US health care programs to the next generation of due to progress.
Well, if you take a look at the accomplishments of most programs, you are more than likely going to see managed care programs still struggling to demonstrate success with their programs. Should this success be in the form of highly successful meaningful use measures, or important changes in population health features, there had better be a few of these “accomplishments”. After all, a typical program is evaluating between 50 and 150 metrics to document its accomplishments. Only some of these are reported. None of these programs (to my knowledge over the past 4 years) produces a thorough ‘Quality of Care’ or ‘Quality Improvement’ analytic program, measuring all or many of the accomplishments of the past years worth of healthcare efforts, and then maps the most significant of these findings. (Such is a reasonable goal, and product, for a HIT-GIS program.)
Knowing how to program your system to make such measurements is 90% of the work; its focus should be on the quality of care/quality of service (QOC/QOS) process for a majority of disease patterns in the region. The reasons such steps are not taken relate mostly to poor planning and administration. These processes could have been decided upon, planned, implemented, expanded and made more efficient in 2005, the year that the content of a valuable meaningful use program could be defined, a time when such a program referred to as a quality improvement [QI] program became a requirement.
There are several reasons managed care programs have not implemented a data warehouse setting in such a way that a spatial analysis technique can be applied, or added to an institution’s QI program with full scale implementation of a GIS.
First, there is no official policy or recommendation that was ever put into place for the implementation of spatial analysis techniques as part of a new meaningful use, quality improvement program.
Second, the skillset for implementing such a program is lacking at the leadership and administrative level. This lack is because directors, managers and administrators failed to hire the type of human resource needed to implement such an innovative program.
Third, even if individual exist in a healthcare system whom are capable of producing highly useful monitoring and intervention maps, the know-how for implementing a new program based upon these findings is also lacking, a blame we may once again lay on the administrators.
So meanwhile, as the Health Information Technology [HIT] departments at most institutions struggle to make old and new outcomes match, and develop a database that is not only consistent but highly worthwhile for monitoring managed care population health, it is best for those already working in their system to take on the next most important research question in managed care.
Can religion be used to evaluate population health, and if so, how do we make use of this unique form of datum?
Religion provides us with equally valuable if not more insight when compared with ethnicity and race data. Ethnicity can be used to search for social inequality and language related barriers involving the most predominant patient ethnic group in the United States. Race provides us with insights into how socioecononic status/poverty, and race and race-linked genetics can impact a populations health features.
What religion tells us can serve as a further clarification of race-related findings for illness and disease. Religion also adds to the insights we receive from the ethnicity work engaged in.
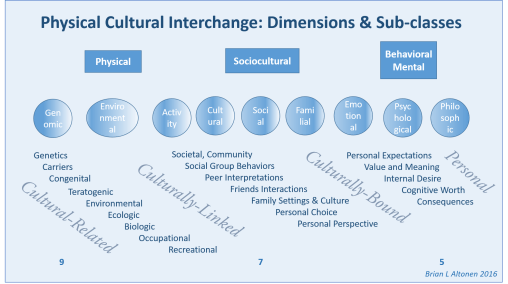
I have identified 9 physical science, 7 social science and 5 behavioral science and/or mental health topics that are closely linked to diseases and the medical disorders people are diagnosed with, in such a way that if these lists were related to the therapeutic processes engaged in for any ICD-defined medical/health state, the results of this interpretation of each ICD should enable us to define those which are most linked to a particular religious culture.
Elsewhere on the web, I have identified the various types of cultural disease patterns that exist, based on the current ICD systems. There are well defined culturally bound diseases, rarely mentioned culturally-linked disease patterns, frequently mentioned culturally-related health conditions and disease patterns involving the physical body.
Specific religious groups infrequently overlap with their disease patterns in United States cultural settings. There is the majority of diagnoses that are ubiquitous to population health, which individuals of all race, culture and religion experience. But there are also specific diagnoses and health problems that occur due to culturally-related human behavior habits. These are the topic of this review.
Using the standard research theory models, like Health Belief Model, to understand how people react to a medical condition, the above figure can be related to that model and the primary dimensions, subclasses and behaviors linked to a disease can be identified. Then a more effective and thorough intervention program may be developed and specifically targeted.
A “meaningful” managed care system assesses the entire population for all of its healthcare needs. This model enables planners to develop a balanced program devoted to physical, behavioral, mental and social care processes. It can be used to define when and where focus groups are needed, what populations to target with a survey, where to look for unexplored ICD related topics for you particular population, and how to improve the intervention planning process for conditions that aren’t effectively treated at the moment.
Consider each of these elements a question that has to be explored in order to fully understand the causes for certain non-physical, behavioral, social and cultural behavioral disorders and/or disease patterns.
