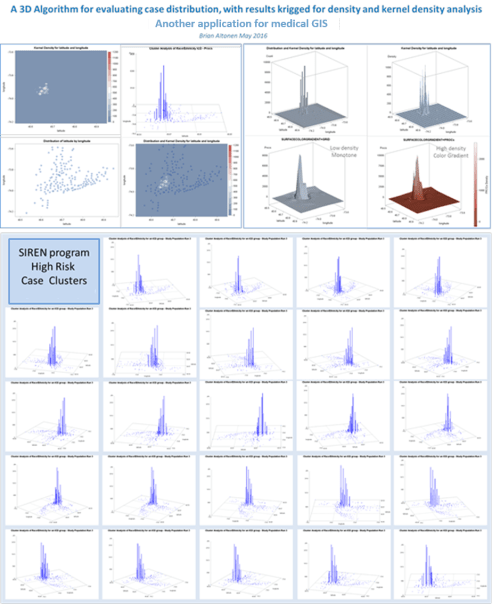
Genetic Disease Carriers, for a very common malady within a heavily populated urban setting. Note: this was not performed using a GIS, but a simple set of SQL-SAS algorithms
Fortunately, technology does catch up with some of the programs I write. One of those programs in the combined SQL and SAS needed to automate reporting for managed care companies.
The limiter to producing an automated ‘MAPP’ Program, as I call it (Mine-Analyze-Produce-Present) is the amount of work you put your system through.
My first attempt to go through this process entailed a production of about 3500 popualtion pyramids for most of the major ICD9 disease classes, many broken into specific age groups, in order to determine the highest risk gender-age groups in one year increments for very special social disease patterns, such as anorexia, wife beating, pyromancy, infibulation, and the varous forms of child abuse. This evaluation took me nearly a half-year to complete, b ut inspired me to automate my processes some more for producing more effective products, more quickly.
My second attempt entailed evaluating regional disease patterns. To accomplish this, I broken the US down ultimately into about 25 regions. It seemed the NCQA, NIH, US Census and USGS ways of breaking the US population and states down into regions, based on income and/or expeditures and insurance related patterns, wasn’t exact enough to demonstrate the varying family sizes I noted for unique areas, in more unique parts of this country. The Midwest and Great Lakes areas for example, I divided into north-south and east-west and combined N-S-E-W quadrant patterns to determine where the most statistically significant differences existed across state line/regional or subregional borders. That project fortunately took only a week or two to perfect, and led me to develop the grid mapping of the entire United States, in detail.

Over the past five years, the status of Medical GIS as practiced within the Managed Care profession has remained at a 5.50-5.75 level. We don’t use GIS to improve our HEDIS results, nor event to routinely monitor the HEDIS requirements, or event the Obamacare “Meaningful Use” requirements. There are numerous programs underway to try to convince managers to implement some form of spatial monitoring process. But due to disinterest, and/or lack of knowledge for this form of research and exploration, this more productive form of Health Information Technology (HIT) management has not become a standard part of any managed care system. It remains, in what I like to call, an “Experimental Use” category for HIT.
My grid mapping algorithms begin with the zip code mapping style, in which two kinds of maps are developed. The first is a raw data related zip code choroplethic or 3D columnar like demonstration of where the distributions exist for each particular metric. These metrics are, like before, of diseases and disease groups based upon ICD9, but also included evaluations of human behavioral patterns like late refills on necessary chronic disease prescriptions, or incidence/prevalance rates for some of the more classical population based disease distributions.
My second way of 3D mapping uses the grid modeling, of one or more resolutions. I tends towards the “best resolution” models determined using standard comparison analyses of the ability of different grid cell sizes to cluster series of adjacent cases to each other, producing the best fit half-bell curve of smoothly changing frequency distribution half-bell graphs. Each have their values when used to produce 3D mapping of large regional health care statistics.
My recent years have been spent applying these processes to local disease mapping. In particular, larger urban areas were needed to test the models that were produced. This allows the cartographer to test outcomes, and then to quantify the utility of each process relative to the spatial-temporal distribution patterns of diseases or measured events. Some processes work incredibly rare on rare disease events. Some appear to be under representative of high density patterns, like diabetes, obesity, hypertension, atrial fibrillation.
The use of prevalence incidence metrics for the spatial grid modeling technique is still very important to work with. But in too many cases (about one third of the time), this traditional use of “rates” as determined by demographers, epidemiologists, and public health specialists to be the chosen method, are unrealistic and useless at the business level. It would be a tremendous waste of company money to direct your spending to the higher prevalence/incidence places, which some of these values relate to low population counts, not any true need to healthcare facility or products and care management development.
There are several essential ways to develop your EMR data for automating the managed care population health reporting process. With the proper use of macros, you can develop the programming needed to make these calculation processes happen. Most importantly, this methodology doesn’t require the introduction of new software and work station settings to the system.
Granted, these standards to evaluating populations will be around for a while, and unfortunately, they distract from the directions in which more effective evaluations need to be made. The standard Cognos, Sharp and other systems out there are productive, but too slow. These processes evolved from the processes I developed are a great deal more productive, and produce lengthy detailed reports, on a daily basis if you wanted.
In the past year, the following algorithms were developed, tested, utilized and produced into report-producing programming end products:
- Population pyramid and standard barchart graphical depictions, for detailing standard metrics (demographies, diseases, costs, savings per member, cost, predicted costs, etc.)
- Age-Gender Population Pyramid produced statistical comparisons of matched or comparable regions, for any health-related metric
- Race-Ethnicity defined grouped data and regrouped data (binomial grouped) differential analytics, per metric
- Religion and Health regrouping algorithm used to compared traditional and various non-traditional religion and religion-health profiling methods for evaluating areas, regions, neighborhoods, in relation to treatment patterns, refusal for care, disease outbreak patterns, and performance of preventive care programs.
- A method for defining the least healthy patients in any program or population
- A method for defining the most important (highest numbers, incidence, costs) ICD groups for a given population, based upon race, ethnicity, etc.
- A method for applying and then combining or merging the three major risk scoring formulas into a single population-area health analysis methodology, specific down to the 1-year age increments for assigning a risk score, for each patient, and then reporting the summary of these data at the age-gender depicting race, ethnicity, religion, regional, program-defined, facility-defined levels [8 x 3 x 10 x n1 regions x n2 insuranceprograms or insured groups (MCD, CHP, MCR, COM, etc.)].
- A method for mapping these data (numerically, or fraction/ratio related):
- institutionally
- facility or office/provider based
- by network types (MCD, MCR, CHP, COM, BCBS, Obamacare)
- by industry distributions (urban hierarchical modeling processes)
- by socioeconomics data, race, ethnicity, and religion
- by specific disease classes (ICD, V and E codes)
- by specific human behavior patterns (based upon criminal or consumer data)
- by potential investor types
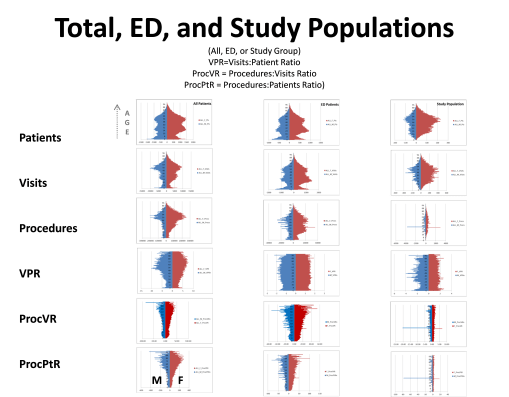
We expect some of what we see on the above diagram. As people get older, they potentially get sicker and require more care. Those who are the sickest experience increases in care related needs, relative to their number of chronic disease patterns. Visits include all visits to doctors, hospitals, labs, referrals, ERs, counselors, anytime you walk into a place and are billed for that visit. Procedures are actions taken by whom you isit, like your lab tests, your annual x-ray, PET, MRI or mammography, your routine drug levels screening for seizure control, your monthly drug urinalysis. VPR is Visits to Patients (per patient) ratio, per 1 year increment of age. ProcVR is the procedures to Visits ration; expected to increase as you get older and more procedures need to be peformed for more reason. ProcPtR is Procedure Patient Ratio, which is a product of ProcVR and Visits to Patient ration of average visits per patient, by age increments (1 year). The left column is for all standard office visit procedures; the middle column for Emergency Visits only; the third is of a population with a specific medical history using the ER for a specific reason. What is most important to note is the flate VPR that exists throughout the ER visits, relative to age. Younger people come in for different reasons, but that seems to balance out with the newer reasons that lead older people to come into ER for in order to receive care. The small spike at 0-2 years of age is for post-delivery problems, that often cause deaths in some children.
