What I consider the first book on medical geography, in terms of: i) a complete study of cultures, their differences, and distribution around the world, ii) medical and health related needs and natural offerings for disease prevention and cure, and iii) all of these in terms of time and place in the world. This actual book may be reviewed at Archive.org, or my page on it and the history of its author.
When I go through my site, and review its responses by the public (the world!) over the past few years, I cannot help but be amazed at the number of visitors interested in these subjects, as a learning experience. One of the things I have tried to remain humble too for the past two decades is how lucky I have been to tap into an unresearched or under-researched part of the history of medicine, that part pertaining to the culture and philosophy of disease, and how these vary around the world.
One of the more important lessons I had in all of this came from the religious scholars who speak of science as another philosophy, or way of explaining things. The philosophy of science is dualistic, in that it takes what is seen and define the other form or opposition to that thing and abides by the premise that these opposites exist. Since energy produces light for example, there is also this entity called darkness, when in fact, the reality of this scenario is that the absence of light is darkness, and darkness therefore is not a physical thing that must exist.
Now, it is important to note that this theory is found elsewhere in the writings–it is not my own. But it relates to the religious name for scientific beliefs called “scientism.” Scientism is the philosophical paradigm upon which all beliefs are based, in order that the best explanation of all that is found and seen can be provided. Since scientific observations guide scientists further, or in a new direction, that move then either reconfirms or cancels the ideology upon which beliefs are based.
On some of the earliest pages I wrote on this site about 8 years ago (for example, see my phenomenology approach), I summarized my teachings and discoveries of how and why medical beliefs change. Why is it that physicians were so convinced that they were right that they had to practically kill patients through the blood letting process? Why were such injurious processes as blistering, baunscheidtismus, the prescribing of purgatives, caustics, and emetics so important.
All of these “mistakes” disappeared once more proof as to a better way to treat such patients came to be. In my transformation of common belief , I argue that medicine survived mostly because practice and error were consistent, and that corrections always had to be made, the treatments had to be improved or made to be better. With success, we saw patients survive a health crisis, or become better, and/or live longer. With success, we dropped the older practices and substitute the new, until a still better belief and method complying with that belief can be discovered (see my anthopological cultural rendering of this recurring human behavior pattern).
Knowledge is the way to learn medicine, and my work on this site is to find knowledge not promoted much in the years before me. Unexpectedly, I found a lot of new concepts not yet taught in medicine, and was able to break the barriers that exist between the reading of historical beliefs and philosophies and relating them to the common themes that different cultures based their health practices upon. Many of the items posted on this page have never been posted or written before by previous medical historians, much less historic medical geographers.

Dr. Carl Friedrich Canstatt, whose book Handbuch der medicinischen Klinik, published in 1847 [in German], is the first book to provide a taxonomy of diseases that is based mostly upon environmental theories, including exposure to climate, chemicals, other parts of the human ecological settings. (I cover this book on this page.)
With that all said and done, I can report the following: several themes, topics and subjects continue to demonstrate popularity in the medical philosophy and history, and medical geography and spatial epidemiology fields.
The first is very popular to academia and the popular culture movements pertaining to alternative medicine, mind-body philosophy, and other cultural renderings or histories of health care and healing. The second is very popular due to the advancing fields and professions of medical geography, spatial epidemiology and research, and the rapidly growing GIS-guided research and professions, in the environment and health.
This first table is of the top 50 countries visiting this site and reviewing my information over the past 4 years. Some color coding is provided so the reader can follow the country across all four years. As expected, the United States is the top country to follow my posting on the value of spatial epidemiology, GIS and medical history. The United Kingdom, being the inventor perhaps, if not the most important influencer of spatial epidemiology and medical geography, is now second in terms of following this site, but is closely followed by its largest “sibling” Canada.
Canada is perhaps one of the leading countries in the world for use of unique spatial methods to evaluate the environment and the human impacted built-in urban environment. The U.K. is the creator of many of the ideologies we base our practices of medical geography upon.
The U.S. by the way is close to the U.K. in terms of its contributions to the fields of spatial epidemiology and medical geography. Were it not for the stubbornness of the early 20th century post-eugenics era scientists, and their pro-socialist sociologists and Marxists in the U.S transforming geography into two practices–environmental science and the controversial sociological alternative culture–the U.S. may well have excelled over the U.K. these past 75 years in terms of Geography field contributions. Our diminishment of “geography” from the pre-college programs and many of the colleges and university further diminished the roles of the U.S. in advancing the field of Geography; countering this were the U.S. contributions to Environmental Science.

Top 75 countries visiting my blog, per year from 2013-2016 (max number as of 2016 was 198)
Take a few minutes to let the variety of countries visiting this site set in. Medicine is a very hot topic worldwide. Many of the topics I cover are multicultural and crosscultural. Medicine itself is one of the most important topics for individual and group survival around the world. The skill of medical geography and mapping disease and health is equally important, at the worldwide level.
The unfortunate nature of the U.S. healthcare system is that it is making us fall far behind developing countries in how we utilize GIS and spatial health to the best of our potentials and ability. The fragmented nature of the U.S. healthcare system makes it difficult and almost impossible to produce a nationwide healthcare program, like other countries are now doing. That may be one of the benefits of socialized medicine in the decades to come, assuming our current HIT level remains stable and productive, and that is not hindered by political changes now happening around the world. An overtake of major forces, governments, ideologies, can have some drastic impacts upon the advances now being made in medicine, the internet, world information exchange, the iCloud, the use of medical and healthcare data to the best of our ability, in terms of fighting the health changes that may ensue in upcoming years.

E. N. Pavlovsky, perhaps the most important medical geographer and disease ecologist in Russian medical history, specializing (inventor of) in modern parasitology and the biology and ecology of vectored and zoonotic diseases (my introduction page on this).
This detailed review of the history of medical geography that I do is focused on the U.S. often, but is not exclusive of other countries, some more important than the U.S. is some parts of the history of this profession. The Russian medical geographers of the nineteenth century are not covered in any anglican writings in this field, which is a shame, for their theories in economics and ecology are in some ways better than those of western society.
In the following photography, the leader of Middle Eastern medicine up until the 1990s, Hakim Mohammed Said, made it a point that the ancient practices remain alive, practiced, researched, and documented. Globalization of health care can effectively makes many of these alternative practices extinct. The practice Said was most attached to was Unaniism, and its resemblances in theory to Hahnemann’s teachings of homeopathy. The political events taking place in the Middle East make some of the Iranian and Iraqian forms of practices extinct from common knowledge. Right now, parts of this medical philosophy and belief system are travelling the globe, and will soon be the next form of alternative/complementary medicine most of allopathy will be having to deal with, along with the health conditions attached to this philosophy of health (more on this at the end).
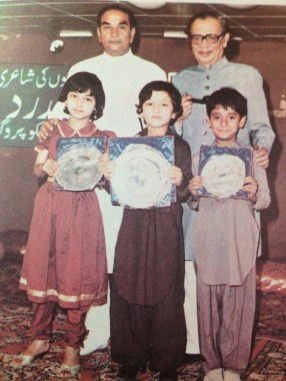
Hakim Mohammed Said (https://en.wikipedia.org/wiki/Hakim_Said)
Back to the history of medicine in the Americas, when the U.S. established itself following the Revolutionary War, U.S. scholars set the stage to become important contributors to the field of Geography during the first 125-150 years of the existence of this new profession in US culture and academia. Many of the teachings back then were quire different from those of the Western European leaders.
Most of the teachings that appear in the medical literature at the time are all accurate environmental renderings of disease patterns, and are directly applicable to the sudden re-emergence of interest in new diseases migrating into the U.S. from afar, and to the return of the old diseases that once were considered eliminated. To best understand the older disease patterns, we need to look at how they existed and were dealt with during their peak ages of existence. Contemporary medicine has not yet taken on that task of relearning its historical background and knowledge.
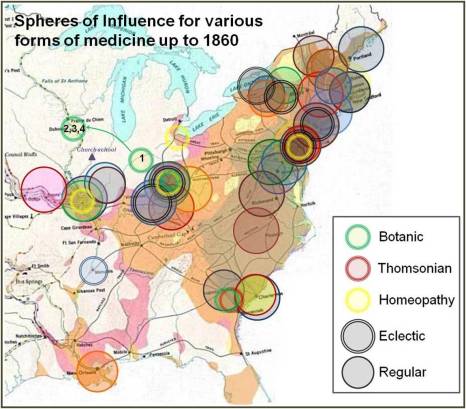
A very early project of mine, on the diffusion of allopathic and non-allopathic health professions in the U.S. from 1750 to 1860, based upon the establishment of medical schools and their geographic and political “spheres of influence.” (See my pages on this, Part 1 and Part 2,)
For examples of applications, review the maps I posted, many of which are the most important to medical geography history. Some of them are basic maps that we immediately understand. Others are maps that we wish we had continued to work on, so as to perfect this skills by today’s day and age, for now we are more than a century behind in this knowledge based, and back to beginner’s level for the most part in trying to implement the same exploratory processes.
The U.S. experienced the first large area, large distance diseases to travel expansive waterways between continents, and to demonstrate quite clearly that there were latitude and longitude differences regarding disease behaviors and distribution.
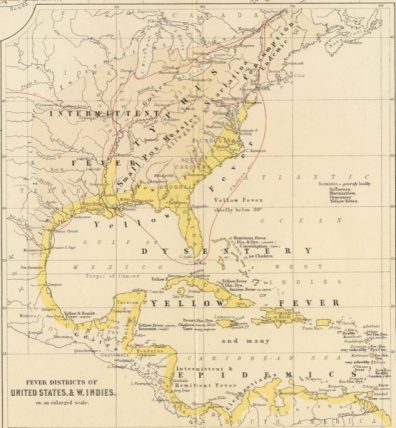
Yellow Fever Insert of Alexander Keith Johnston, 1856 (See https://brianaltonenmph.com/gis/historical-disease-maps/alexander-keith-johnstons-famous-map-a-detailed-review-1856/)
The yellow fever outbreaks of the post-Revolutionary War years into the early 19th century were at first puzzling (“The Extraordinary Disease at Martha’s Vineyard”), but later better understand and gave rise to the development of the quarantine policies for incoming ships.
The cholera had stricken Western Europe a number of times, and European geographers were able to develop some very important hypothesis regarding spatial disease spread behaviors and patterns. British epidemiologists developed the models claiming disease spread patterns were in part due to populations, but perhaps more so due to living style, the distribution of poverty, and the practice of poor sanitation. United States geographers developed the models relating disease to urban density and what may now be called hierarchical diffusion patterns for disease transmission, an ideology re-invented in the 1960s by a U.S Economics Geographer.

Top sites people visited
Notice, the 1890 Census Medical Geography has surpassed the page with my personal information, an important change in the pattern of use of this site.
More important perhaps is the fact that geography and my review of geography as a historical medical geographer are now contributing greatly to fields other than healthcare, epidemiology and medicine.
Native American, Indigenous culture and philosophy, and Indigenous health are teachings that stand out on my site. The immediate popularity of the fairly thorough work I did (from 1990-1994 about), on Chicle and the Chewing Gum industry is probably due to the large numbers of classes in the U.S. with Hispanic students and teachers wanting to find important topics that portray the contributions Hispanic cultures made to the history of the U.S. The late 1800s map of Mexico’s disease patterns and the regionalism of disease patterns is an important example of how we developed our “deterministic” philosophies during the late 19th and early 20th century (the eugenics period).
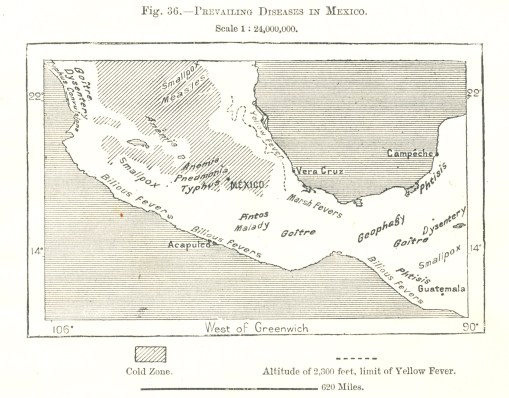
A map of the diseases of Mexico, from a World Geography set ca. 1897. The history, meaning and anthropological, cultural interpretations of these diseases and their distributions is extensively reviewed at my page on this map’s history.
When I began teaching in 1988, in fact, my goal was to point out the firsts in American and U.S. culture. This included the first uses of Native American philosophy for medicine, the first use of a U.S. plant for the more modern 19th and 20th centuries western European pharmacy, the first time we reviewed natural causes for diseases outside the human body, aside from temperament and inheritance.
I was also fortunate enough to uncover evidence for the first Jewish MD physician and doctor in the mid-Atlantic (New Amsterdam/New York) part of the North America–Dr. Isaac Marks. Researching him as part of the Revolutionary War doctor’s manuscript (Dr. Cornelius Osborn) that I re-discovered in 1981, opened the door to understanding and demonstrating colonial interpretation of the American Indian philosophies, and their willing to engage in new versions of older theories like alchemy in the New World, as the predecessors to understanding human emotions, spirit, emotions, and psychology (Harvard’s 1650 Charles Starkey‘s practice of this and its parallels with the Dutch (and thus New Netherlands) preacher and professor of medicine/mindbody effects–Hermann Boerhaave).


The first medical geographers
Disease mapping is also a major topic of interest now to medical history and geography students. The first disease maps came from the United States (although I wouldn’t be surprise if somewhere we do find some European mapper producing something like this in a manuscript collection). The local New York City patron of medicine in the field, Dr. Samuel Mitchell, published this country’s first article(s) on “medical geography” and may in fact be the first to popularize, if not both publish and popularize, this term.
The U.S. doctor next in line for the U.S.’s fame in this field is Valentine Seaman, of NYC, who produced the first epidemiology map. using it to explain the recurring seasonal yellow fever outbreaks in lower Manhattan. No one was in the famed city of Philadelphia was like Seaman or Mitchell, including the famous Benjamin Rush.
Benjamin Rush, however, did introduce to us other important “discoveries” and additions to the field of medicine, thereby distinguishing it completely from the medicine practiced in Great Britain. He produce the precursor to the idea that as land use patterns change with time, as will lifestyles and disease patterns. Rush didn’t take it as far as health and diseases, but managed to at least defined the impacts of land use changes upon the occupations and lifestyles of people surviving in different regions, ranging from farming communities, to villages and small town and larger cities.
Benjamin Rush and his important article proposing a sequent occupance type model is available for review on this page.
With this, Rush provided the medical geography field the first example of a use of an ideology that would later be reborn again by midwestern U.S., helping scholars imagine and publish the sequent occupancy idea.
Although never related directly to just health and disease patterns, sequent occupancy was the preliminary idea that was born again later under the term epidemiological transition.
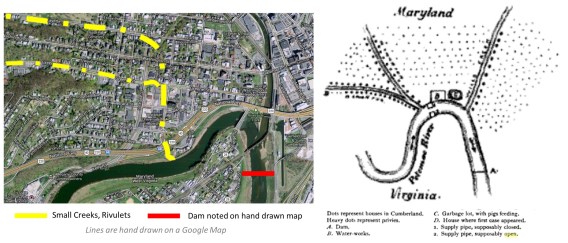
How the contamination of Cumberland city water happened by the seepage of waste from barkyard privies and city sewage overflow into the Potamac river, as revealed by Dr. William Wyett Wiley with the quickly handrawn map (right) subsequently published in a medical journal. [From one of my pages on this.]
For geographers, the sequence of change was popularized in 1890s (Derwent Whittlesey [professional obituary]), but then forgotten. The temporal-spatial disease diffusion process was explained and popularized with models published by geographer Gerald F. Pyle in the 1960s, and promoted further by his 1979 book “Applied Medical Geography”.
In 1832, Cholera entered northern North American via Canada and the St. Lawrence Seaway, impacting inland cities like Quebec and then almost immediately migrating southward to New York City by way of heavily travelled water routes. This introduction of cholera by way of major heavily populated places was first published by NY Medical Geographer Lewis Beck (Report on Cholera in Canada and New York, 1832). This hierarchical diffusion path was duplicated 150 years later when Ebola was introduced to North America for the first time about a decade ago, this time by airplane.
For epidemiologists, epidemiological transition is linked mostly, or only to scholar Abdel Omran, conceived in the late 1950s and 1960s, as part of the Columbia University school of Public Health, but not popularized until 1971 (see my page on his study as it relates to Native American epidemiological transition). Several attempts have been made to modify the Epidemiological Transition theory, to better fit the changes over time and new observations being made, but the sequent occupance model remains a more valuable and precise interpretation of changes in disease patterns over time and space.



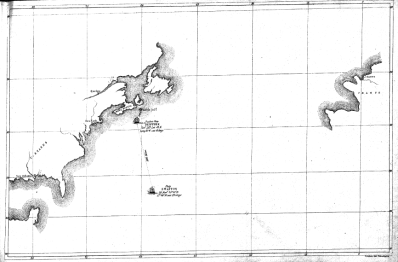
The first map of disease by Valentine Seaman, Yellow Fever outbreak, NYC, ca. 1798/ mapped by its 1803 publication date; part of the first Medical Charts series ever produced, used for defining insurance payments, by Sydney H. Carter’s Insurance Company in NYC; three examples of the first disease maps published in the 1890 U.S. Census (area highlighted was reviewed for one of my studies posted on this site).
The ways in which medical geography can be directly related to epidemiological transition theory, through the sequent occupancy model, are defined in my thesis (posted by itself and the theory discussed briefly on several pages at this site).

The present state of utilizing GIS for surveillance by the U.S. managed care systems.
We remain at this level, although I am inclined to prepare for changes in 2017. Once evidence is published for use of GIS in ways other than “descriptive”, the medical profession will be heading into the next generation of GIS use, as an analytic tool.

Famous medical geographers
There are several medical geography topics that are going to become increasingly important in 2017.

#1
Islamic culture medicine has to be further investigated, with an emphasis on Unani and non-Unani medical practices. We are provided more information about the practice of Unani medicine through the Muslim India internet sites, than through Iranian, Iraqian sites–the two philosophies do demonstrate some important subjective, cultural differences (which I must cover later).

#2
The impacts of Islamic practices (Unani and non-Unani, Sharia Law practiced) in the Middle East, on people migrating to the U.S. is going to have a profound financial and cultural impact on the U.S. health care system. Some legal impacts may be experienced and become problematic as well. The three most important issues uncovered to date are: infibulation (female circumcision) history and practice and its practice on children under 18 years of age, and especially under 9 and under 5 years of age. The younger the patient residing in the U.S., the more likely she will have received this practice while living in the U.S., by a U.S. MD or non-MD practitioner, including the use of methods practiced in some very “crude” ways (“broken bottle process”).

#3
The Obamacare PPACA plan may change or even go away, but the need to demonstrate cost improvements in healthcare will not. If the current PPACA is changed, disenrollment and increases costs may drive up epidemiological problems once again; without the development of spatial GIS methods in the American healthcare systems, we will certainly experience more unpredictable disease outbreaks, in lower income areas and in the form of in-migrated disease patterns.
#4
The BD2K (Big Data to Knowledge) plan now being initiated in health care–making available, testing, sharing and employing these larger datasets to develop more comprehensive population health research programs–will cause radical changes in the system, regardless of the program that exists. Insurance programs, if they continue practicing unengaged irresponsible, non-forward thinking healthcare practices, will ultimately lose their trustworthiness and integrity. The application of GIS to healthcare is one of the most time-saving methods for analyzing BD2K data thoroughly and completely, reporting the outcomes frequently.



#5
The numerous “genomic plans” developed to improve genome centered healthcare practices must be performed along with an equal number of “epigenomic” programs, designed to focus on the environment, neighborhood, people and health. This can only be performed using GIS or some form of Spatial analysis routines.
#6
Spatial analysis provides more accurate ways to analyze healthcare statistics. The hexagonal grid model I developed is 27% more accurate than traditional grid models. It produces smoother more realistic 3D modeling results, and is the visualization tool that must be utilized by the public medial geography sector to produce more accurate results, more rapidly than through the use of traditional modelling tools already in place.
***********************************************************************
