NOTICE!!
If you work in a company, industry, or academic setting and know that GIS or spatial analysis is a part of the requirements for your company or workplace…the following applies to your occupation.
A Survey has been developed to document and compare GIS utilization in the workplace. This survey assesses GIS availability and utilization in both academic and non-academic work settings. The purpose is to document the need for GIS experience as an occupational skill. GIS is currently being underutilized by most companies. Spatial Technician and Analyst activities and a few managerial activities requiring GIS are reviewed.
This survey, which takes about 20-25 mins to complete (@25 questions), can be accessed at
Survey Link
……………………………………………………………………………………………………
(c) 2006, 2010 Brian Altonen

Seeing the Elephant
To “see the elephant”, in American history, is a phrase often used to imply that you have experienced or witnessed everything possible by the time you’ve reached a certain point in life. This phrase, common to mid-19th century writers, is much like what we mean today when we hear someone say in just the right tone “Now, I’ve seen everything!”
During the late 1840s and very early 1850s, this phrase became common place in the Midwest. At first this was due to its association with traveling circus shows, but as time progressed, applications for the term ‘elephant’ changed. One day, for example, in the town of Carthage, Illinois, a circus made its way through the central part of the County’s town center in May of 1852. Soon after, Asiatic Cholera struck the city and its hotels for the first time, taking thousands of lives over the next few weeks as this disease was spread into in the various towns situated along the local roadways and the Mississippi River.
As caravans occasionally made their way into town, with circus players settling the nearby hotel rooms and residing in tent cities, one rarely had the opportunity to see such a thing as an elephant as one of the main events. For this reason, ‘seeing the elephant’ had very little to do with the animal itself, and so, for the most part, children and parents relied upon the books to learn about these beasts. It wasn’t until these families had the opportunity to travel to one of the larger state fair establishments, that a true elephant, lion, or even camel could be seen. So, in spite of the commonness of this term ‘to see the elephant’ in American history, this phrase more often referred to the numerous public health crises that developed over the years due to poor sanitation, poor living conditions, malnutrition, lack of exposure or immunization regarding any newly introduced diseases making their way by ships. This is just interpretation of the phrase ‘to see the elephant’ in public health history.
Another much broader meaning of the phrase ‘to see the elephant’ is a more traditional interpretation of philosophical meaning of the ‘elephant’ in the history of mankind. This more ancient, philosophical has much broader applications than the midwestern meaning for this phrase. The more traditional ‘elephant’ eluded to with such a phrase pertains to the famous story of several blind men trying to define the elephant that stands before them. A well-known poem, “The Blind Men and the Elephant,” by John Godfrey Saxe (1816-1887), underscores just how fragmentary knowledge can be when it is produced by scientists.
.

.
This is especially true regarding the work of epidemiologists, who take numerous steps along numerous avenues of research in order to define, as best they could, the health of a given population. This synopsis of population health is a results of each other’s studies and a review of how each of these studies support and corroborate other similar studies engaged in at numerous levels within a health care system. For population health epidemiologists, the term ‘elephant’ very much defines what it is that these researchers are trying to measure. Epidemiologists work at various levels to better understand the health of a population. When it comes to applying these findings to population health in general, this process is much like several blind men standing around an elephant, providing their own interpretations of the observations they completed about the form, shape and meaning of their individual findings.

The current methods that exist for interpreting population health are performed based on a number of very different methodologies. When we read about the results of a particular study performed at some university or teaching hospital level, or learn something new about the possible causes for increased morbidity and mortality in a particular subclass of people, or find a study suggesting a new line of reasoning about how to prevent contracting an infection or experiencing cancer, we unknowingly may be essentially just re-interpreting the conclusions of these researchers, based on just a small part of the overall picture about population health. Were we to base our lines of reasoning on just the few warnings and fears published by such researchers, we could miss some of the other important components about population health still out there for us to discover and learn to make the best use of. For this reason, all possible avenues for reviewing population health have their own individual roles and purposes.

(Click on above image to enlarge, and to read the fine print)
One level of analysis pertaining to population health that has yet to be fully realized as a potential source for public health knowledge and understanding, pertains to the best use of prescription or drug data. The above illustration demonstrates the levels of data that are already out there for use in population health monitoring practices. Quite a few methods for analyzing population health are in place, and engaged in as part of an ongoing process of measuring the overall performance of the health care system and its various components (insurance agencies, hospitals, doctors, patients, etc.). The level between Federal or National programs and large-scale institutional or agency level programs is a level that is not yet heavily employed as some part of a public health monitoring system, a level one step above our major method of researching such information and reporting our outcomes (in yellow)–the Corporate level (MegaRx and industries) (Hint: click on these images for enlargement and to see the details).
To take a much larger additional look at the ‘elephant of public health’, we have to come to any understanding about what is already out there that is being told, and what avenues of research are still available for engaging in the population health monitoring process. Currently, we make use a number of research methods to engage in public health studies. The following levels of health monitoring have been identified for developing a program design to review a particular population at the level that we are independently capable of and so desire. These levels are defined based on the ways in which individuals and people learn about health practices and performances, and then chose to engage in these practices in some fashion, so as to impact personal and/or population health. Note that for this particular review, a new level of engaging in modified behavior model practices and activities is being introduced–the engagement in this process at the large-scale institutional or corporate level. This level of involvement has only surfaced in recent years as a possible method for measuring population health. The ability to engage in this method of monitoring health, and health practice/health education, has surfaced due to the ability of major service providers to merge their corporate information to such an extent, that large databases have been formed with endless amounts of data pertaining to individuals, groups and overall population health. 
At the community level, this possibility of researching population health has come about due to the mergers formed whenever various facilities serving a fairly large but interconnected area in the state decide to combine their services and activities and form a large regional organization, as a part of which, much larger and interconnected databases begin to emerge. At the corporate level, these large databases are formed as a result of large and small buy-outs and the ultimate conglomeration of data that takes place within these megalopolis public health and medical service settings. Traditionally, it is at this level that the least amounts of health conscious work have been performed in order to monitor and change population health. This is largely due to the limited “power” these institutions have in the various fields of medicine and pharmacology. They are for the most part passive observers, meeting the needs of a fairly large consumer population, who in reality can only have a minimal impact on the health care system as a whole. These corporations do not make diagnoses. They do not define the policies for determining how to best treat a patient. They do not produce guidelines for how to best engage in specific health care related practices such as defining the most reliable lab test to perform or drug to be administered. What these corporations do have on their side is their ability to perform larger reviews of data and outcomes retrospectively, at a level and size that few other research groups are capable of performing. The purpose of providing these outcomes may have traditionally been economically driven, with the goals of reducing average costs and saving money on a per patient basis, but now has the additional ability to be employed in such a way that it more than adequately complements those processes that are already in place for measuring population health and program success, with an ability to add new measurements techniques and steps to be taken in order to provide valuable input into the system as a whole. This latter accomplishment is in fact the reason for this review, and will be discussed following a review of methods already in place.
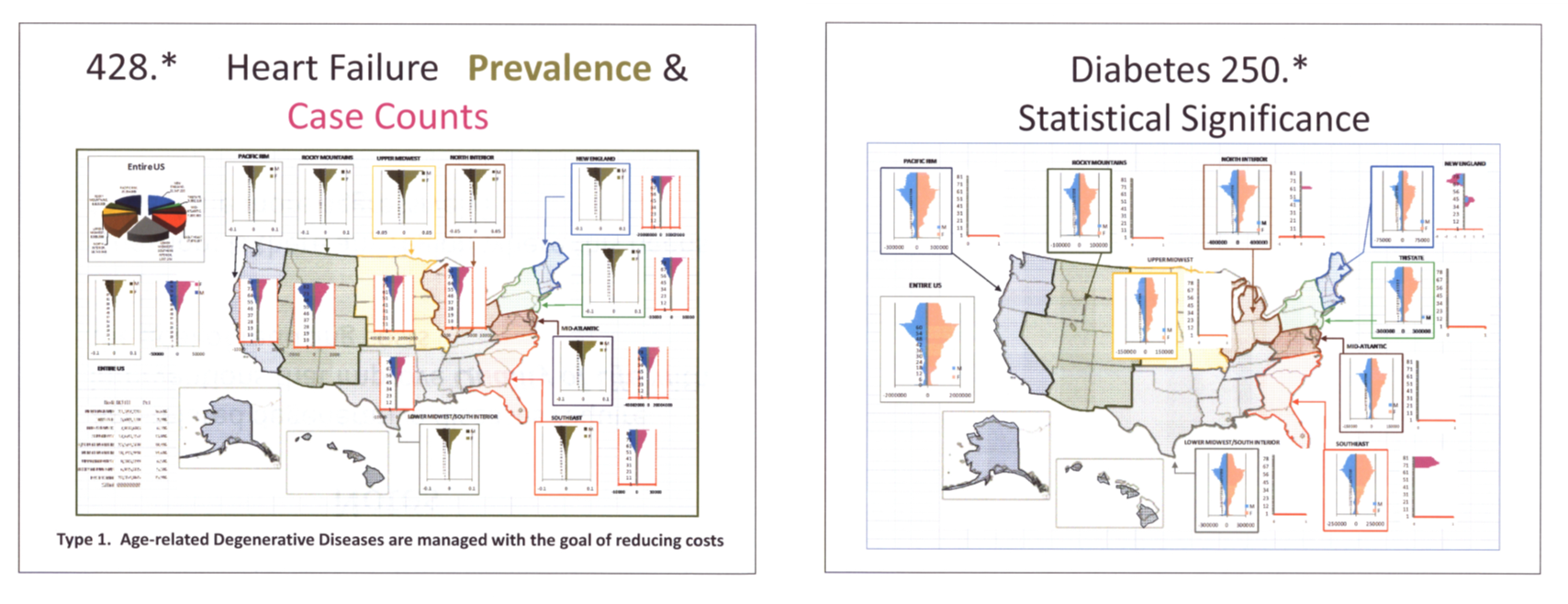
Comparing distributions for two of the most common chronic diseases: heart failure and diabetes. Case counts (pink-blue, M=left, F=right), Prevalence (dark and light brown), and Relative Stat Sig (dark pink, dark blue) are mapped in population pyramids format, evaluating ages grouped using a “moving window” 5 year age range strategy calculated along the entire y-axis. This method tested on more than 1000 ICDs, some with subgroups added. [ca. 2005/6]
Current Population Health Measurement Methods
In general, there are several methods in use when reviewing population health. We can define the degree of impact that a particular health education lesson, healthy behavior or disease-inducing pattern has on people in general. We can also use some sort of standard sociological method of defining these different levels of impact, working out way from the smallest groups–the individual–to the largest group–the total population, defining various strata along the way such as family, extended family, associates or friends, local community, town, county, etc. until the total country or world population level is reached. In addition, we can place more of an emphasis on the routes of communication that exist between health-related lessons or disease-related patterns of pathogenicity, using this to demonstrate how each of the different types of individuals become more aware of health and disease. We can also apply to this methodology a review of the various levels of health care that are available, determining whether or not a change occurs in population health due to the activities of physicians, or the activities of an institution or health care insurance program.

Results of a study on one-fifth of the US population, ca. 2006, for Anorexia the syndrome vs. Anorexia the symptom, pointing out the regionalism of health statistics and the use of a hybrid format for mapping based on Census and HEDIS definitions.
These various methods of reviewing ‘the elephant’ also provide us with whatever insights are needed to produce a much better ways to monitor that which is already in place. We can then add to this system by designing new methods to measure and interpret any impacts these changes have on human population health in general. With the exception of Level 7 above, there are a number of methods currently in use for monitoring each level of the health care system as noted above. Many of these activities pertain to such matters as accreditation and quality assurance. Some are simply internal studies engaged in due to other institutional requirements, such as the production of an end-product for a grant-sponsored project or the development of a final report used by the research group to continue the flow of incoming financial support. For this reason, we find almost everything that is monitored has both internal and outside organizations engaged in this process. These outside agencies are typically related to either the reaccreditation process itself, or some specialty group involved with this process for the purpose of making sure the program being reviewed is trustworthy and reliable in terms of the quality of its medical care. It is not unusual for fairly large health care systems to undergo numerous interactions with governmental organizations, special interest groups, and even npo’s in charge of monitoring certain aspects of population health and health care outcomes. We find some agencies to be engaged in monitoring just the process of administration, with limited concern for the outcome and more attention paid to such things as abiding by specific rules or protocols for treatment, or remaining efficient in terms of administration and billing practices. Still other agencies pay close attention to the system as a business, reviewing income activities and behaviors, at times even searching for ways to cut costs when it comes to managing the program being reviewed.
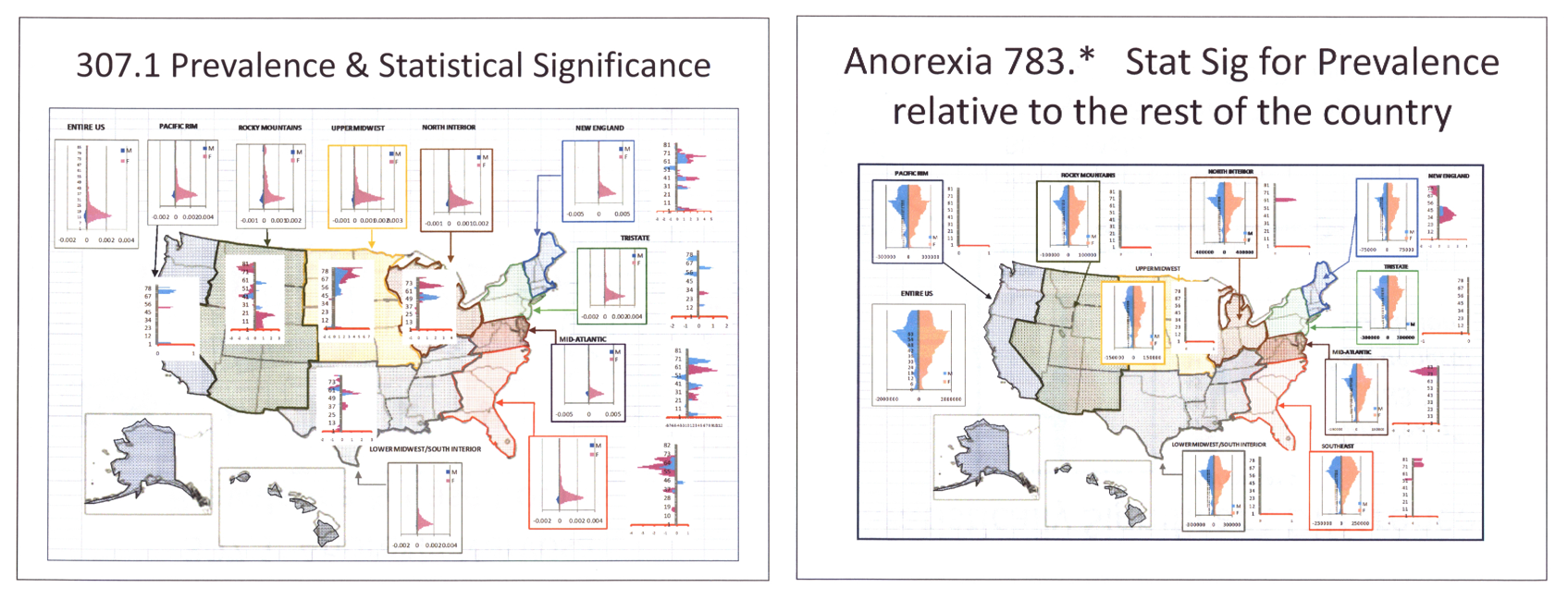
Anorexia as a syndrome or psychological/psychiatric disorder, versus as a symptom–the impacts of age on regional differences in prevalence
For public health and epidemiological work, there are several levels of epidemiological surveillance that can be related to the system as a whole and the population of the people as a whole. The following explains these levels of review, as they are interpreted for this study.
The Traditional Tetrads of Health

When we are asked about how we engage in health maintenance and our visit practices without health care providers, we typically think of just two things–ourself and the main doctor or health care provider whom we visit (or at times lack). A few seconds later, we then realize the other services were are receiving related to health, ranging from allied health care providers and agencies outside the typical physician’s office or hospital setting, to the insurer or types of payment programs we like to rely upon to pay for our care. This tetrad of features forms the base of most personal health care systems. Some of the elements are there just during certain periods in life, such as when we can afford them or are working at a place where health insurance is made available, others we use throughout much of our life, such as dietary and exercise practice changes taught by a popular health guru and methods of dealing with and preventing diseases that we learn about from our family, friends and associates. In the professional sense, we rely mostly upon the health care system with its accredited service providers (both regular and complementary health providers) to receive the bulk of our most important care, that is assuming the need for such arises.
Most people purchase medications from a pharmacist (although we could include TCM and ND “pharmacists” into this part of the story as well), whom we tend to interact with on a fairly personal basis, Although there are health care systems that we can interact with that have a pharmacy available on premises and part of the Institutional Healthcare Provider network (IHP), we tend to make use of some sort of outside provider as well. This adds another component to the web we are now weaving, all for the sake of personal health.

(Click on above image to enlarge)
Another level in this system (or part of the elephant) can be defined for the agencies that oversee these service providers. These are the agencies which monitor their practice behaviors to ensure that we are receiving some sort of care that meets specific standards. Some of these agencies are higher up on the totem pole of progress in this method of health care monitoring, with those situated higher up usually more often related to better performing programs. For the most part, these agencies or offices/programs exist to ensure adequate health care procedures and “sufficient” medical practices.

(Click on above image to enlarge)
Usually we are also familiar with some standard overseer and education facility monitoring the activities of the health care system we are a part of. Within fairly rural settings, the association with such a facility is much harder to see any evidence for, and for the most part may never exist as an active part of the local health care system. The people in these settings tend to remove to a more heavily population area to receive the special services provided by such institutions and their care givers, of take advantage of caravans passing through that offer free or reduced services to these rural settings. Most of us, however, are fairly familiar with the medical education system, its interactions if any with treatment facilities and any additional services if may provide that need to be taken advantage of. This system includes every things from small local care centers serving as clinical sites to the much larger conglomerate such as regional professional groups overseeing the local drug prevention programs being provided, npos targeting teenage girls at risk for pregnancy, or health education organizations with a local office used to produce local classes on CPR and first aid.

(Click on above image to enlarge)
A number of other services and agencies are added to this system to produce a fairly complex relationship used for the development of large programs meant to serve large population groups. The two remaining components that can be added to this system are the large-scale international or electronic-processing providers for prescription drug services, and the various forms of health education service providers that exist outside the traditional university/medical school setting. These to groups are, generally speaking, For-Profit agencies with good intentions in terms of public, community and institutional or agency-related health, but they are also consumer-minded businesses with goals related to both internal progress as well as improved population health outcomes.

(Click on above image to enlarge)
In a fairly recent article published reviewing the impacts of “For-Profit” status on values at the population level, it was demonstrated that large corporate level programs tend to have better programs than institutional or university driven programs, in terms of content and quality. A few of these may be in violation of certain HIPAA regulations should they not engage in adequate internal policing when it comes to maintaining human privacy related issues at a corporate level.
Measurement Tools and Programs
A number of programs are in place for measuring health performance at nearly all levels, ranging from small special service agencies to national and federal accreditation programs. The following are examples of the various programs already in place that are used to monitor health care services at each of these levels within the health care system. The first examples are of programs that are for the most part initiated and engaged in internally. Once the regional and federal level of monitoring is reached, these programs are primarily for evaluation and accreditation purposes.


(Click on above image to enlarge)
Other Pages in this Section – “Seeing the Elephant – Part 1”
- The ‘Elephant’ and the flow of information
- Part 1 – Measuring People and Health
- Part 2 – A Study of Asthma Risk and Preventive Care
- Part 3 – Defining and Representing Research Populations
- Part 4 – Making the Best Use of your Data Sources
- Part 5 – HEDIS Measures
- Part 6 – Non-HEDIS Measures
- Part 7 – HEDIS Evaluations
- Part 8 – PIPs and QIAs
- Part 9 – Traditional Baseline Measures
- Part 10 – New Baseline Measures
- Part 11 – Balancing your Evaluations with HP 2010 and other tools used to define New Indicators
- Part 12 – Examples of Applications
- Part 13 – Developing the Final Report

The above view of Heart Failure diagnoses defines regions based on Census and HEDIS/NCQA definitions, combined to produce smaller regions in certain parts of the country. In the prevalence population bars, movement to the right indicated greater than the national averages for that age group, with age specific rates analyzed in one year increments. Movement to the left means the national average is greater than the regional average for that age range. In the above example, the SE section shows significantly larger prevalence in the older age, which is expected for the Florida region. The section of New England demonstrates a peak in heart disease at the older working age level; this implied the working class in this region have a greater risk of heart disease than those to the south, such as in the NY-PA-NJ tristate or Mid-Atlantic regions. The healthiest old age population are found in the Pacific NW and the northern Rocky Mountains regions. The localization of this health is missed when we define these two regions using the traditional NCQA and/or Census region definitions, as in the above map. A grid method was developed soon after in order to produce a much more locally sensitive method for mapping regional public health data.
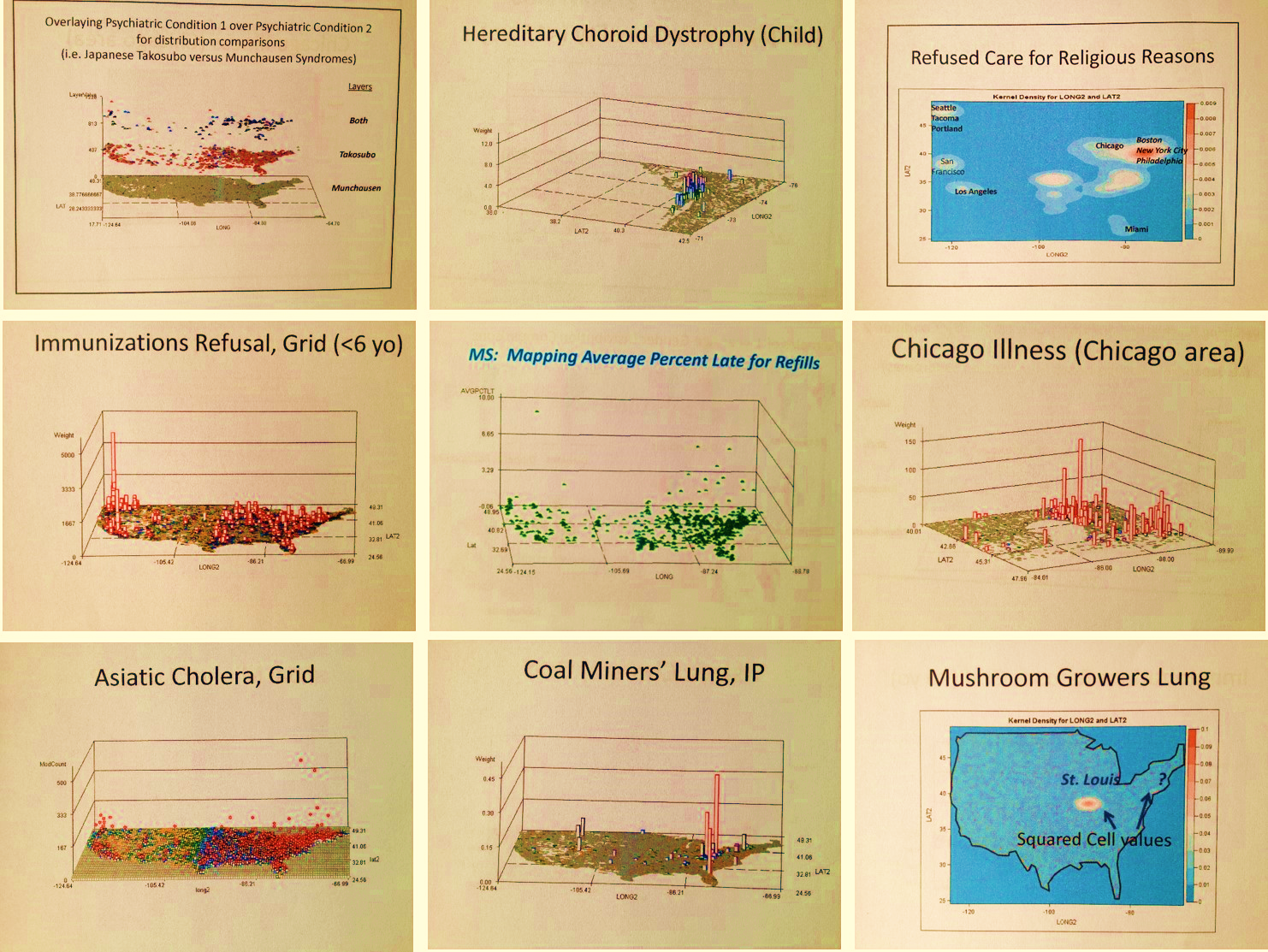
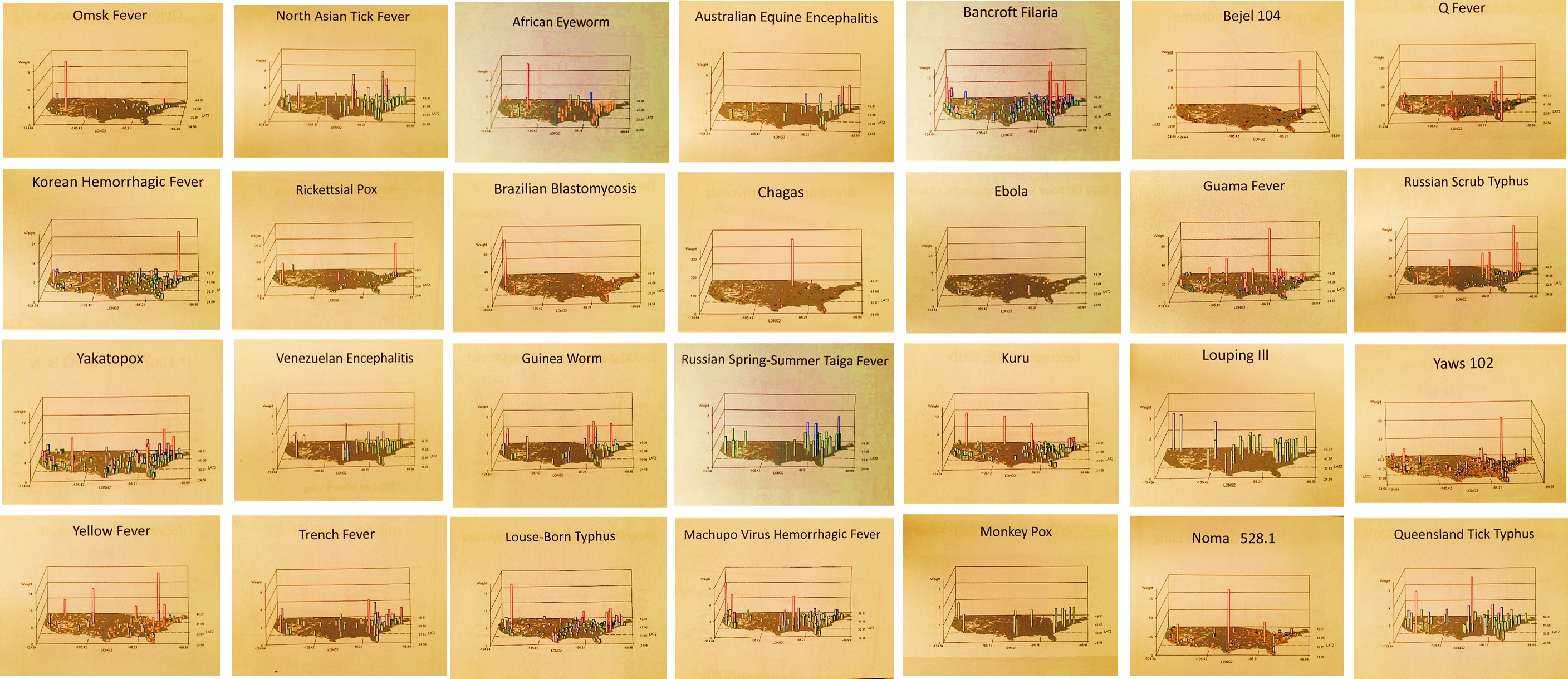
Note: This project came about in 2004/5 due to a request submitted to me by two NIH funded and contracted IT firms devoted to infectious disease monitoring. Their work focused on disease migration and surveillance, evaluating bioterrorism and agriterrorism risk, and related this to national public health needs. This project later evolved into my National Population Health Grid Mapping Program measuring disease rates across the country at a 25 x 25 mi gridcell level.
Examples:
 Regional and Local Health Concerns
Regional and Local Health Concerns
.
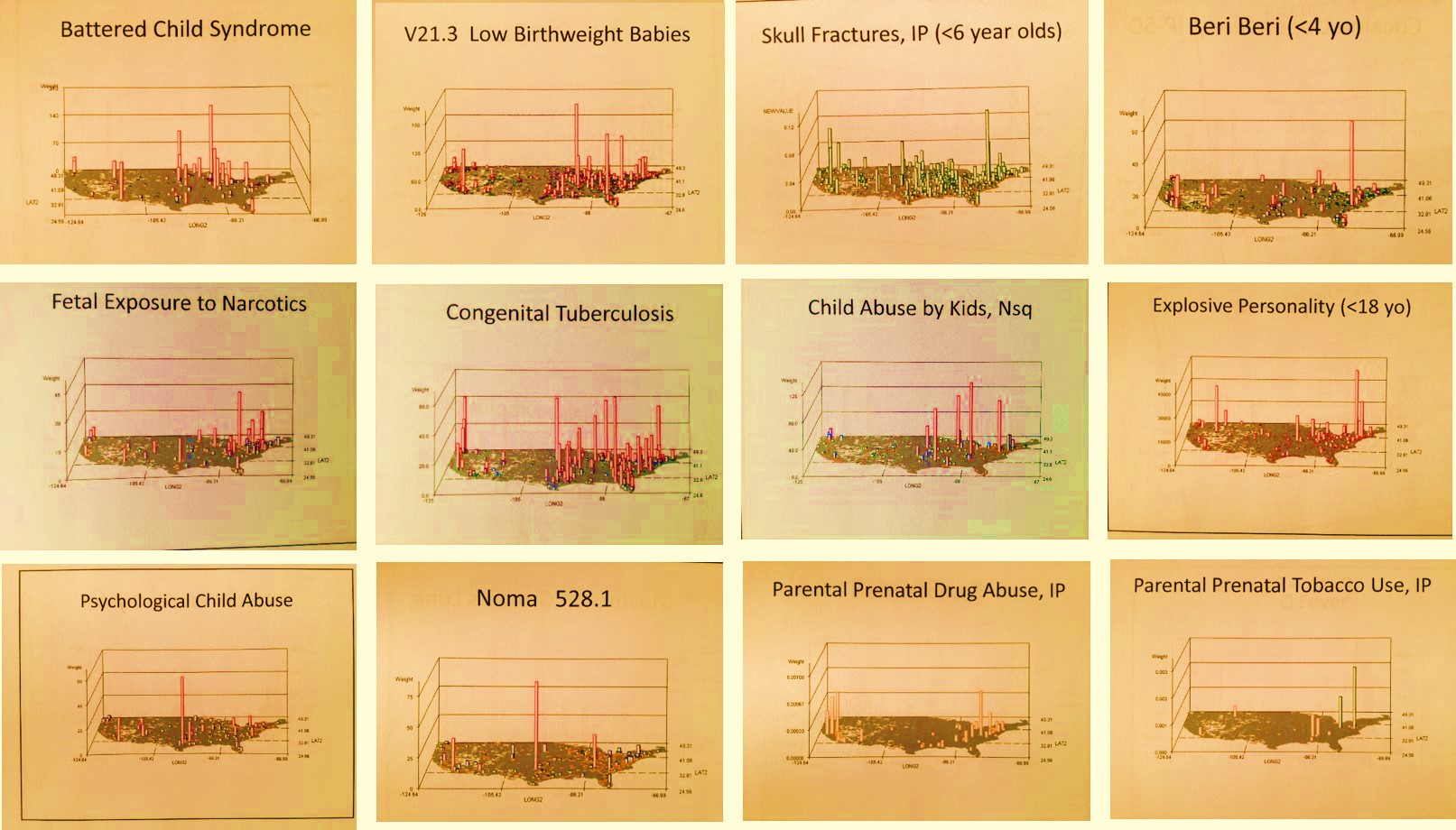
Child Abuse and Neglect
.
In-migration of Diseases
