LINK – – – Skills Test – – – LINK
https://www.surveymonkey.com/s/V5THRFQ
As a student of Northcentral University, I am developing a study on the applications of spatial analysis and GIS to managed care (health insurance and pharmacy benefits manager) programs. By promoting more active surveillance across the managed care venue, we are provided with more opportunities to monitor and make note of important disease behavior and ecological changes.
The following images were applied to a survey I developed on Survey Monkey.
This survey was developed to assess the value of GIS to Managed Care and health insurance programs classified as Health Maintenance Organizations (HMOs) and Preferred Provider Organizations (PPOs).
.
These images will be link to some of the questions in Part 3 of this 30 question survey analytics tool.
The image follows the section title with Image number. The corresponding survey question is provided after that identifier.
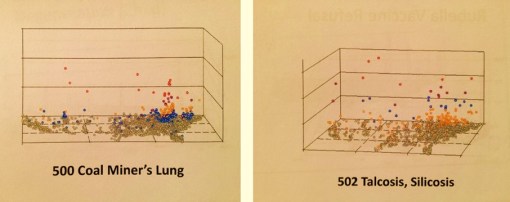
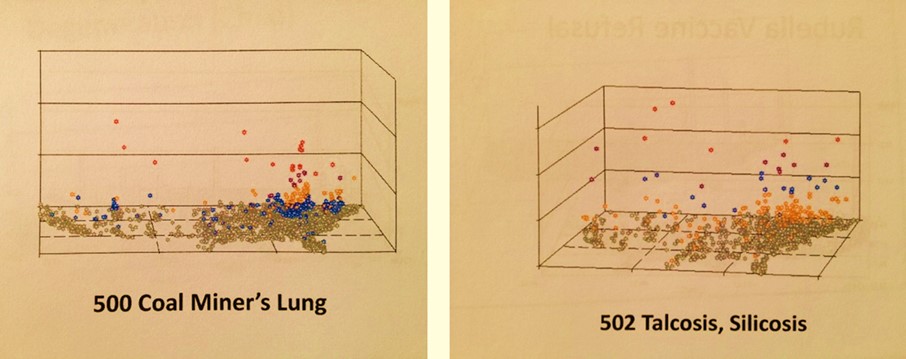
Image 1

The above four images were posted on the web (website noted at base of each map). The current system utilizes these for publishing results. Rank these four in INCREASING order of increase in resolution, and increase in personal or patient identifier potentials.
Image 2

Image 3

Image 4
Image 5
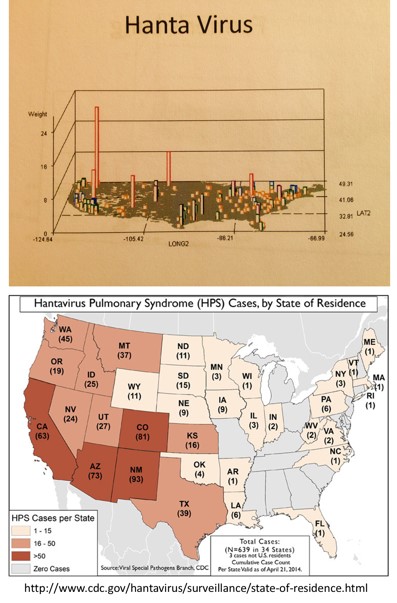
Image 6
Image 7

Image 8

Image 9
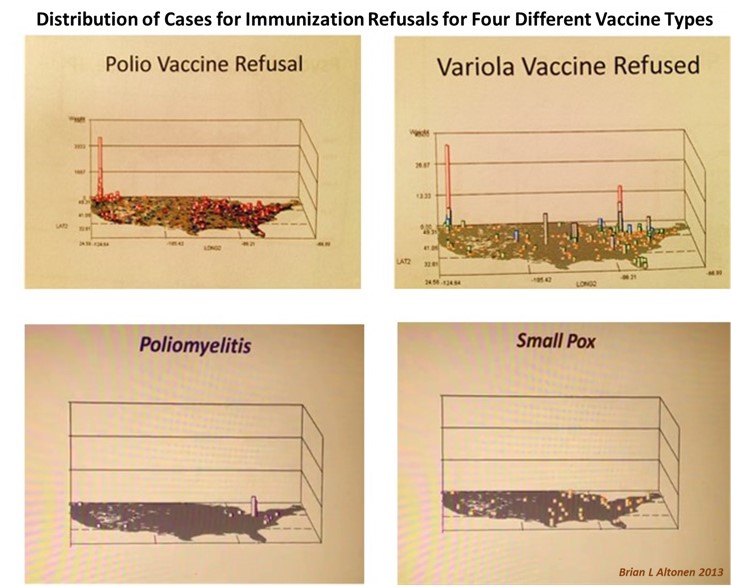
Image 10
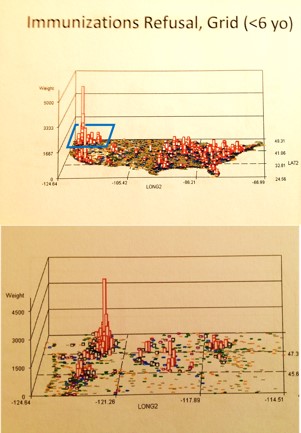
Image 11 (Extra)
***************************************************
Work in Progress
GOAL: DEFINE A POLICY AND PROGRAM FOR MANAGED CARE HIT/GIS PUBLIC HEALTH SURVEILLANCE
Policy implementation steps (tentative, as of 10/25/15):
- Design an institutional GIS-HIT Policy
- Define metrics levels
- Define stages and order of development (see metrics list below, choose several projects to initiate with)
- Define stages and levels of reporting (direct/indirect; next level=clinical/clinical admin; next=upper level admin, public reporting (if any))
- Define the process of developing an HIT-GIS station; define tool or tools, correlate with projects/spatial analytic steps taken
- Set Goals for each stage in this process, define dates for those goals.
- Assign an overall goal of implementing fully functional workstation for certain parts of the HIT-GIS program, testing its performance. [Recommendation: 9 months for Level 1 reporting, 12 months for approval of statement that goal was met. 15 months=produce first report(s) or models for reports.
- Have a Management Report plan and format in place, in order to administer these reports
- Define the exact Metrics [34 types, about 1000-2000 metrics, depending upon reports/subgroupings)
- Initiate use either in sections, or as need requires.
- Produce chronology or GANTT on this
- Evaluate rate of development of the HIT-GIS work stations over time.
- Evaluate rate of documentation of critical events or improvements in HIT-GIS development
*********************************
Description of uses for HIT/GIS
The following is an initial list of the kinds of metrics to consider:
- QA – missing data [unk, total ICD? Region, facility?]
- Standard metrics – population data on ICDs, plus demographics/area [2-16]
- Standard metrics – IH LOS, OP, LOS [7-10],
- Standard ICD QOC metrics – Ch Well Visits; CDM Yrly visits; 2MoFU for MH [10-15]
- Standard Rx Compliance Measures – Refill rates [2-3]
- Ethnicity measure for overall [2-16]
- Basic Foreign Language requirement, documentation metric; external use metric? [8,14]
- Specific Ethnic ICD/place measures (2 levels) – AfrAm or Hisp, other, Asian, AI/NA [5 each, incl W]
- ACOs [45-60]
- Other than ACO/QOC-S, simple basic QIA/PIP metrics (defined elsewhere) [15-20]
- HEDIS Admin metrics focused on facilities [25]
- Institutional 300+ Disease reporting tool (set for monthly or bimonthly use) [repeats above, 1 report, 300+ metrics]
- Ethnic-focused ICD reporting tool/report [40-100, x 4-5, x 8 or 11]
- SES-focused reporting tool, with special topics: poverty groups and areas [ditto]
- Age-subgroups tools: suicide, epilepsy SUNDS etc. [5-7]
- V-codes: ch/adult abuse, abandonment, refusal of care for religious reason, immunization refusal [socially meaningful, 12-15]
- ICD codes: suicide risk, special cultural/region risks, ID risks [age/gender related, 7 x 12 = 94]
- 65+ yo ICDs report [dupl. above but with different ages, ca. 20-100]
- Congenital Diseases report [20-45]
- Genetic Diseases report [1-4, or up to 100+ ICDs]
- Pregnancy/Child-bearing report (Chlamydia and non-chlamydia, age) [30]
- Comprehensive Chronic Disease Mgmt report (2-4 levels) [n cd, 4 grps, 8 regions, 11 facilities, 4-5 ethn]
- Charlson Disease list and scores report (totals, levels 1, 4, 6+) [ditto]
- Prediction modeling formula/reports (regionally, institutionally, by boroughs; SES-PH, BCBS and OptumHealth “black box” tools) [2 formulas, x 8, 11]]
- Newborn/Infant Care (3 or 4 years), risk levels (prediction tool) [25-40 icds, x 8,11]
- Young:Old Childcare (0-8, 9-17) (tic, beh h, ep, pulm, drug, smoking, alc ab, drug ab, suicide, fx, disl, tc.) (prediction tool) 25-40 icds, x 2 age groups, compared x 8, 11]
- Child Schooling (4-17), (Beh H, Nutr, CD, BMI, Injuries, Fx/Disl, ED use) [1 group, ditto]
- Mother:Child relationship (families, unmarr. vs married?; 10-45 yo) [1 group, ditto]
- Childhd:Adult [changing coverage] QOC conversion rates (asthma, CD, MH), 10-30, 12-26, 15-25/27) [25-40 icds, 8, 11]
- Pre-post 65+/- [changing coverage] QOC relationship (55-64, 65-74) [15-40 icds, 2 groups]
- SNGs reports: IDs, Autism, EP, MS, PTSD, Specific Drug Abuse hxs, Bullying, Ch Viol. Ch Sx Ab, Age-Fxs, BioT [15-25 icd small groups, 8, 11]
- Special reports, Risk Areas: Child Abuse indicators combination ICDs and V-codes, Suicide, Adult Abuse, Gender specifics; Infib, Violence indicators 6-12 icd subgroups]
- Special reports, cultural: culturally-bound indicators, culturally-linked indicators, cultural QOC comparisons (B vs W, H vs W, A vs W) [3 x 40 = 120, starting]
- Standardized Special reports: Diabetes, asthma, MS, epilepsy [3-7]
- Design modules, major beneficiaries
- Define and contact internal Gatekeepers for other options
- Document reporting requirements
- Fit requirements into HIT-GIS plan
- PHI
- HIPAA
- Establish IRB engagement process
Note: a fully developed HIT-GIS will be capable of reporting on nearly all of these, and then some.
****************************************************
SURVEILLANCE LISTS
LIST 1 – MANAGED CARE POPULATION HEALTH METRICS (many of these should be reported quarterly, semiannually or annually)
Metrics
[34 types or groupings of metrics, about 1000-2000 metrics, depending upon reports/subgroupings]
The following classes of metrics are defined. All have been developed and produced in the current managed care system and regional health care system that I am responsible for. An estimate of the numbers of metrics that are required appears in brackets.
- QA – missing data [unk, total ICD? Region, facility?]
- Standard metrics – population data on ICDs, plus demographics/area [2-16]
- Standard metrics – IH LOS, OP, LOS [7-10],
- Standard ICD QOC metrics – Ch Well Visits; CDM Yrly visits; 2MoFU for MH [10-15]
- Standard Rx Compliance Measures – Refill rates [2-3]
- Ethnicity measure for overall [2-16]
- Basic Foreign Language requirement, documentation metric; external use metric? [8,14]
- Specific Ethnic ICD/place measures (2 levels) – AfrAm or Hisp, other, Asian, AI/NA [5 each, incl W]
- ACOs, MU metrics [45-60]
- Other than ACO/QOC-S/MUs, simple basic QIA/PIP metrics (defined elsewhere) [15-20]
- HEDIS Admin metrics focused on facilities [25]
- Institutional 300+ Disease reporting tool (set for monthly or bimonthly use) [repeats above, 1 report, 300+ metrics]
- Ethnic-focused ICD reporting tool/report [40-100, x 4-5, x 8 or 11]
- SES-focused reporting tool, with special topics: poverty groups and areas [ditto]
- Age-subgroups tools: suicide, epilepsy SUNDS etc. [5-7]
- V-codes: ch/adult abuse, abandonment, refusal of care for religious reason, immunization refusal [socially meaningful, 12-15]
- ICD codes: suicide risk, special cultural/region risks, ID risks [age/gender related, 7 x 12 = 94]
- E Codes:
- 65+ yo ICDs report [dupl. above but with different ages, ca. 20-100]
- Congenital Diseases report [20-45]
- Genetic Diseases report [1-4, or up to 100+ ICDs]
- Pregnancy/Child-bearing report (Chlamydia and non-chlamydia, age) [30]
- Comprehensive Chronic Disease Mgmt report (2-4 levels) [n cd, 4 grps, 8 regions, 11 facilities, 4-5 ethn]
- Charlson Disease list and scores report (totals, levels 1, 4, 6+) [ditto]
- Prediction modeling formula/reports (regionally, institutionally, by boroughs; SES-PH, BCBS and OptumHealth “black box” tools) [2 formulas, x 8, 11]
- Newborn/Infant Care (3 or 4 years), risk levels (prediction tool) [25-40 icds, x 8,11]
- Young:Old Childcare (0-8, 9-17) (tic, beh h, ep, pulm, drug, smoking, alc ab, drug ab, suicide, fx, disl, tc.) (prediction tool) 25-40 icds, x 2 age groups, compared x 8, 11]
- Child Schooling (4-17), (Beh H, Nutr, CD, BMI, Injuries, Fx/Disl, ED use) [1 group, ditto]
- Mother:Child relationship (families, unmarr. vs married?; 10-45 yo) [1 group, ditto]
- Childhd:Adult [changing coverage] QOC conversion rates (asthma, CD, MH), 10-30, 12-26, 15-25/27) [25-40 icds, 8, 11]
- Pre-post 65+/- [changing coverage] QOC relationship (55-64, 65-74) [15-40 icds, 2 groups]
- SNGs reports: IDs, Autism, EP, MS, PTSD, Specific Drug Abuse hxs, Bullying, Ch Viol. Ch Sx Ab, Age-Fxs, Bioterrorism [15-25 icd small groups, 8, 11]
- Special reports, Risk Areas: Child Abuse indicators combination ICDs and V-codes, Suicide, Adult Abuse, Gender specifics; Infib, Violence indicators 6-12 icd subgroups]
- Special reports, cultural: culturally-bound indicators, culturally-linked indicators, cultural QOC comparisons (B vs W, H vs W, A vs W) [3 x 40 = 120, starting]
- Standardized Special reports: Diabetes, asthma, MS, epilepsy [3-7]
*******************************************
LIST 2 – ZOONOTICS
(use this mostly for part of the public health surveillance program)
The following are defined as metrics for developing an international or cultural disease surveillance work station. (This data was exported, programed and re-merged from the shapefile dbf, so punctuation isn’t perfect.)
- 1 – Coccidiomycosis. ICD=114, Group: Regional Infectiousness. Country or region/nationality: North and South America, South America, Mexico, SW US
- 2 – European Cryptococcus. ICD=117.5, Group: Regional Infectiousness. Country or region/nationality:
- 3 – Elephantiasis. ICD=457.1, Group: Regional Infectiousness. Country or region/nationality: African, Africa
- 4 – Elephantiasis. ICD=125.9, Group: Regional Infectiousness. Country or region/nationality: African, Africa
- 5 – Histoplasmosis. ICD=115, Group: Regional Infectiousness. Country or region/nationality: ,
- 6 – Buruli Ulcer (Mycobacterium ulcerans). ICD=31.1, Group: Regional Infectiousness. Country or region/nationality: African, Africa
- 7 – Strongyloidiasis (Strongyloides stercoralis). ICD=127.2, Group: Regional Infectiousness. Country or region/nationality: African, Tropical and Subtropical
- 8 – Neurocysticercosis (Taenia solium). ICD=123.1, Group: Regional Infectiousness. Country or region/nationality: African, Africa
- 9 – Dracunculiasis (Dracunculus medinensis). ICD=125.7, Group: Regional Infectiousness. Country or region/nationality: African, Africa
- 10 – African Trypanosomiasis. ICD=86.5, Group: Regional Infectiousness. Country or region/nationality: African,
- 11 – Trepanomatosis (Trepanoma spp.). ICD=, Group: Regional Infectiousness. Country or region/nationality: , see Syphilis, Yaws, Pinta, Bejel
- 12 – Leptospirosis (Leptospira). ICD=100, Group: Regional Infectiousness. Country or region/nationality: ,
- 13 – Scabies (Sarcoptis scabiei). ICD=133, Group: Regional Infectiousness. Country or region/nationality: ,
- 14 – CHOLERA. ICD=1, Group: Infectious/Parasitic. Country or region/nationality: India, Ceylon, Peru, Louisiana,
- 15 – TYPHOID. ICD=2, Group: Infectious/Parasitic. Country or region/nationality: ,
- 16 – PARATYPHOID. ICD=2.1, Group: Infectious/Parasitic. Country or region/nationality: ,
- 17 – PARATYPHOID. ICD=2.2, Group: Infectious/Parasitic. Country or region/nationality: ,
- 18 – PARATYPHOID. ICD=2.3, Group: Infectious/Parasitic. Country or region/nationality: ,
- 19 – SHIGELLOSIS. ICD=4, Group: Infectious/Parasitic. Country or region/nationality: ,
- 20 – AMOEBIASIS. ICD=6, Group: Infectious/Parasitic. Country or region/nationality: ,
- 21 – TUBERCULOSIS. ICD=010-018, Group: Infectious/Parasitic. Country or region/nationality: ,
- 22 – LISTERIOSIS. ICD=27, Group: Infectious/Parasitic. Country or region/nationality: ,
- 23 – ERYSIPELOTHRIX (E. Indiosa infection). ICD=27.1, Group: Infectious/Parasitic. Country or region/nationality: ,
- 24 – PASTEURELLOSIS. ICD=27.2, Group: Infectious/Parasitic. Country or region/nationality: ,
- 25 – LEPROSY. ICD=30, Group: Infectious/Parasitic. Country or region/nationality: ,
- 26 – Meningococcal, meningitis. ICD=36, Group: Infectious/Parasitic. Country or region/nationality: ,
- 27 – Meningococcal, encephalitis. ICD=36.1, Group: Infectious/Parasitic. Country or region/nationality: ,
- 28 – Meningococcal, meningococcemia. ICD=36.2, Group: Infectious/Parasitic. Country or region/nationality: ,
- 29 – Meningococcal, Waterhouse-Frederichsen Syndrome. ICD=36.3, Group: Infectious/Parasitic. Country or region/nationality: ,
- 30 – Meningococcal, carditis. ICD=36.4, Group: Infectious/Parasitic. Country or region/nationality: ,
- 31 – SMALL POX. ICD=50, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 32 – COW POX & PARAVACCINIA. ICD=51, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 33 – MILKER’S NODE, PSEUDO-COWPOX. ICD=51.1, Group: Viral Diseases with Exanthema. Country or region/nationality:
- 34 – COW POX. ICD=51.01, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 35 – contagious pustular dermatitis. ICD=51.2, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 36 – CHICKEN POX. ICD=52, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 37 – MEASLES. ICD=55, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 38 – RUBELLA. ICD=56, Group: Viral Diseases with Exanthema. Country or region/nationality: ,
- 39 – VIRAL HEPATITIS. ICD=70, Group: OTHER VIRAL. Country or region/nationality: ,
- 40 – MUMPS. ICD=72, Group: OTHER VIRAL. Country or region/nationality: ,
- 41 – ORNITHOSIS/PSITTACOSIS. ICD=73, Group: OTHER VIRAL. Country or region/nationality: , Europe
- 42 – COXSACKIE. ICD=74, Group: OTHER VIRAL. Country or region/nationality: ,
- 43 – Coxsackie carditis. ICD=74.2, Group: OTHER VIRAL. Country or region/nationality: ,
- 44 – Hand, foot and mouth disease. ICD=74.3, Group: OTHER VIRAL. Country or region/nationality: ,
- 45 – TRACHOMA (Chlamydia sp.). ICD=76, Group: OTHER VIRAL. Country or region/nationality: ,
- 46 – EPIDEMIC KERATOCONJUNCTIVITIS. ICD=77, Group: OTHER VIRAL. Country or region/nationality: ,
- 47 – Swimming Pool Conjunctivitis. ICD=77, Group: OTHER VIRAL. Country or region/nationality: ,
- 48 – Shipyard Eye. ICD=77.1, Group: OTHER VIRAL. Country or region/nationality: ,
- 49 – SWEATING FEVER. ICD=78.2, Group: OTHER VIRAL. Country or region/nationality: ,
- 50 – CAT-SCRATCH DISEASE. ICD=78.3, Group: OTHER VIRAL. Country or region/nationality: ,
- 51 – FOOT AND MOUTH DISEASE. ICD=78.4, Group: OTHER VIRAL. Country or region/nationality: ,
- 52 – CYTOMEGALOVIRUS. ICD=78.5, Group: OTHER VIRAL. Country or region/nationality: ,
- 53 – KOREAN/RUSSIAN HEMORRHAGIC NEPHROSONEPHRITIS. ICD=78.6, Group: OTHER VIRAL. Country or region/nationality: ,
- 54 – YELLOW FEVER. ICD=60, Group: Arthropod-born. Country or region/nationality: , Orig. Africa, then Americas *
- 55 – DENGUE. ICD=61, Group: Arthropod-born. Country or region/nationality: , Asia, Africa, North America
- 56 – Japanese Encephalitis. ICD=62, Group: Mosquito-born Encephalitides. Country or region/nationality: Japan, Japan
- 57 – California Encephalitis. ICD=62.5, Group: Arthropod-born. Country or region/nationality: , U.S.
- 58 – St. Louis Equine Encephalitis. ICD=62.3, Group: Arthropod-born. Country or region/nationality: , U.S.
- 59 – Eastern EE. ICD=62.2, Group: Arthropod-born. Country or region/nationality: , U.S.
- 60 – Western EE. ICD=62.1, Group: Arthropod-born. Country or region/nationality: , U.S.
- 61 – Venezuelan Encephalitis. ICD=66.2, Group: Arthropod-born. Country or region/nationality: , South America, Venezuela
- 62 – Australian Encephalitis. ICD=62.4, Group: Arthropod-born. Country or region/nationality: Australian, Australia
- 63 – Taiga Spring-Summer Encephalitis (RSSE). ICD=63, Group: Arthropod-born. Country or region/nationality: Russian,
- 64 – Central European Encephalitis. ICD=63.2, Group: Arthropod-born. Country or region/nationality: Russian, Eastern Europe
- 65 – Louping Illness. ICD=63.1, Group: Arthropod-born. Country or region/nationality: Russian, Western European (Scottish history)
- 66 – Colorado Tick Fever. ICD=, Group: Arthropod-born. Country or region/nationality: , Colorado, NW U.S.
- 67 – Tick-borne Relapsing Fever, Old World. ICD=87, Group: Arthropod-born. Country or region/nationality: ,
- 68 – Tick-borne Relapsing Fever, New World. ICD=87, Group: Arthropod-born. Country or region/nationality: , South and North America
- 69 – Lyme Disease . ICD=, Group: Arthropod-born. Country or region/nationality: , Sweden, U.S.
- 70 – Tick-borne Typhus (Rocky Mountain Spotted Fever). ICD=, Group: Arthropod-born. Country or region/nationality: , North America
- 71 – Tick-borne Typhus (Old World). ICD=, Group: Arthropod-born. Country or region/nationality: ,
- 72 – Endemic Typhus. ICD=, Group: Arthropod-born. Country or region/nationality: ,
- 73 – Viral Encephalitis. ICD=64, Group: Arthropod-born. Country or region/nationality: ,
- 74 – Omsk Hemorrhagic. ICD=65.1, Group: . Country or region/nationality: Russian, western Siberia, in places including Omsk, Novosibirsk, Kurgan, and Tyumen
- 75 – West Nile. ICD=66.4, Group: Arthropod-born. Country or region/nationality: African, Egypt
- 76 – MURINE TYPHUS. ICD=81, Group: RICKETTSIOSES, TYPHUS. Country or region/nationality: ,
- 77 – BRILL’S DISEASE. ICD=81.1, Group: RICKETTSIOSES, TYPHUS. Country or region/nationality: , NYC
- 78 – SCRUB TYPHUS. ICD=81.2, Group: RICKETTSIOSES, TYPHUS. Country or region/nationality: , Japan, Kedani Fever, mite-born typhus, tustsugamushi
- 79 – SPOTTED FEVERS. ICD=82, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: ,
- 80 – BOUTONNEUSE FEVER. ICD=82.1, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: India, African, Indian, Kenyan, Marseilles, Mediterranean Tick Fever
- 81 – NORTH ASIAN TICK FEVER. ICD=82.2, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: Russian, Russia
- 82 – QUEENSLAND TICK TYPHUS. ICD=82.3, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: Australian, Australia
- 83 – LONE STAR FEVER. ICD=82.8, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: ,
- 84 – EHRLICHIOSIS. ICD=82.4, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: ,
- 85 – Q-FEVER (Coxiella burnetii). ICD=83, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: Australian, Australia origins
- 86 – TRENCH FEVER. ICD=83.1, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: , Europe to Egypt, Urban
- 87 – RICKETTSIALPOX. ICD=83.2, Group: RICKETTSIOSES, TICK-BORN. Country or region/nationality: Russian, Russia, Japan
- 88 – MALARIA. ICD=84, Group: MOSQUITO-BORN. Country or region/nationality: ,
- 89 – BLACKWATER FEVER. ICD=84.8, Group: MOSQUITO-BORN. Country or region/nationality: ,
- 90 – QUARTAN. ICD=84.2, Group: MOSQUITO-BORN. Country or region/nationality: ,
- 91 – MALIGNANT. ICD=84, Group: MOSQUITO-BORN. Country or region/nationality: ,
- 92 – Louse-borne Rickettsia Typhus (Rickettsia prowazekii, transmitted by the human body louse (Pediculus humanus corporis). Associated with Brill-Zinnser Disease. ICD=80, Group: LOUSE BORN. Country or region/nationality: ,
- 93 – Scrub Typhus . ICD=81.2, Group: . Country or region/nationality: Australian, Russia, Australia, Pakistan, Afghanistan (tsutsugamushi triangle)
- 94 – Trypanosomiasis (African Sleeping Sickness). ICD=86, Group: FLY BORN. Country or region/nationality: African, Africa
- 95 – RELAPSING FEVER. ICD=87, Group: FLY BORN. Country or region/nationality: ,
- 96 – Louse-born. ICD=87, Group: LOUSE BORN. Country or region/nationality: , South and North America
- 97 – Tick born. ICD=87.1, Group: TICK BORN. Country or region/nationality: , South and North America
- 98 – LEISHMANIASIS. ICD=85, Group: LEISHMANIASIS. Country or region/nationality: ,
- 99 – VISCERAL (post kala-azar, Mediterranean). ICD=85, Group: LEISHMANIASIS. Country or region/nationality: ,
- 100 – Asian Leishmaniasis. ICD=85.2, Group: LEISHMANIASIS. Country or region/nationality: Asian, Asia
- 101 – Ethiopian Leishmaniasis. ICD=85.3, Group: LEISHMANIASIS. Country or region/nationality: African, Africa
- 102 – Leishmaniasis. ICD=85.5, Group: LEISHMANIASIS. Country or region/nationality: ,
- 103 – CUTANEOUS LEISHMANIASIS. ICD=85, Group: LEISHMANIASIS. Country or region/nationality: India, Aleppo, Baghdad, Delhi
- 104 – PLAGUE (Yersinia pestis). ICD=, Group: . Country or region/nationality: , worldwide
- 105 – Murine Flea-borne Rickettsia or Typhus. ICD=80, Group: . Country or region/nationality: , America, Pacific Rim, worldwide urban settings
- 106 – . ICD=81, Group: . Country or region/nationality: ,
- 107 – . ICD=82, Group: . Country or region/nationality: ,
- 108 – . ICD=83, Group: . Country or region/nationality: ,
- 109 – Loasis. ICD=125.2, Group: . Country or region/nationality: , Africa
- 110 – Pinta. ICD=103, Group: Non-arthropod-borne. Country or region/nationality: , Mexico, Central America *
- 111 – Kyanasur Forest Disease. ICD=65.2, Group: . Country or region/nationality: Asian, Indian, African, S/SE Asia, India
- 112 – Anthrax . ICD=, Group: Non-arthropod-borne. Country or region/nationality: ,
- 113 – Bejel. ICD=104, Group: Non-arthropod-borne. Country or region/nationality: Middle East, Middle East, esp. Bedouin Tribes
- 114 – Yaws. ICD=102, Group: Non-arthropod-borne. Country or region/nationality: , originated in tropical Africa
- 115 – Chagas. ICD=103, Group: Non-arthropod-borne. Country or region/nationality: , South America *
- 116 – Cestodes Tapeworm. ICD=122, Group: Non-arthropod-borne. Country or region/nationality: ,
- 117 – Cestodes Tapeworm. ICD=123, Group: Non-arthropod-borne. Country or region/nationality: ,
- 118 – Chicago Disease (Blastomyces dermatitidis-fungus)[U.S.. ICD=, Group: Non-arthropod-borne. Country or region/nationality: ,
- 119 – Chiclero Ulcer. ICD=, Group: Non-arthropod-borne. Country or region/nationality: South American/Central American/Mexico, Mexico, some of Central America *
- 120 – Creutzfeld Jakob Disease (Mad Cow). ICD=46.11, Group: . Country or region/nationality: ,
- 121 – Eyeworm Disease of Africa. ICD=, Group: Non-arthropod-borne. Country or region/nationality: African, Africa
- 122 – Filaria . ICD=, Group: Non-arthropod-borne. Country or region/nationality: ,
- 123 – Guinea Worm. ICD=, Group: Non-arthropod-borne. Country or region/nationality: African, Northern Africa, formerly Asia
- 124 – Giardia. ICD=7.1, Group: Non-arthropod-borne. Country or region/nationality: ,
- 125 – Ancyclostomiasis. ICD=126.9, Group: Non-arthropod-borne. Country or region/nationality: ,
- 126 – Histoplasmosis. ICD=115, Group: Non-arthropod-borne. Country or region/nationality: , North American caves, fungus
- 127 – Hookworm (Necator spp.). ICD=126.9, Group: Non-arthropod-borne. Country or region/nationality: , New World
- 128 – Hookworm (Ancyclostoma sp.). ICD=126.9, Group: Non-arthropod-borne. Country or region/nationality: , Old World
- 129 – Gnathostomiasis (Gnathostoma spp.). ICD=128.1, Group: Non-arthropod-borne. Country or region/nationality: , England
- 130 – Korean Hemorrhagic Fever. ICD=78.6, Group: Non-arthropod-borne. Country or region/nationality: Asian, Korea
- 131 – Machupo Virus (Bolivian) Hemorrhagic Fever. ICD=78.7, Group: Viral Fevers. Country or region/nationality: South American/Central American/Mexico, Bolivia, western South America
- 132 – Hanta Virus and allies. ICD=79.81, Group: Viral Fevers. Country or region/nationality: Asian, Korea, US
- 133 – Ebola. ICD=65.8, Group: Viral Fevers. Country or region/nationality: African, Zaire, Sudan, Ivory Coast, Bundibugyo (Reston, Va)
- 134 – Monkey Pox/Yaba Pox. ICD=59.22, Group: Viral Fevers. Country or region/nationality: African, Africa
- 135 – Yatapox /Tanapox. ICD=59.21, Group: Viral Fevers. Country or region/nationality: African, Africa, Kenya/Zaire
- 136 – Kala Azar. ICD=85, Group: Viral Fevers. Country or region/nationality: , Tropical
- 137 – Noma. ICD=528.1, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: ,
- 138 – Kwashiorker. ICD=260, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: ,
- 139 – Kuru. ICD=46, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: African, Papua New Guinea
- 140 – Takot Subo. ICD=429.3, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: Japan, Japan
- 141 – Takayasu’s Arteritis. ICD=446.7, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: Japan, Japan
- 142 – Moya Moya. ICD=437.5, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: Japan, Japan, Hawaii
- 143 – American Leishmaniasis. ICD=85.4, Group: LEISHMANIASIS. Country or region/nationality: South American/Central American/Mexico, North(?) and South America
- 144 – Brazilian Blastomycosis. ICD=116.1, Group: Non-arthropod-borne. Country or region/nationality: South American/Central American/Mexico, Brazil *
- 145 – Pinta. ICD=103, Group: DISEASES WITH SPECIFIC CULTURAL GROUPS/ORIGINS. Country or region/nationality: South American/Central American/Mexico, Mexico, Central America *
- 146 – ARENOVIRAL HEMORRHAGIC FEVER. ICD=78.7, Group: DISEASES WITH SPECIFIC CULTURAL GROUPS/ORIGINS. Country or region/nationality: South American/Central American/Mexico, Argentine, Bolivian, Junin, Machupo)
- 147 – American Trypanosomiasis /Chagas. ICD=86, Group: . Country or region/nationality: South American/Central American/Mexico, North and South America *
- 148 – Crimean Hemorrhagic Congo Virus. ICD=63, Group: . Country or region/nationality: Russian, Africa, Russia
- 149 – Taiga Spring-Summer Encephalitis (RSSE). ICD=63, Group: . Country or region/nationality: Russian, Russia
- 150 – Chigger-born Rickettsia (Rickettsia tsutsugamushi, in chiggers of Leptotrombidium (Trombicula) akamushi and Leptotrombidium deliense. In Japan, some cases transmitted by mites of Leptotrombidium scutellare and Leptotrombidium pallidum). ICD=, Group: . Country or region/nationality: Russian, Russia, Japan
- 151 – SCRUB TYPHUS. ICD=81.2, Group: . Country or region/nationality: Japan, Japan, Kedani Fever, mite-born typhus, tustsugamushi
- 152 – African Idiopathic Cardiomegaly. ICD=425.4, Group: Non-infectious Diseases, Other Cultures. Country or region/nationality: African, Africa
- 153 – Monkey Pox/Yaba Pox. ICD=59.22, Group: . Country or region/nationality: African, Africa
- 154 – Crimean Hemorrhagic Congo Virus. ICD=65, Group: . Country or region/nationality: African, Africa, Russia
- 155 – Onchocerciasis. ICD=125.3, Group: . Country or region/nationality: African, Africa
———————————————
RESEARCH NOTES – 12/5/2015.
NOTE: These are ongoing, regular projects I am currently engaged in for studies of a 10M patients population of multiple, ethnic backgrounds, and 20+ years of data. (Students: feel free to cut and paste, just please cite me (this date 12/9/15)–I kept some of the codes/text out for ICD10.)
*******************************************
RESEARCH PROJECTS DEVELOPED & BEING TESTED
MAJOR THEME – PUBLIC HEALTH, CULTURE & SES
RESEARCH TOPIC 1.
Cultural-Familial Linked Healthcare Practices and Diagnoses
Research Question: How are the familial, genetic and developmental diseases distributed in terms of zip code tract and specific cultural regions defined for [the] City?
A number of ICDs and ICD groups have been identified as value surveillance tools used to assess the distribution of healthcare needs in [the] City.
The study of genetically based disease patterns has several levels of complexity and resource utilization. Traditional studies have focused on familiar genetic disease patterns, with the focus on chronic diseases such as diabetes, obesity, hyperlipidemia, birth defects, congenital abnormalities, and most recently, epilepsy, endocrine diseases, and susceptibility to certain forms of cancer such as breast and cervical cancer. This study divides diagnoses pertaining to possible genetically-based disease patterns into several groups: i) well-documented congenital disease patterns, often detected using standard chromosomal screening processes, ii) congenital diseases and unanticipated birth relate diagnoses, some without a prior history (i.e. cystic fibrosis, tissue degenerative diseases, retinitis pigmentosa), iii) familial chronic disease patterns (the common familial heart disease patterns, along with HTN, HL, DM, and Obesity), iv) a number of very recent, genetic-screening findings, and v) specific behavioral health or cognitive function diagnoses with possible relationship to family history (ADD, epilepsy). This study focuses on ICD related diagnoses that are related to the second category–congenital diseases and unanticipated birth relate diagnoses, some without a prior history. Genetic screening practices are already in place for diagnoses defined by the first and fourth categories. The third category (familial chronic diseases) has adequate services underway, many of which are well into their testing phase. The fifth category, behavioral health, remains the least explored of these topics clinically and experimentally for the moment, and is not reviewed for this study.
To carry out this analysis, the following ICDs need to be thoroughly reviewed and very specialized lists developed for the population health analysis.
RESEARCH TOPIC 2
Congenital, Developmental Risk Assessment (The ICD 740.* Series Study)
The 740 to 759.99 series are all related to developmental disorders, usually part of the care program well after labor and delivery. (BETWEEN 740 and 759.99)
The following ranges define the subgroups for this review, from this series. These groups will be reviewed separately as well as merged into one dataset. The standard state, county, borough, district, census block, block group, network, facility and zipcode methods of spatial analyses will be used.
- 740-742.99-Nervous system (6 values),
- 743-744.99-Eyes, ears, face, neck (27),
- 745-747.99-Circulatory system (40),
- 748-748.99-Respiratory (2),
- 749-751.99-Digestive (23),
- 752-752.99-Genital Organs (14),
- 753-753.99-Urinary (10),
- 754-756.99-Musculoskeletal (35),
- 757-757.99-Integument (8),
- 758-758.99-Chromosomal anomalies (18), and
- 759-759.99-Other severe conditions (15).
Other childhood risk indicators possibly related to this study include:
- Consciousness alteration (780, 780.0-coma, 780.01, 780.02, 780.03, 780.09)
- Convulsions (780.3, 780.31, 780.32, 780.39)
- Severe diaphoresis (780.8)
- Fussy infant (780.91), Crying infant (780.92) and Excessive Crying (780.95)
- Jaundice (782.4)
- Cyanosis (782.5)
- Petechiae (782.7)
- Aphasia (784.3)
- Aphonia (784.4, 784.41)
- Alexia (784.61)
- Apnea and other rhythmic breathing disorders or S/S (786.03 – 786.09)
- Stridor (786.1)
- Hemoptysis (786.3)
- Chest Pain (786.5, 786.51, 786.52)
- Rales (786.7)
- NVD (787.0, 787.01, 787.02, 787.03)
- Abdominal, Pelvic abnormality (789, 789.0, 789.1, 789.2, 789.3, 789.4, 789.5, 789.6)
- Morbidity-Mortality S&S (798, sudden death, SIDS, 798.0,.1.,.2.,.8.,.9)
- Asphyxia (799.0)
- Respiratory Arrest (799.1)
- Debility (799.3)
- Cachexia (799.4)
RESEARCH TOPIC 3.
Childhood Diseases and healthcare needed related to genetic disease and potential disease history features
Research Questions: Are there particular genetic diseases that exist in clusters in the ***** City area? Are there adequate facilities and programs in place to meet their needs?
The goal is to compare these results regionally, culturally, and in terms of identified religious groups.
The following 170 conditions or condition classes from ICD9 are identified for this study.
Endocrine (271.0, 271.1, 271.3, 272.1, 272.2, 272.3, 272.4, 272.5, 272.6, 272.7, 273.8, 275.0, 275.1, 275.2, 275.3, 275.4, 275.41, 275.42, 275.49)
- Pompe’s Glyconeogenesis Disease (271.0)
- Galactosemia (271.1)
- Hereditary fructose intolerance (271.2)
- Congenital Lactose deficiency (271.3)
- Familial hypercholesterolemia (272.1)
- Frederickson hyperlipoproteinemia (272.2)
- Burger-Grutz Sydrome (272.3)
- Alpha-lipoproteinemia (272.4)
- Bassen-Kornzweig Syndrome (272.5)
- Lipodystrophy (272.6)
- Gaucher’s/Niemann-Pick Disease (272.7)
- Familial Trasferremia (273.8)
- Hereditary hemochromatosis (275.0)
- Wilson’s (Cu metab) Disease (275.1)
- Magnesemia (275.2)
- Hypophosphatasia (275.3)
- Calcemia, hyperparathyroidism (275.4, 275.41, 275.42, 275.49)
Metabolic Disorders (277, 277.0, 277.2, 277.3, 277.4, 277.5, 277.6, 277.7, 277.81, 277.85, 277.86, 277.87)
- Cystic fibrosis (277.0)
- Porphyria (277.1)
- Lesch-Nyhan Syndrome (277.2)
- Familial Mediterranean Fever (277.3)
- Crigler-Najjar/Gilbert’s Syndrome, hyperbilirubinemia (277.4)
- Mucopolysaccharidosis, Hurler’s, Hunter’s, Sanfillipo’s syndrome (277.5)
- Alpha-1-Antitrypsin deficiency, hereditary angioedema (277.6)
- Dysmetabolic syndrome (277.7)
- Primary carnitine deficinency (277.81)
- Fatty Acid oxidation metabolism (277.85)
- Zellweger Syndrome, peroxisomal metab. (277.86)
- Kearns-Sayre Syndrome, mitochondrial metab. (277.87)
Obesity (278.0) [focus on morbid, esp. cases with genetic predispositions in the form of lipid metabolism disturbances]
Immune Disorders (279, 279.11, 279.12, 279.13)
- DiGeorge Syndrome (279.11)
- Wiskott-Aldrich Syndrome (279.12)
- Nezelof’s Syndrome (279.13)
Digestive Tract – Oral (520, 520.0, 520.1, 520.2, 520.3, 520.4, 520.5 520.6, 520.7, 524, 524.0, 524.03, 524.1, 524.2, 524.3, 524.4, 524.5, 524.6, 524.7, 524.8, 528.1, 528.0
- Anodontia and other tooth disorders (520, 520.0, 520.1, 520.2, . . . 520.7)
- Dentofacial anomalies (524, 524.0, 524.03, 524.1, 524.2, 524.3 . . . 524.8)
- Cancrum oris, noma (528.1)
- Stomatitis (528.0)
Optic (362.7, 362.74, 362.76, 369.0, 371.5, 371.50, 371.51, 371.52, 371.53, 371.54, 371.55, 371.56, 371.57, 371.58, 377.17, 378, 378.0, 378.3, 378.30, 378.31, 378.32, 378.33, 378.34, 378.35, 378.5, 759.89, 743.45, 743.3, 377.43, 743.57, 743.58, 270.2, 389.*)
- Hereditary retinal dystrophy (362.7)
- Retinitis pigmentosa (362.74)
- Leber’s Congenital Amaurosis (362.76)
- Blindness, bilateral, profound (369.0)
- Hereditary Corneal Dystrophy (371.5, 371.50, 371.51, 371.52 . . . 371.58)
- Leber’s Hereditary optic neuropathy (377.17)
- Congenital Strabismus (378)
- Esotropia (378.0)
- Exotropia (378.1)
- Heterotropias (378.3, 378.30, 378.31, 378.32 . . . 378.35)
- Paralytic strabismus (378.5)
- Noonan Syndrome (759.89)
- Aniridia (743.45)
- Congenital Cataract (743.3)
- Optic Nerve hypoplasia (377.43, 743.57, 743.58)
- Albinism (270.2)
- Deafness (389.*)
Neurological (330.00, 330.1, 331.3, 331.81, 331.8, 332.0, 333.0, 331.1, 333.2, 333.4, 333.8, 333.81, 334.0, 334.8, 334.1, 335, 335.2, 335.20, 335.21, 335.22, 335.23, 335.24, 335.29, 340, 341.1, 342, 342.0, 342.1, 343, 343.0, 343.1, 343.2, 348.1, 348.0, 356.0, 356.2, 356.3, 356.1, 358.0, 358.01, 358.02, 359, 359.0, 359.1)
- Leukodystrophy, Krabbe Disease, Peliaeus-Merzbacher Disease (330.0)
- Batten/Tay Sachs Disease (330.1)
- Communicating hydrocephalus (331.3)
- Reye’s Syndrome (331.81)
- Cerebral degeneration (331.8)
- Primary Parkinsonism (332.0)
- Olivopontocerebellar atrophy/Shy-Drager syndrome (333.0)
- Familial Tremor (331.1)
- Lafora’s/Unverricht Myoclonal Disease (333.2)
- Huntington’s Chorea (333.4)
- Torsion Dystonia (333.8)
- Blepharospasm (333.81)
- Friedreich’s Spinocerebellar Ataxia (334.0)
- Ataxia-telangiectasia (Louis-Bar Syndrome) (334.8)
- Hereditary spastic paraplegia (334.1)
- Anterior Horn Cell Diseases (335)
- Motoneuron disease (335.2, 335.20, 335.21, 335.22, 335.23, 335.24, 335.29)
- MS (340)
- Schilder’s Disease, Diffuse myelinoclastic sclerosis (341.1)
- Hemiplegia (342, 342.0, 342.1)
- Cerebral Palsy (343, 343.0. 343.1, 343.2)
- Epilepsy (345.*)
- Anoxic Brain Damage (348.1)
- Cerebral Cysts (348.0)
- Hereditary Peripheral Neuropathy (356.0)
- Hereditary Sensory Neuropathy (356.2)
- Refsum’s Disease (356.3)
- Peroneal muscular atrophy (356.1)
- Myasthenia Gravis 358.0,. .01, .02)
- Benign Congenital Myopathy (359, 359.0)
- Muscular Dystrophy (359.1)
Genetic Blood Diseases (280.0, 282, 282.0, 282.2, 282.5, 282.6, 282.4, 282.43, 282.45, 282.44, 282.1, 282.8, 282.7, 282.9, 284.0, 284.01, 287.1, 288.2, 289.81, 289.7, 446.6, 759.89, 285.0, 286, 286.0, 286.1, 286.2, 282.3, 282.4, 282.6, 282.9, 773, 757.39)
- Pernicious anemia (280.0)
- Hereditary hemolytic anemias (282)
- Hereditary spherocytosis (282.0)
- G6PD (282.2)
- Sickle Cell trait (282.5)
- Sickle Cell anemia (282.6)
- Thalassemia (282.4)
- Delta-Thalassemia (282.45)
- Alpha-Thalassemia (282.43)
- Beta-Thalassemia (282.44)
- Hereditary elliptocytosis, SE Asian ovalocytosis (282.1)
- Hereditary somatocytosis (282.8)
- Hereditary hemoglobinopathy, Hereditary Persistant Fetal Hgb (282.7)
- Fanconi’s Anemia (284.0)
- Bernard-Soulier Syndrome (287.1)
- Diamond-Blackfan Anemia (284.01)
- May-Hegglin Anomaly (288.2)
- Antithrombin III deficiency (289.81)
- Protein C deficiency (289.81)
- Congenital Methemoglobinemia (289.7)
- Upshaw-Schulman Syndrome (446.6)
- Allport Syndrome (759.89)
- Hermansky-Pudlak Syndrome
- Grey Platelet Syndrome
- Quebec Platelet Disorder
- Sideroblastic Anermia (285.0)
- Hemophilia (286)
- Hemophila A (286.0)
- Hemophilia B (286.1)
- Hemophilia C (286.2)
- Von Willebrand’s Disease (286.4)
- Hypoprothrombinemia/Factor XIII deficiency/Congenital afibrinogenemia (286.3)
- Defibrination Syndrome (DIC) (286.6)
- Coagulation Defects (286.9)
- Newborn hemolytic disease (773)
Dyskeratosis congenita (757.39)
These ICDs will be reviewed as boroughs, network, facility and zip code datasets.
RESEARCH TOPIC 4.
High Risk Prenatal Postpartum Care
Research Question: What are the highest risk regions for prenatal-postnatal care, based upon age-diagnostic/therapeutic features?
Populations of the following age categories are evaluated: Female <8, 8 to 12, 13 to 15, 16 to 17, 18-20, 21 to 24 (perhaps 25-29). Evaluations focus on ICDs related to pregnancy, chlamydia, STDs. V codes and E codes may also be evaluated for certain risk indicators. Parent-abused Child codes may also be added for another dimension of this analysis. HIV immunization rates may be included in this review as well.
Evaluate population health features, at the zip code tract, and if possible census block or block group level. Include race and religious group focus.
This study duplicates portions of two standard MCD studies, focused on prenatal-postpartum care analysis, and chlamydia care for young adults. V-codes and E-codes are added in order to assess parent-child relationship. Detailed population pyramids will provide important data pertaining to how to evaluate the young parent:child ratio each study group has. Certain religious or ethnic groups may demonstrate a greater number of children per primary adult or parental care provider. Certain regions are expected to demonstrated higher ratios as well. Standard census related zipcode-household income data may be incorporated into this study.
RESEARCH TOPIC 5
Childhood Wellness
Research questions: What is the rate of compliance for children undergoing the appropriate number of wellness visits between the ages of 0 and 24 months? 2 years and 5 years? What is the rate of lead screening that these patients undergo? Which well visits are missed the most? What are the primarily preventive health procedures associated with each visit?
A preliminary study of well visits in relation to immunization requriements for children suggested that the reason a child who undergoes a healthcare visit (emergent, urgent, therapeutic, or actual well visit with the appropriate goal(s) in mind) has certain visits that are required in order to complete the immunization process. This study focuses on well visit behaviors, to determine which well visits are most adhered to versus those most likely to be missed. Since each well visit has a particular set of expectations involving the assessment and lab related practices engaged in by the care givers, this study is meant to determine which well visits are most often missed, and those most likely attended, based upon months of age and time since the last visit. The following time frame for 0-2 yo children is reviewed: 0-1 week, 0-1 mo, 1.5-3 mo, practitioner, 6 mo, 9 mo., 12-15 mo, 18 mo, 2 yr., 3 yr, 4 yr, and 5 yr. These evaluations will later be used to identify study population for assessing particular development disorders based upon ICDs, to determine if any relation exists between well visit practices or lack thereof, types of developmental and behavioral disabilities developed, in association with the standard demographic features (place, SES, MCD or not).
Evaluating this data by zip code tract, relate the outcomes to closest facilities and/or PCP care related opportunities.
RESEARCH TOPIC 6
Childhood Congenital and Development Disease Screening-First Diagnosis Age-specific Rates
Research question: How effective and timely are the initial screening-first visit-first test practices for children suspected to have a familiar or genetic disease?
Age specific rates are the rates at which a process is completed in health care by a certain age-related deadline or recommendation. In the case of preschool children for example, learning related disability may need to be assessed by the age of 5, or the first month that child attends a regular school. During the first days, weeks and months of a child’s lifespan, certain signs and symptoms should in theory lead to specific rule out procedures. This study evaluates the earliest age in which the rule out process is fully carried out. These measures are also reviewed in relation to expected healthcare visit rates and patterns. Delayed health care processes are evaluated using temporal and log regression models. ICDs to be evaluated specifically for this study have yet to be determined.
RESEARCH TOPIC 7
Elementary, Middle School and High School Health Risk Rates
Research questions: What are the rates of risky behaviors for school age children? Which of these are the best indicators for regional school children’s health?
A population health risk score can be developed using the following ICD data, and related initial and follow-up health care processes. V codes and E codes included. Examples: Elementary: test results hx, STDs, smoking hx, drug hx/note, abuse hx, poor nutrition/malnutrition dx, chronic disease history already documented, 312-316 level learning disability dx, ASD dx,, wt/obesity Middle School: test results hx, anorexia nervosa, STDs, smoking hx, drug hx/note, abuse hx, sexual abuse hx, counseling hx, violence syndromes, chronic disease history already documented, certain beh/psych dx, ASD dx,, wt/obesity. High School: anorexia nervosa, STDs, smoking hx, drug hx/note, abuse hx, sexual abuse hx, counseling hx, violence syndromes, chronic disease history already documented, certain beh/psych dx, ASD dx, wt/obesity. Algorithm to be developed. Predictive modeling application.
RESEARCH TOPIC 8
Child Abuse Indicators
Research Questions: What are the primary indicators that to be used for evaluating regions and programs for child abuse related problems? V-codes? E-codes?
Nutritional deficiencies (260-269) [BETWEEN 260 and 269.99]
- Kwashiorkor (260)
- Nutritional marasmus (261)
- Severe protein-calorie malnutrition (262)
- Other protein-calorie malnutrition (263)
- Vitamin A deficiency (264, 264.0 – 264.9)
- Thiamine deficiency (265), beriberi (265.0), Wernickes Encephalopathy (265.1), Pellagra (265.2)
- Vitamin B deficiency (266, 266.0, 266.2)
- Vitamin C deficiency (267)
- Vitamin D deficiency (268, 268.0, 268.1, 268.2, 268.9)
- Vitamin K deficiency (269.0)
- Other vitamin/mineral deficiency (269.2, 269.3, 269)
Other ICD groups (need to work on this)
- Injuries
- Fractures
- Dislocations
- Infections
- Behaviors (Parent)
- Abuse
- Abandonment
RESEARCH TOPIC 9
Chronic Obstructive Sleep Apnea
Research question: how common are the Sleep Apnea disturbances within the [city] area?
780.5, 780.50, 780.51. 780.52, 780.53, 780.54, 780.55, 780.56, 780.57, 780.58, 780.59
TBD/Work in Process. Confidential with Principal Investigator.
RESEARCH TOPIC 10
Aging, Human Behavior and Fractures
Research question: what is the relationship between age or age range/group, and particular types of fractures and dislocations?
An evaluation of all fracture and dislocation codes, as individual body part codes or groups of codes. Open and closed fractures may be compared at the appendages level (Null hypothesis assumed for this group.) Several fractures may be considered specific to particular public and behavioral health findings, linked to child abuse and elder abuse. These distinct fracture/dislocation groups will be evaluated and compared. Nutritional ICD predisposition to frequency as a comorbidity for specific fracture groups will also be evaluated. Unique osteopathies are expected to impact these results for certain age groups and perhaps income levels for patients. MCD, MCR and non-MCR/MCD program patient populations will be compared.
RESEARCH TOPIC 11
Cultural Richness and Diversity
Research Questions: What are the social, cultural and/or ethnic groups settings contained within the five boroughs of New York City? In particular, are there specific zip code tracts and census block areas that may be evaluated in order to develop the tools needed to profile patient health at the community level?
More than likely, a number of ethnic or cultural communities exist within [the] City that serve as valuable research settings, for projects similar to those made famous by the Alameda studies carried out in Los Angeles, California over the past several decades. For example, the most famous community-cultural settings in the some of the larger urban settings include communities rich in a cultural heritage, and language and mercantile behaviors closely linked to specific groups, such as the local “Little India”, Jamaica, Chinatown, Spanish Harlem, Black or African American Harlem, Hassidic Judaism, Russian-based Judaism (——), Middle Eastern Muslim communities. This project explores the following ethnicity or culture related research questions: What are the demographic and business related indicators of these community settings? The business indicators? The related healthcare provisions that are unique in nature? Another serious of questions to be explore are those which focus on health care provider locations and activities. This includes a review of foreign language background, the availability of medical documents in the most appropriate foreign language, the types and amounts of healthcare provides that service these neighborhoods, their cultural specificity and appropriateness. The presence of any unique services or public health related requirements and demands posed by these unique cultural settings. The purpose of this study is to document the unique demographic and sociocultural features of the populations serviced by these ****** facilities, and to ultimately use this information to provide more highly targeted, culturally-linked, culturally-defined healthcare services.
RESEARCH TOPIC 12
Culturally-defined Special Service Needs and Requirements
Research question: Why are there differences in age-gender population distributions for male versus female patients, diagnosed as either a sickle cell disease patient and or a sickle cell carrier?
The diagnoses of sickle cell and being a sickle cell carrier can have a tremendous impact on how a patient makes certain decisions about lifestyle and life goals. The presentation and diagnosis of either of these two conditions is different for women and men. For the disease itself, sickle cell has similar impacts upon men and women, with women possibly experiencing better chances for survival through their mid-life years (40 to 60s) than men. For the carriers, preliminary results suggest that the risk of survival through the midlife years is considerably less for men than for women. More importantly, female carriers of sickle have an ability to survive through their reproductive years, a disease behavior not noted for male carriers. The reasons for this asymmetry are uncertain. It is possible that late diagnosis of the condition may be responsible for women peaking in their reproductive years for diagnosis of this condition (genetic screening related to childbearing potential preventive acre work). This explanation does not apply to older male carriers, who seem to reduced greatly in numbers by the time they reach 40 years of age. These unique population–related features of sickle cell disease and carriers are in need of further exploration. Either a focus group or case study methodology is recommended in order to determine if there are statistically significant differences between female versus male case or potential carrier case management practices.
RESEARCH TOPIC 13
Research questions: Is there a difference between two groups of patients either diagnosed as having sickle cell or diagnosed as a sickle cell carrier, when these two groups are defined as having either an African Americas heritage or a Hispanic heritage, according to EMR documentation?
A major concern about electronic health and electronic medical records data is the validity or truthfulness of these data. A review of the EMR/EHR has revealed two primary demographic groups identified with documents revealing either a sickle cell disease or sickle cell carrier related diagnoses—African American, and Hispanic. Very little research has been performed on the sociocultural impacts of being diagnoses with a disease that has significant quality of life and longevity related implications. The diagnosis of having a sickle disease or being a carrier impacts the decisions patients make regarding family planning, engagement in further healthcare related activities, and the value that may be place by the patient upon healthcare providers, agencies, insurance programs, and long term lifestyle related living practices and activities.
To study this outcome a focus group approach is recommended in order to document the different interpretations these two cultural settings experience when faced with such a diagnosis. The number of patients who checked the “Hispanic” box for ethnicity are very few in number for our patient population. These suspected cases may be a result of patient entry error, patient choice of race related errors, data entry by technicians, or a “more than one race” related error. For patients whose lifestyles are truly Hispanic in nature this offers a unique opportunity to closely evaluate how the interracial passage of a genetic disease like sickle cell impacts the patient. Hispanic patients who live a traditional Hispanic lifestyle without much influence related to African-American beliefs may experience this diagnosis differently from combined maternal-paternal African-American couples. This study reviews and interprets the culturally linked patterns of behavior, related to the culturally-bound reactions and behaviors that may exist for a sickle cell disease or carrier patient diagnosis.
RESEARCH TOPIC 14
Research question: What are the relationships between religion and race with regard to the documention of spouse abuse cases, in which the abuse victim is the adult women or wife?
A preliminary review of ICDs for the adult abuse code revealed disproportionate findings for the number of abuse cases documented through EMR/EHR databases. Documentation of the ethnic background and religious affiliation of cases identified within the databases revealed distinct differences between the subpopulations that could be identified. Not only was the absence or presence of these codes for groups different, the numbers of events or visits accounted for at the per patient level appeared to be significantly different as well. This study is a further exploration of the use of this class of ICD data for analyzing population health features and producing very specific programs when needed to deal with such events as they appear in the EMR/EHR data. A well-targeted case study approach is recommended for this project, requiring gender sensitive researchers and assistants be engaged in this case review process. Female nurses, social workers and counselors are recommended for this project, which may be used to design a better targeted spouse abuse prevention program.
RESEARCH TOPIC 15
Culturally-bound Health
Research questions: What are the culturally-bound health conditions that may appear in clinics? Are these adequately documented? (unanswerable) How can we identify them as the happen and therefore improve their documentation and treatment processes?
This is an ICD 10 study, with comparitive studies performed as well for prior ICD9 diagnosis for the same patient groups. Database used: 10-20 years, all EMR. A thorough study of cultural-bound health is lacking in the medical literature pertaining to managed care programs. This study applies the basic studies and methods of research utilized primarily by medical anthropologists and social services agencies to a culturally diverse managed care population. The cultural richness of this combination, in combination with its sizeable populations and vast amount of community, cultural-related services provided for complimentary healthcare practices within this region, provides ****** with one of the most unique opportunities to fully explore this important managed care research topic. The following are examples of ICD10’s for culturally-bound syndromes, noted to exist by other allopathic care programs and agencies. The related culturally-bound syndromes for each of these ICD10 diagnoses are listed. Possible ICD9 codes that may relate to some of these diagnoses are provided in parentheses. Other related ICD10s are also defined for each major group reviewed.
- F32.11 – Moderate Depressive Episode with somatic syndrome (ICD9 296.2 or 296.3?). Example: nerves (northern Europe), nerfiza (Egypt), nerva (Greece), nervios (Mexico, Central and South America). Possibly valid for ataque de nervios (Puerto Rico, Latin America), colerina (Andes, Bolivia, Columbia, Ecuador, Peru), ich’aa (Southwestern US Idigena), berserkergang (Scandinavian, Saami), carfard (Polynesia), benzi mazarazura (so. Afr. Shona), ahad idze be (New Guinea). Related also to anfechtung (Hutterites), brain fag (Nigeria), colerina, pension, bilis (Mexico, Central and So. Amer.), hseih-bing or xie-bing (China), hwa-byung (Korean peninsula), qissaatuq (Inuit), narahati-e a sa and maraz-e a-sab (Islamic Republic of Iran). Considered partially linked to cultural stress due to low self-esteem. Experienced by women more than men in some cultures. These have also been related to F48.0 and F45.1.
- F40 – Phobias. Examples: taiijin kyofusho, shinkeishitshu, and anthropophobia (Japan). Afflicts younger people. Perfectionism, oversocializing, events related to inferiority complex issues are noted. Akin to adolescent acceptance behaviors.
- F40.2 – Social or Specific phobia(s) 1) Examples: pa-leng (China, fear of cold winds), agua frio, aire frio, and frio (Mexico, Central and South America). American terminology example of the temperature based philosophy (weakness, weak body or weak soul) includes frigiphobia. Cultural basis is fear, anxiety, obsessiveness, related to the underlying humoural implications. [Possibly ICD9=300.2, 300.2*] 2) Hwa-byung (Korea) is similar, with the exception that it is termed a “Firey Illness.” Anger and rage are manifested, with changes in somatics, autonomics, and mood. Woemn more than men. Related to cultural oppression. Has some rage-like features.
- F40.8 – Phobic Anxiety Disorders [see 300.23 social phobias] Continuation of the F40 series. Examples: taiijin kyofusho, shinkeishitshu, and anthropophobia (Japan). Other possible associated diagnoses: anfechtung (Hutterites), itiju (Nigeria).
- F44.3 – Trance and Possession Disorders. Examples: possession disorder, saka, ufufuyane (So. Africa, Bantu- Zulu, Kenya). Akin to a Voodoo spell. Some relations with “magic” and stupor, seizures, trances. Scientific profiles include drug use suspected. Young unwed women are most susceptible. Related as well to aluro (Nigeria), phi bob (Thai), and zar (Egypt, Ethopia, Sudan).
- F44.7 – Mixed dissociative (conversion) disorders. Examples: pibloktoq (Inuit), uqamairineq (Inuit), possession disorder. [ICD9=300.1*, 300.11] Seizure like behaviors. Multisensory hallucinatory events. “Soul loss” experience is common event. Soul wandering is one interpretation of this event, that tends to occur in older kids and young adults. Very much psychosocial in nature in terms of defining purpose and meaning, and assigning “power” to a young potential leader’s “purpose” within his or her group.
- F44.8 – Other specific dissociative, conversion disorder. Examples: latah (Malaysia), pibloktoq (Inuit), uqamairineq (Inuit), old hag (Newfoundland), phii bob (Thai), aluro (Nigeria). [ICD9=300.1*, 300.11]. Inuit feel it represents “soul lost” or wandering. Dissociative hysterical cases occur. Seizure like manifestations may ensue, followed by drowsiness (sleep paralysis).
- F45.1 – Undifferentiated somatiform disorder. Examples: susto or espanto (Mexico to So. Amer.), nerves (var.). ICD9 closest is possibly 308.* “Soul loss” generated by the supernatural. Social stressors may be related. Related to lanit (Philippines), latah (Indonesia, Malaysia), malgri (Australian aborigines), mogo laya (New Guinea), narahati (Islamic Republic of Iran), and saldera (Amazonia).
- F45.34 – Somatiform autonomic dysfunction of the genitourinary system. Examples: koro (Hainan Island of China, India, Singapore, Thailand), suk-yeong (Cantonese), suo-yang (Mandarin), jinjinia bamar (Assam), rok-joo (Thai), rabt (East India). Anxiety and panic are some of the basic S/S, sense of coldness, retraction of body parts (penis) as a result. Linked as well to F48.8. The ICD9 closest to this is 302.7*-psychosexual dysfunction, 302.72-impotence,frigidity, and 302.73, 302.74-anorgasmia. Possibly 306.* The koro (Hainan island of China, India, Singapore, Thailand) may be associated with this as well. [See f48.8]
- F48.0 – Neurasthenia. Example: nerves. Possible shenjing shuarino (China), when patient is afflicted with a sense of mental and physical exhaustion, memory loss, inability to concentrate, irritability, headaches, weakening of nervous activities or nervous system (“neurasthenia”).
- F48.8 – Other specific neurotic disorders. Examples: dhat (India), koro (Orient), latah (Malaysia), jiryan (Assam), shen k’uei, or shen-kui (Oriental), amurakh (Siberia), iekunii, ikota, okan, myriachit, menkeiti, (var. Orient), Lapp panic (Lapps/Sammi), bachtschhi (Thai), imu (Ainu indigena or Japan), mali-mali (Philippines), silok, susto (Mexico), yuan (Myanmar, formerly Burma), jumping (French Canada). One part of this philosophy relies heavily upon the spirit of life concept. Therefore, one route taken for this disorder and diagnosis is the belief in chi, which is found in ayurvedic and Oriental health philosophies, and possibly unaniism. The four humours, five elements theory plays into this, and the loss of chi via semen reduction is important to the cause. Shen is the spirit of life (Chinese and Japanese), expressed as “the sign of life” in a patient’s eyes. This has been associated as well with F45.34. Due to the primary sexual and “energy” nature of this condition, Western medicine identifies it with sexual neuroses. Echopraxia, echolalia are also predominant behavioral symptoms.
- F48.88 – Other specific dissociative (conversion) disorders. Examples: susto (Mexico). See F44.7 (pibloktoq, Inuit).
- F68.8 – Other personality disorders of adult personality or behavior. Examples: amok (Malaysia), windigo (NE Native Amer.), hseih-ping (China), sar (Egypt and Sudan). Possible ICD9: 301.5? 301.50?. Windigo is an obsession, which can include cannabailistic ideology, and belief in being taken by nature’s “monsters”. Once related to starvation history, now more behavioral and obsessive in nature. Possibly akin to ostracizing and trying to prove one’s self to peers.
- G47.4 – Narcolepsy and catalepsy (incl. sleep paralysis). Example: uqamairineq (Inuit). (ICD9=306.0). This may be too off-base for culturally bound behaviors and diagnoses. A diagnosis of false epilepsy is more fitting.
Also:
- Epilepsy – “Spirit Captures you and you fall down” (Laos, Native American)
- Schizophrenia – Amish
- Sudden Unexplained Nocturnal Death Syndrome (Laotians)
Preliminary studies demonstrated possible somatic-autonomic links for culturally-bound syndromes seeming to impact the heart and circulation, for example Obscure cardiomyopathy of Africa (452.2), Asian pseudo-RBBB or Brigada Syndrome, Takayasu’s Disease (Japanese) (446.7), Japanese Moyamoya (vessel disorder), Takotsubo (429.83).
The following behavioral psychology ICDs were considered possibly linked to culturally-bound syndrome behaviors and diagnoses:
- 290.* Dementias
- 300.* Anxiety states
- 300.02 Generalized Anxiety Disorder
- 300.1 Dissociative Disorders
- 300.11 Conversion Disorder
- 300.13 Fugue
- 300.14 Identity
- 300.16 Factitious Disorder
- 300.21-.22 Agoraphobia
- 300.23 Social Phobia (301.7 Antisocial)
- 306.2 Acute Physiological Malfunctions of the Heart due to Mental Factors (306.8 bruxism, 306.6 endocrine)
- 307 Sleep Disorders (307.45 Circadian, 307.46 Arousal)
- 307.46 Sudden Affective Disorder (SAD)
- 308 Acute Reaction to Stress
- 309.4 Emotion and Conduct Adjustment Disorders
- 309.21 Separation Anxiety
- 309.29 Culture Shock
- 309.81 PTSD
- 309.* Adjustment Disorders
- 309.1 Prolonged Depression
- 310.1 Personality Change due to . . .
RESEARCH TOPIC 16
Culturally-Linked Health
Research question: Are there Unani health care communities in the five boroughs region? How do we identify them? Do their patient population and related health issues and health prevention practices result in a unique healthcare burden for the traditional allopathic care programs and health insurance available to these communities?
Unaniism is a unique practice engaged in by a special class of practitioners found in parts of Indian, and the Iran-Iraq portions of the Middle East. Unaniism is a very unique form of medicine in that it is of ancient Hippocratic decent, with certain Hippocratic medical practices definitive of modern western medical practice (allopathic) philosophies, and yet is practiced in a more traditional form in a number of very non-Western, non-allopathic health care settings. The primary burden a non-western practice such as Unaniism might result in is the application of its traditional practices an beliefs a priori to the allopathic care practices and procedures covered by traditional health insurance programs in the U.S. This community-focused exploration of non-traditional allopathic health care focuses on culture, culturally-distinct health care service programs, over the counter healthcare services and products, and the density of these healthcare clinical and non-clinical resources in the local community. Two distinct cultural groups are identified as strongly linked to Unani healthcare practices—Muslim or combined African-American-Muslim communities and Indian or combined Indian-Muslim communities.
Note: Assume that Culturally-based studies always require special IRB processes. Studies related to the above at the ICD/EMR level are expected to produce some follow up queries. At the clinical level, special case studies and focus group approaches may be needed. Due to the diversity of cultures and types of manifestations of these diagnoses, small groups may not be available, suggesting in turn that a case study approach may need to be taken. The research processes, and steps taken to develop this knowledge base, need to be documented further. More examples of this type of research work that have already been engaged have to be uncovered and reviewed.
MAJOR THEME – SURVEILLANCE
RESEARCH TOPIC 17
Surveillance
Research question: Could a problem resembling the recent Legionnaire’s disease happen again?
A review of the infectious diseases and their spatial behaviors, based upon events, cases, and various public health related environmental-ecological reviews of infectious disease data.
Three components: i) Cooling Tower technology and maintenance; ii) local weather and climatic state; iii) human transportation.
Applying the Asiatic Cholera approach to interpreting this, as detailed in my thesis, there are the following stages to consider: a) initiation stage: initiation of an ecological setting for pathogen to survive and develop (cooling tower); b) incubation stage: environmental features responsible for allowing the organism to remain viable, and potentially spread at a later time once population counts are increased; c) facilitation stage or event: development of an important event that enabled initiation of the outbreak to be possible (meteorological, seasonal, topographic, climatic); d) exposure stage: initial contact of potential victims and pathogens (normal or unusual daily processes in the environment); e) pathogenetic stage: successful spread to one or a few victims; f) diffusion stage: diffusion to new sites (transportation, commercial transport defined by company and industry in this case; g) perpetuated transport/diffusion stated: additional facilities found to be contaminated were directly linked to the original business, suggesting routine transport between facilities, provider or patient transport programs, facilitated the spread to facilities outside the immediate area (this latter facilities is barely revealed in the reports.)
RESEARCH TOPIC 18
Politically-based in-migration and Public Health
What are the unique stresses that the influx of Middles Eastern, NE African cultures might induce upon the ****** system?
A similar evaluation was performed extensively on the influx of Vietnamese, Laotians, Hmong, and Cambodians into the US during the 1970s, due to the Vietnam War. The processes social services engaged in to prepare for this influx of new patients were documented. The unique stresses this placed regarding public health, personal physical health, personal social health and personal behavioral health were documented at the time, and then re-reviewed and summarized in a separate study completed around 2001/2. The protocols learned from that study will be applied to this particular ethnic group.
RESEARCH TOPIC 19
Research question: What is the distribution of antibiotic resistant organisms within the five boroughs settings, and their related healthcare facilities and patient populations, focused on a review of emergent care patient results versus patients engaged at least one hospital stay during the year?
This study was first proposed by the Emergency Department and the ***** County Hospital, and focused on a review of E. coli test results, for comparison between in-patient (IP) and emergency patient (EP) populations. IP and EP patients may be differentiated by a column in which this data is provded, and the length of stay [LOS] the patient experienced for the emergency care encounter. A LOS of less than 2 days was used to define EP eligibility for this study, to avoid patients who were hospitalized for any significant lengthy of time due to their visit. The original study focused on one healthcare facility, one bacterium test, for an undetermined number of prescription antibiotic medications. The result for each evaluation made included information on the medication tested for antibiotic resistance, and the result of that study entered as either ‘resistant’ ‘not resistant’ or ‘undetermined’. This study will be re-performed adding zip code data to the analytic process, and applying the entire algorithm and data interpretation process to all of the networks, regions and facilities involved with ****** programs. The four ACO facilities, specialized care facilities, and long term care facilities are excluded from this work. This process may be used to identify clusters of antibiotic resistant behaviors, geographically, institutionally, demographically, and perhaps socioeconomically.
RESEARCH TOPIC 20
STD rates
What are the current rates of STD diagnosis, in narrow band age groups, for the city, its networks, acute care facilities, pediatric versus family medicine practices, individual zipcode tracts?
This is a follow up to the recent news indicating there is a resurgence in STDs in high school populations and young adults. The goal is to evaluate population health features, including age band/sip specificity, for syphilis, gonorrhea, HIV/AIDs, Chlamydia.
Note: The processes developed for this work could be applied to any subsequent ICD focused surveillance projects engaged in.
A separate study is in the works, reviewing the local history of HIV/AIDs and paralleling the initial studies produced by Daniel Fox, SUNY-StonyBrook, Exec., Chief Editor Milbank Quarterly.
RESEARCH TOPIC 21
Fetal-Perinatal Health
Research question: Are there particular indicators of the quality of perinatal events experienced in ******?
The following groups of ICD indicators are under consideration for this study.
ICDs 760 to 779 cover perinatal period health conditions (evaluate using BETWEEN ‘770’ and ‘779.99’). The 760 series reviews developmental conditions related to the development period, but not the development process, such as fetal exposure to alcohol or drugs, factors experienced by the fetus but related mostly to maternal related problems, large baby. Gestational events are evaluated by the 764-766 series; size, growth rate and malnutrition are partially evaluated with these values. 767 refers to birthing process trauma, indicators of PCP skills and maternal participation activities. Post-birth respiratory problems are indicated by the 768 to 770 series, with respiratory distress syndrome and meconium aspiration its most important features. The 771 series refer to infectious diseases. 772 refers to hemorrhagic conditions, blood endocrine dyscrasias, isohemolytic disorders, jaundice related conditions, and hematological disorders. Internal organs and integument problems result in 777 and 778 series diagnoses. Other generally more severe problems are noted in the 779 series.
The 630 to 679 series refer to pregnancy, childbirth and puerperium related diagnoses. 632 is ectopic pregnancy. 636 is illegal abortion, 638-failed abortion. Risk of early termination (640-641) may not related to human behavior induced risks. Hypertension leads to the 642 series of complications. 643 refers to pregnancy related vomiting. The series 644 to 647 are high risk indicators (BETWEEN 644 and 647.99, but see full list for details and decimal additions): 644 refers to premature delivery, 645 systems problems perhaps chronic disease related, 647 and 648 refer to infectious disease rates and congenital development related problems. 649.0 is tobacco use during pregnancy; 649.1 is for obesity as a complication.
The 650-655 series may not relate to risk assessment processes, because they are “natural” and unpredictable complications that develop, for the most part. 656 refers to mother-fetus (Rh) complications. ICDs ranging from polyhydramnios (657) to abnormal fetal heart conditions (659.7) are useful for risk assessments (BETWEEN 657 and 659). 660-669 are labor related complications. 670 to 676, and 678 to 679 are also complications that may not be preventable.
Note: Any Role for Neonatal thrombocytopenia (287.4, *)?

{kind=link}