May 2016
Monthly Archive
May 30, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Religion: A New Dimension in Disease and Public Health Mapping
Over the past few weeks I have been ranting about the fact that the current managed care system has advanced little over the past 10 to 15 years. In fact, the first articles on the barriers to developing an electronic medical records system so essential to the managed care environment were published fifteen years ago. Today, many of these problems remain. The only thing that has changed is that information technology software programs and packages have improved, the amount of data that a data warehouse can store has increased significantly, and the speed at which ‘Big Data’ analyses can be carried out has improved substantially.
When you turn to the LinkedIn posting on IT, you’re left with the impression that this is a rapidly advancing field, with the ability to bring US health care programs to the next generation of due to progress.
Well, if you take a look at the accomplishments of most programs, you are more than likely going to see managed care programs still struggling to demonstrate success with their programs. Should this success be in the form of highly successful meaningful use measures, or important changes in population health features, there had better be a few of these “accomplishments”. After all, a typical program is evaluating between 50 and 150 metrics to document its accomplishments. Only some of these are reported. None of these programs (to my knowledge over the past 4 years) produces a thorough ‘Quality of Care’ or ‘Quality Improvement’ analytic program, measuring all or many of the accomplishments of the past years worth of healthcare efforts, and then maps the most significant of these findings. (Such is a reasonable goal, and product, for a HIT-GIS program.)
Knowing how to program your system to make such measurements is 90% of the work; its focus should be on the quality of care/quality of service (QOC/QOS) process for a majority of disease patterns in the region. The reasons such steps are not taken relate mostly to poor planning and administration. These processes could have been decided upon, planned, implemented, expanded and made more efficient in 2005, the year that the content of a valuable meaningful use program could be defined, a time when such a program referred to as a quality improvement [QI] program became a requirement.
There are several reasons managed care programs have not implemented a data warehouse setting in such a way that a spatial analysis technique can be applied, or added to an institution’s QI program with full scale implementation of a GIS.
First, there is no official policy or recommendation that was ever put into place for the implementation of spatial analysis techniques as part of a new meaningful use, quality improvement program.
Second, the skillset for implementing such a program is lacking at the leadership and administrative level. This lack is because directors, managers and administrators failed to hire the type of human resource needed to implement such an innovative program.
Third, even if individual exist in a healthcare system whom are capable of producing highly useful monitoring and intervention maps, the know-how for implementing a new program based upon these findings is also lacking, a blame we may once again lay on the administrators.
So meanwhile, as the Health Information Technology [HIT] departments at most institutions struggle to make old and new outcomes match, and develop a database that is not only consistent but highly worthwhile for monitoring managed care population health, it is best for those already working in their system to take on the next most important research question in managed care.
Can religion be used to evaluate population health, and if so, how do we make use of this unique form of datum?
Religion provides us with equally valuable if not more insight when compared with ethnicity and race data. Ethnicity can be used to search for social inequality and language related barriers involving the most predominant patient ethnic group in the United States. Race provides us with insights into how socioecononic status/poverty, and race and race-linked genetics can impact a populations health features.
What religion tells us can serve as a further clarification of race-related findings for illness and disease. Religion also adds to the insights we receive from the ethnicity work engaged in.
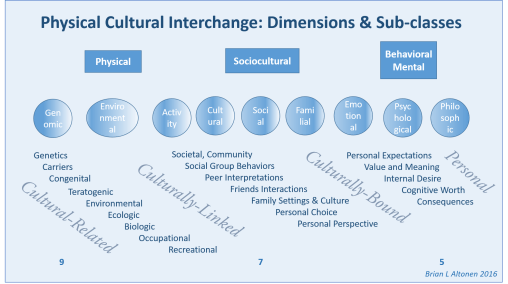
I have identified 9 physical science, 7 social science and 5 behavioral science and/or mental health topics that are closely linked to diseases and the medical disorders people are diagnosed with, in such a way that if these lists were related to the therapeutic processes engaged in for any ICD-defined medical/health state, the results of this interpretation of each ICD should enable us to define those which are most linked to a particular religious culture.
Elsewhere on the web, I have identified the various types of cultural disease patterns that exist, based on the current ICD systems. There are well defined culturally bound diseases, rarely mentioned culturally-linked disease patterns, frequently mentioned culturally-related health conditions and disease patterns involving the physical body.
Specific religious groups infrequently overlap with their disease patterns in United States cultural settings. There is the majority of diagnoses that are ubiquitous to population health, which individuals of all race, culture and religion experience. But there are also specific diagnoses and health problems that occur due to culturally-related human behavior habits. These are the topic of this review.
Using the standard research theory models, like Health Belief Model, to understand how people react to a medical condition, the above figure can be related to that model and the primary dimensions, subclasses and behaviors linked to a disease can be identified. Then a more effective and thorough intervention program may be developed and specifically targeted.
A “meaningful” managed care system assesses the entire population for all of its healthcare needs. This model enables planners to develop a balanced program devoted to physical, behavioral, mental and social care processes. It can be used to define when and where focus groups are needed, what populations to target with a survey, where to look for unexplored ICD related topics for you particular population, and how to improve the intervention planning process for conditions that aren’t effectively treated at the moment.
Consider each of these elements a question that has to be explored in order to fully understand the causes for certain non-physical, behavioral, social and cultural behavioral disorders and/or disease patterns.
May 23, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Another Interpretation of Epilepsy – – will we be ready?
Introduction
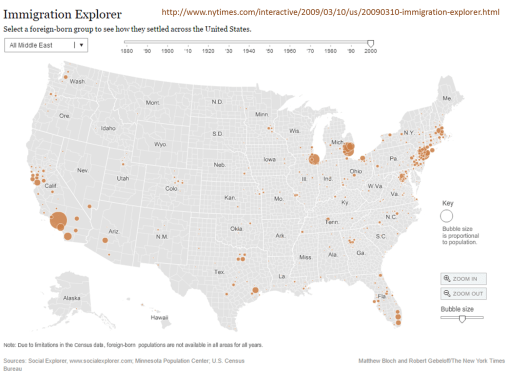
With the migration of settlers from the Middle East, Arabic medicine will soon be impacting Western medicine or allopathy. This influence will be in the form of Unani-Tibbs medical practices.
To understand this impact of a newly arriving medical belief, consider the impact that Asian migration has had on the U.S healthcare system since 1830. Whereas there was plenty of migration between the mid-1800s and late 1800s, it wasn’t until well established oriental communities were formed in urban settings, with enough local consumers, in the form of Asian families, available to support a growing medical business devoted to traditional Chinese medicine.
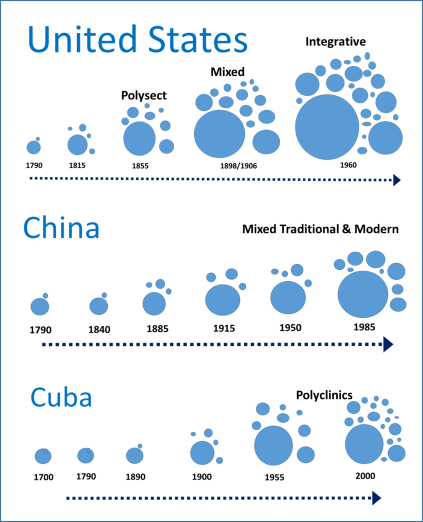
From an older essay comparing these three programs
Oriental Medicine in the US
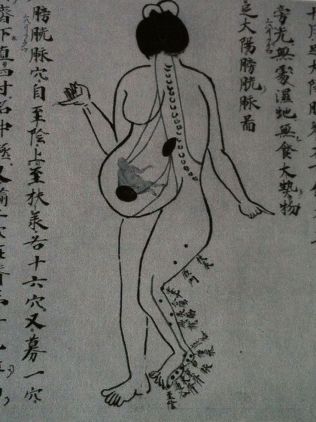
Within western cultural settings, there have been several stages when parts of the oriental philosophies came to be common practice by western doctors. Most of these methods tried and accepted required some form of western philosophical paradigm to improve their likelihood for acceptance and integration into Western Medicine practice. The most recent examples of these many non-Asian United States citizens are aware of, like the practice of acupuncture and acupressure, the use of ginseng for strengthening the body, ginkgo for the mind.
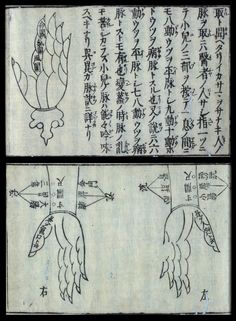
Yet there are parts of the Oriental philosophy which we struggled to develop philosophical interpretations for. One of the earliest Oriental practices noted and almost accepted in western European writings was the use of moxi, a smoldering stick consisted of pressed sage leaves that maintained the fire but not the flame—its purpose: to heat a specific area of the skin, add energy or chi, and improve the vitality of the body there, assist in the flow of its energy from one part of the body to the next, through this area that served as a node or place where such flow could be strengthened.
The acceptance of moxi, more as a curiosity noted in the earliest oriental travelers recounts, initiated as early as 1650. To make sense of it in the traditional four humours paradigm of western medical philosophy, the writers termed it a way to add fire to the four elements that needed to be in balance within. Yet, there were other theories that could be used to explain how Oriental medical practices made sense, many based on the observations made about electricity and the body.
The other practice sometimes reviewed by writers in their recounts of China was acupuncture. To understand acupuncture required a knowledge fo the how the body was shaped, and then how these particular moxi points were distributed across the body surface, and how without heat, but only through the use of a very thin needle, these points could be changed with a barely visible perforation of the skin. This view of the acupuncture needle process seemed counter to the much cruder, more injuring practice of lancing the body, in order to let the blood flow, in the form of the practice of bleeding or bloodletting.
The Western paradigm stated that a certain amount of blood had to be removed, to remove the bad humours within and give room for newer, more healthy humours to form and fill this empty space in the vessels. That philosophy was much easier to visualize and understood, and was accepted as true by Western Doctors, whereas the acupuncture theory that was suggestive of energy flow rather than fluid blood flow, had less evidence to base itself upon. Lanced blood was more convincing than theoretical energy released and allowed to flow freely elsewhere in the living body.
When electrotherapy had its first discoveries, the similarity of these early phenomena to the claims linked to moxi-generated heat and acupuncture-generated energy could be equated with parts of the western medical theory for electric cure. The first form of electricity this related to was equivalent to the concept of the battery, with energy stored in the form of static electric change, stored and held by the Leyden jar, an early form of the capacitor. If one grasped the right wire atop the Jar, a shock was felt, an electric charge, that could in theory “revitalize” the body, and in the realest sense, recharge a heart that has stopped beating. The witnessed evidence that leyden jar and static electric charge production and discharge could revitalize a living thing, was the use of static electric generators to cause a muscle to twitch, to make a seeming dead muscle in a young child paralyzed by a disease like spinal meningitis contract again, offering help to the crippled child and his parents.
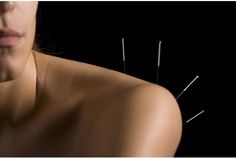
The Oriental philosophy of how energy worked in the body, the power of Chi, wasn’t exactly equivalent to the Western medical paradigms upon which certain regimens were discovered and then added to the philosophy at hand. It wasn’t until the 1830s that later stages in the development of the use of electricity, in particular in the form of stored galvanic electricity, led to another rendering of the use of acupuncture to help patients. The acupuncture needle became a medium through which energy flowed, out and across the chi pathway in the sense of oriental methods for its use, from the energy source into the body in the allopathic electric cure sense.
The other forms of Chinese medicine that came to be popular were mostly related to herbs. Ginseng was mostly worth what it was to the Chinese people. But similar tonics could be found in United States treatments that were akin to the Chinese tonic medicines. The occasional overlap between Chinese medicine and Allopathic medicine did happen in the early 19th century, but its impact on the acceptance of traditional Chinese philosophy in general was minimal. Oriental medicines like the Ailanthus glandulosa (Tree of Heaven) became popular because its stench worked against the miasma, not due to an energy it helped to generate in the body to help heal the patient and strengthen a patients defense again sickness. The Chinese ginseng had its American equivalents, but they cost the price of a great medicine, not an aged root worth more than its weight in gold due to its form, age and twisting spiraling nature. A root was simply a root in Western medicine. The purest whitest powder of a starchy Smilax tuber was appreciated due to the nature of it starchy content and its value in preparing formulas, not its symbolic purity.
“Modern” Philosophies and Traditions
The latest rebirths of Oriental medicine, (there were several) came in much the same manner that other forms of “alternative medicine” have come to be practiced. There was this tremendous dissatisfaction with the standard allopathy for the time—people were in need of safer and more trustworthy methods of treatment and cure. During the late 1890s and early 1900s, Oriental medicine was practiced heavily in American office, by Oriental practitioners, sometimes in association with American non-allopathic MDs. The bacterial theory had caused a major eruption in heathcare, enabling non-allopathics to briefly get a hold of the reins once again. If it weren’t for improvements in licensure laws at that time, many of these philosophies might have been here to stay.
But many medicine philosophies were put to the test by the regular medical profession around 1900s. The 1906 Food Act helped further this attitude about health, as did the 1915 Food and Drug Act, which effectively got rid of unfounded or unsupported over the counter drug based remedies (i.e. over the counter opium in treatments for teething babies). Since then, many of the 19th century allopathy skills have since vanished from the medical books. The allopathic standards of leeching, blistering, and bloodletting were the first to go, followed by the excessive use and reliance upon rubefacients and other irritants that in theory were working as “counter irritants”. There was also the reliance upon unusual tools such as the baunscheidtismus contraption, mean to apply the equivalent of many irritants, numerous lances, all in one spot. This elimination of the serious irritant, however, did not completely eliminate the perceived value of the acupuncture needle from Oriental medicine.
When Mao Tse Tung showed the world that acupuncture could be used to perform Open heart surgery in his primary teaching hospitals, the United States and United Nations observers of this practice were not only stunned, they were amazed, and convinced of its success. Chinese medicine has ever since had its periods of acceptance and then rejection by western practitioners, until recently, when allopathy finally decided to include it in the possible treatment paths for specific therapeutic pathways they were unable to be successful with—alcohol abuse, drug abuse being the most prominent, but the treatment of certain chronic diseases like ileal paralysis, chronic back pain and HIV or AIDs infection.

Middle Eastern Unani-Tibbs Medicine
Are the same things that happened with Traditional Chinese Medicine and United States medicine about to happen with Unani-Tibbs medicine?
More than likely yes, but for different reasons.
As the number of families from the Middle East increase, those devoted to practicing their own unique forms of medicine known as Unani-Tibbs will become the standard (if it isn’t already the standard for some community settings). It is possible that the transition of small social settings from western the Sharia Law will provide insights into where these transitions will first take place, and where they will first have their impacts on patients receiving both Unani-Tibbs and Allopathic forms of medical care.
The most important parts of these other forms of medicine that may become a standard in some western medical-integrated healthcare systems are the ways in which some diseases are interpreted, etiologically explained, and then treated. What we learn from how Chinese medicine was introduced into Western Medical practice paradigms may relate to how we should view, study and interpret what events are happening as Unani-Tibbs medicine becomes more popular, and more common.
Like Chinese medicine, Unani-Tibbs medicine does have its own unique way of interpreting the cause of disease, the meaning of diseases, the developmental processes responsible for disease onset, and how to treat and eliminate the disease. Like Chinese medicine, Unani medicine has its more direct, and perhaps reliable and trustworthy applications, at the cultural level, treating behavioral health and psychologically related or induced states, by basing these treatments upon traditional cultural paradigms.
But what about diseases that are mindbody-like in their behavior, those which during the 1940s and 1950 (and even 1960s) we called “psychosomatic diseases”? Irritable Bowel Disease and Fibromyalgia are two very common examples of this. Might other versions of treatment for these long-lasting chronic conditions be beneficial to some patients?
One of the best examples of these conditions which has a very social and cultural definition attached to its seriousness and meaning is Epilepsy. Epilepsy is a prime example of a disease that has different interpretations across different cultures, and perhaps even requires different methods of treatment depending upon the source of the paradigms that guide the lives of specific patients diagnoses with epilepsy.
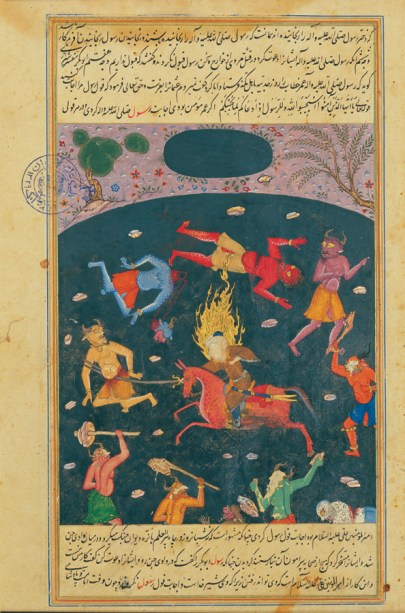
Djinn, or Jinn
Epilepsy Causality
Like the theory of humours, epilepsy has this long history of definition and redefinition of its cause and treatment over the millennia. Western medicine, Asian medicine, and Middle Eastern medicine have been involved in how we developed our current perceptions of the patient with epilepsy, especially in his or her uncontrollable or intractable state.
Vitalism – – the Western Medical theory of life energy in 1800 +/- 10 yrs
In the past, western medicine has dealt with the notion that epilepsy is related to some “invasion of spirit concept”. Hippocrates taught that to us, as well as Chinese and Native American doctors and healers. The unexplainable nature of the seizure, and the appearance of the invasion of other beings or demons into the human body, is a cross-cultural paradigm assigned to explaining certain seizure types. The New Testament attests to many examples healed by numbers of healers during their pre-sanctification phase or existence. This same story, so common to most leading religious writings, is curiously absent from the Koran, the reasons for which are in dire need of a professional theological and medical review and the publication of any intense speculation that may arise due to this research by the best scholars in the world.
But until then, we have to deal with the reality of epilepsy—that it exists, and that it impacts Muslims probably as much as it impacts most other populations. If epilepsy is an unusual example of culturally-bound disease pattern, like some of my past writings have suggested, it exists because western medical philosophy allows it to exist, allows for its related behaviors to happen, be interpreted the way they are, and then diagnosed as expected.
As a historian, I always though it curious as to how and why past forms of epilepsy are different from the standards we believe in today. The hysteric convulsion, the French diagnostic categories of seizures were very different from those we believe in right now. They seem to be mostly presentation and symptoms based, relying heavily upon the patient’s appearance and affect during the seizure episode. And when you read some of the severest events as they happen, you have to wonder why they were more often considered a form of sleep walking or somnambulism, or some sort of hallucinatory state like those induced by medicines, or those initiated by the animal spirit in the human body, its emotional system and emotional reaction to the stimuli at large in life, home and society.
Islamic “Treatment of Spirits” (Djinn)
Middle East Interpretations
With patients from the Middle East, they have a unique spiritual and physical medicine interpretation of epilepsy that must be adequately approached by the western physician or neurologist unaware of Islamic beliefs and faith regarding the seizure. That will likely not happen, unless the primary care giver is Islamic himself or herself.
The primary reason a child is brought to the doctor for possible epilepsy, is that the family and closest associates need to know if it is of djinn origins or physical origins.
At first, this seems a very easy problem to deal with. The provider has to convince the parents that the seizure is what s/he (the allopath) thinks or believes it to be. But try to convince a different culture that this interpretation is true.
There is a transition going on in Unani-Tibbs medicine just like there was when Oriental medicine was put under the lens during the late 1800s. We will see transformed Unani-Tibbs trained MDs who are convinced that this traditional path does provide unique opportunities to better a patient’s life. We will also see Unani-Tubbs trained physicians who have moved away from the traditional philosophy and try to lay to rest the fears that riddle the families receiving western medical care who are so concerned about the roles and reasons related to the “evil” forms of disease onset that they experience, and yet no other culture does, in terms of how they interpret it. We will also see traditional MD allopaths, perhaps even of Middle Eastern descent, who haven’t any training in the philosophies of these cultural scientists and medical leaders.
In a recent review of epilepsy cases and their care practices performed in large urban settings, I found that there was a growing number of Middle Eastern parents with children adding to the health care system due to their greater numbers of visits to the provider for children, about their concern that the child might have epilepsy.
By reclassifying the religions noted in their EMR data, I was able to merge the data enough produce classes of religion that could then be used to five major religious groups to each other, and then to several smaller religious or religious-like belief systems that are increasingly popular, and can impact the way patients chose to seek out medical care or not. The final group I defined was the “Unknown” group, patient who had no religious affiliation listed.
Inoculation discovered – Al Rhazes
Findings
A review of ten groups in terms of the numbers of kids with parents concerned about epilepsy, with the epilepsy ICD in their electronic medical records database, showed that mostly the Middle Eastern families were highly concerned for their child’s welfare when it comes to diagnosing and treating epilepsy for a child who is under the age of 4. They are the only group demonstrating early peaking in visits for this ICD for the one and two year old children, demonstrating aggregate visit rates that more than twice those of any other religious class in the U.S. The summation of these visits for kids by the time the child reached eight years of age, was much greater than the other classes, in particular at the visits and procedures levels. This means that not only were the patients evaluated for possible epilepsy higher in Middle Eastern groups, but also underwent considerable more visits to determine their diagnostic state and many more procedures to confirm the final findings or claims made about a diagnosis.
Equally important to note for this study is that the peak age for children seeking out help or assistance about a possible epilepsy condition is closer to the 8 to 12 year range than the 0-5 year range, like it is with Middle Eastern families. This implies that the non-Middle Eastern families have a wait and see attitude that prevents them from seeking out possible insight into their child’s state, assuming that child even experienced an event that would make the parents be so concerned about epilepsy.
Commentary
The needs for childcare visits for epilepsy for children so young in Middle Eastern families suggests there is a culturally attached belief system feeding into this watching and waiting attitude, avoiding it as much as possible. This could be because the Middle Eastern concerns and judgments about a person who is diagnosed with epilepsy have a much greater impact on that person’s life and the life of his or her family.
One final observation about this Middle Eastern behavior related to seizure related visits and procedures involving very young children is the gender asymmetry of this pattern, with boys receiving this care more than girls. In other cultures, the two genders have equal representation for the most part, with boys sometimes slightly more than girls in early childhood, but with female related visits and procedures performed far outnumbering male visits and procedures for most of the decades to come.
This difference in patients, visits and procedures data for epilepsy related visits, by these ten groups I defined and evaluated for approximately thousands of cases, suggests that this topic is in need of a much more detailed analysis. As the numbers of Middle Eastern patients increase in the years to come, we will most likely see the influences of Unani-Tibbs medicine and philosophy come into play in highly multicultural healthcare settings, in particular the managed care programs.
If the institutions in charge of some managed care system aren’t ready for this change, this could result in less communication between patient and provider in the traditional allopathic healthcare system. We don’t want to see the influx of new cultures lead to the development of another set of new healthcare providers in the United States, not effectively monitored, because the current allopathic system is unable to make the accommodations necessary for this new way f dealing with and interpreting medical history at home, in the doctor’s office, and in the in-patient setting.
From my Pinterest slides on this topic
Recommended Searches to review:
https://www.google.com/search?num=20&espv=2&q=unani+altonen&oq=unani+altonen
https://www.google.com/search?num=20&espv=2&biw=1580&bih=840&q=islamic+epilepsy
https://www.pinterest.com/altonenb/international-health/
May 14, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on What to make of the Spikes in Followers
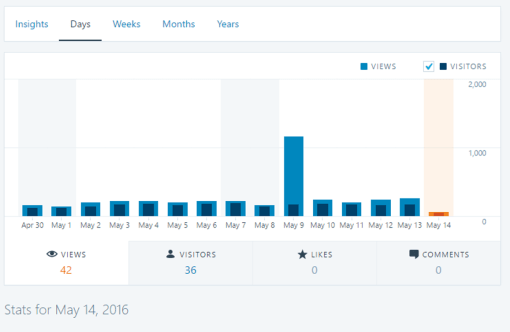
About twice a year I get these huge spikes in people visiting my site.
What does it mean?
The first time this happened, I had about 3000 hits in 24 hours. Totally unexpected, it led me to contract the company that provides the place where my site and information are housed. Their response . . . . normal traffic, due likely to a recommendation to visit my site by a place with regular visitors or a list of subscribers.
At times, there is no telling why these people visit. If I am lucky, I can link the surge in visitors to a single page and topic. One day, a few years ago, I was able to find a web page indicating that a conference was being held at the moment, and my site was possibly referred to as an example of what is out there. The topic . . . medical GIS.
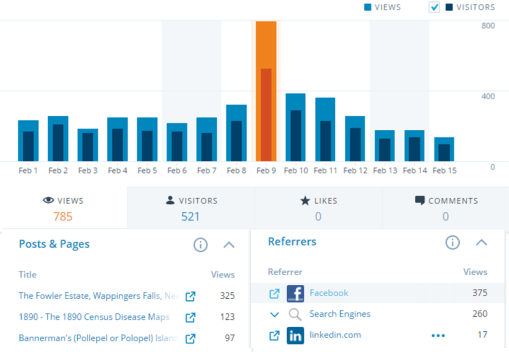
Several times I have been able to link the masses of visitors to a specific topic or course related to medical GIS. My hexagonal grid mapping is the most common page frequented now by medical GIS students. Interestingly, it also suggest that professors and practitioners in the field of medical GIS have yet to adopt this new methodology.
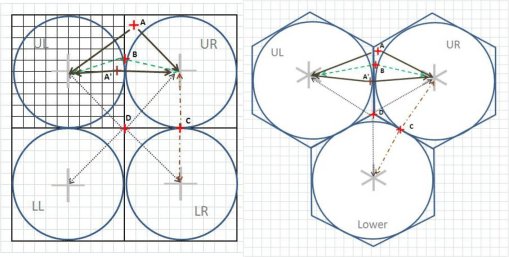
My illustration for the math behind hexagonal grid mapping.
There are some things that the health profession cannot do. They cannot treat everyone perfectly. They cannot prevent the most basic iatrogenic illnesses and surgical mistakes from happening. The evolution of new disease and illness, due to the clinical setting, are natural events–the profession’s decision to focus on just the insured at the risk of ignoring the uninsured is the reason we are having immunizable disease outbreaks. relying upon false assumptions and grandiose conclusion drawn about the success of your 98% effective immunization program, is like turning your back to the plank fence blocking your view of all those poorer communities you have missed.
The recent resurgence in in-migrating vectored diseases is an indication that public health and the world health were taken by surprise by the ability of old diseases to travel to new places. Why the errors?
Understaffing at the WHO level, and those whom were employed weren’t experts at all compared to some of the leaders in this field, and the questionable ability of United States, CDC, and even NIH leaders to even successfully managed its small pox labs and anti-terrorism teams. We do not know if AIDS was ever borne due to corporate lack of control, but we do know that Anthrax made its way into the public setting due to poor management and leadership, or that old vials of forgotten test samples of small pox could be found, where they were never supposed to be stored these past 50 to 60 years.
Fortunately, what few open minds that there are for new discoveries, are mostly found in the student populations of public health programs.
In just a few months, any system can design a means to managed its population using just five basic query paths for its EMR. This means that while systems struggle to make their EMR systems perform and function at the clinical level, quality improvement teams working on their own at the corporate or institutional level can produce a system that makes more effective use of their data at one or two thousand times the other teams’ productivity level.
Meaningful use has some meaning. But it tells us little about the prevalence of genetic diseases, the amounts of illegal care practices being performed such as childhood female circumcision, the amount of spousal abuse engaged in by specific religious groups, the amounts of poor nutrition and malnutrition related conditions suffered by low income communities, the amounts of MVAs experienced by kids riding ATVs, the numbers of people who refuse to have their kids immunized and locations of their clusters, the age at which boys are least likely to see a doctor, the kinds of developmental disorders that are surging in certain ethnic groups.
We can brag about about MU attempts and the results of a few of those 40 or 50 measures we’re focused upon. Yet throughout all the hours spent trying to get a perfect outcomes and report generated, we miss nearly 99% of the population still in need of the same type of care and managed care improvement processes.
This latter reason is the primary reason Medical GIS has to be implemented as a core part of all managed care programs. But as the evidence shows regarding those that visits my pages devoted to Medical GIS, such a change is perhaps another generation or two away from happening. Leadership, management, directors and VPs are still struggling, trying to make progress about a subject that should have been resolved nearly a decade ago, when medical GIS was ready to become a standard.
May 8, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on religion and health
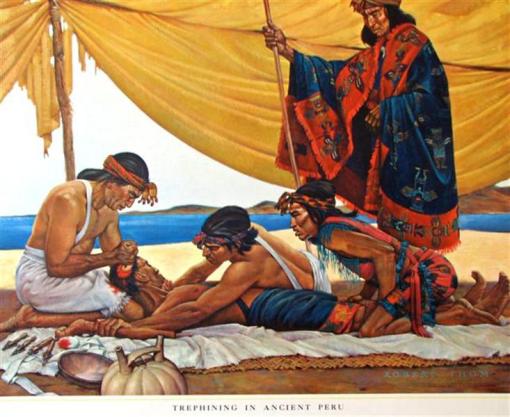
“letting out the bad spirit” caused by a head wound with an adz while in battle
From a teaching collection. See http://www.trowbridgegallery.com.au/john-gould/trephining-in-ancient-peru
I finally reached the point where I have been able to analyze religious philosophy and relate it to health and medicine practices. Religion is not a single philosophy or even a set of philosophies of similar form and content.
Religions vary because their philosophies are different. But just because two religions are distinct from each other doesn’t mean the way they look at health is different from each other. Alternatively, when two religions are in the same major belief system, using the same books or sacred writings, basing their philosophies on the same mystics, saints and writers who produced these books, this also doesn’t mean they think identically.
Religions have a topology or distinction from each other, and the ability to merge together to form similar groups with seemingly quite different theological ideologies, because certain features of their philosophy and discipline relate them to each other. Fundamentalists in the major religious sects of the work, for the most part, belief in some of the same things as each other, enough to lead them to have similar experiences about being ill, and about how that illness can be made to dissipate or go away.
Similar, people who are completely devoted to the science of health, in either the physical and or behavioral science way, believe in theories that are used to describe how the health of a patient comes to be. There are certainly differences between the purely physical science idealist, and the behavioral science only idealist (you are or become what you think).
With regard to religion, if you don’t belief in religion, but believe in something akin to some of the beliefs of religion, such as this higher power, your “religion” is what I have termed natural theological. You belief is some higher power, but not so far out on the edges that it isn’t religion at all that your are thinking. Two prime examples: Quakerism and Shakerism.
To some writers of religious philosophy, out pragmatism makes us become who and what we need to become, and many of our thought processes relate to this process of behavior and personal development. We become whom and what we are for a reason. That belief is very much akin to religion, with the exception that we place the total responsibility for who and what we are on ourselves first, and nature second, and the effects that nature has on us, either as some truly scientific form of nature, or as a nature with this possible “force” that we must learn to control to help define and determine out own long term fate. This kind of religion I call “natural theology” because the “universal concept” it depends upon is that universal power, energy, being, or field of change and existence.
The universal energy belief that is attached to certain religions is a simple, less anthropomorphic version of the extracorporeal God concept. For example, the “God within” that we allow to exist, we decide to accept as being potentially useful, and usually approachable, with the hopes of gathering it enough to produce a consequence. The individual who believes in the Godlike power of prayer, universal energy, waving the cross over the head of a “possessed child”, but without abiding by a traditional global religion based version of this philosophy, is one of those universalists who pay heed to universal power, which in turn is interpreted as the “universal god”.
There is also a slightly less universal-minded philosophy that approaches more the physical science, neurochemical interpretation of the mind, and God as a state of that mind. This religious group, although we hear about it quite a bit, doesn’t seem to pop up in the medical records as much as a new researcher of religion in the local community appears to exist. Only the big groups tend to show up in the medical records it seems. Patients are still quiet about their universal energy ideology borne by the religion of Scientology or Christian Science. We know they exist, but may not be indicated as such in the medical documents. A modern term for these beliefs, and their reliance on “logic” is philosophical realism. Belief is everything, no matter how many parts the brain has and how they are divided from each other.
Religion is also defined by culture, and culture in turn is defined by countries or nations, and nations and countries often have relationships to the majority of people within that nation. So a nationally-definable single religion does not exist, but certain religions do seem to relate to specific cultures, and those cultures in turn to specific countries.
Even though a single religion in related countries is not universally the same across all those countries, there are some culturally defined life patterns and personal, family and community behaviors that define the roles that a particular religion may play in producing, supporting or helping an individual’s health. Asian cultures are quite different from each other, and the religions harbored by certain parts of the world vastly different from each other in when they were born, who their founders were, how they interpret disease and discuss it via the religion writings, and how they react to disease, feed the child, treat the very sick, tend to the very poor and needy. Buddhism, Hinduism and Bahai faiths are very different. Yet their attentiveness to self, relatives, family, neighbors, community, foodways, beverage consumption, cooking practices, sleeping and prayer techniques, hope and prayer for the ill, are very similar in how they impact the ill person, because the families tend to display the same human reaction to poor health, in spite of their religious and cultural upbringing differences. What brings them together into a single group is my observation that these followers often place more trust in the self and the philosophy this other culture is teaching them. With the exception of one Caribbean group, the bulk of these beliefs systems are Asian or Asian derivatives. The reason to group them together pertains mostly to the faith that they hold in their traditional beliefs, not primarily the teachings and philosophy of Western medicine.
So, beginning with approximately 160 religious types, after a few days of thinking and analysis, mostly reflecting back upon the years of readings I engaged in about religious philosophy and the meaning of disease, I developed three classification systems for religion, and in the end, for now, allow the following to be used and evaluated in relation to how disease, state of illness, religious behaviors, personal religious philosophy and community or family belief practices, play into the health and well being of each individual, at the preventive health level as well as with the recovery process and exceptional cure (“Miracle”) process of recovery.
For now, the following ten religions are used to analyze the interplay of health, religion and culture/ethnicity or race on how patients survive and experience their diagnoses.
- Catholicism
- Christianity
- Christian Sects
- Judaic or Jewish
- Islamic or Muslim
- Natural Theological
- Cultural (the Chi, the higher power)
- Contemporary Spiritualists (higher power is scientific; i.e. Xian Sci, Scientology)
- Modern and Postmodern (atheists, agnostics)
- The undefined (no answer given)
In the next few months I hope to see relationships between certain disease and health states, and the entry within medical records that defines your personal ideology or philosophy.
May 6, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on About to pass the 350,000 Mark
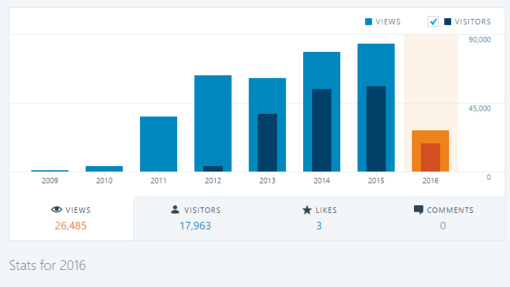
As of today, 17,963 visitors have come to this site since January 1st, 2016, visiting 26,485 pages, resulting in an average of about 1.5 pages per visitor in 2016. That additional page, is usually a new visitor visiting my home page to learn more about the producer of this blog site.
This site is slowly approaching the 100,000 hits per year mark. It will probably come close, but not pass this number by the end of 2016.
But by tomorrow morning, I am pretty certain I will have passed the 350,000 hits mark, being visited by about 2/3 x 350,000 times, about 117,000 people, essentially over the past 5.5 years.
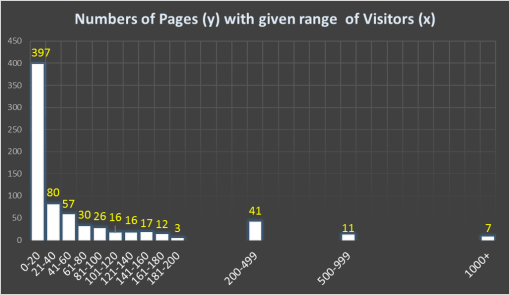
There are currently 713 pages on this site, and another several dozen sitting until that are either completed but on hold, or being held until security privileges are lifted for other researchers accessing the data they hold.
My number one pages for all the time since their first posting are as follows:

The Census Disease Maps page, which tops this list, is a fairly recent addition relative to the rest. This tells us just how hot a topic like mapping population health has become.
If we combine the two pages devoted to hexagonal grid analysis–one which is informative, the other for downloading the excel file to produce you data with for learning this precious GIS skill–then hexagonal grids is my second hottest topic for this site. For the time being, I am given unofficial credit for having worked with, tested, analyzed, and successfully applied this innovative way of mapping data. Its most important attribute–it reduces spatial error by about 26% when used instead of the square grid method still heavily promoted.
No other spatial mathematician has produced and circulated this important spatial method, since I first posted this methodology several years ago. (For background information, I invented this method/the math in winter of 2003/4, while looking for GIS work, which I didn’t find, and used it successfully to map chemical exposure in the state of Oregon, and develop much smoother contour maps and 3D surface models of this exposure history using a combined grid-raster GIS-Remote Sensing analytic system.)
For a while, “Cattle Drives . . . ” was very much my hottest page after these first ones. “Small Pox and Cree” and “Four Prussian Diseases” remain at the top since they were first posted, four or five years ago.
My Thesis on historical medical geography has climbed up several levels recently, suggesting to me the growing interest in the history of medical geography, not just spatial epidemiology.
In general, the history of medical geography is the singlemost important part of this rapidly growing field. As a graduate student in the field, I found it interesting but not surprising that scholars were reinventing the wheel in the field of spatial health and medical geography. My dozens of pages on the historical examples of disease mapping during the 19th century, and the most important, “first time” writings of a number of theories, recently re-invented by epidemiologists, are provided for researchers to review the true history of discoveries made in this field.
In fact, the medical sciences and recent natural sciences scholars in spatial epidemiology and medical geography/GIS have tried claiming they made discoveries that were around as far back 150 years. This can be blamed on the prejudice this country and culture had against “learning geography” since the 1960s. During the 1970s and 1980s, we were all hard scientists, strongly against the idea that sociological and cultural studies were really of much importance to United States academia, science research, health and medicine. The schism between hard science and the social sciences that developed because of this ideology drove medical geography concepts into the backs of journals and books, and onto shelves in the library rarely visited by scientists, just the few geography students in academia.
With interests in spatial medicine now around for good, and the need to explore this other route to understanding people and health on the rise, medical geography is an essential way to learn sociology and medicine. It may seem post-modernist to focus so much on neodarwinian people concepts, to want to understand how society and people spatially present themselves to researchers trying to understand disease and health behaviors, but this post-modern approach is important not only because it is new and “out of the box”, but also because it better explains some phenomena better than old fashioned science has done.
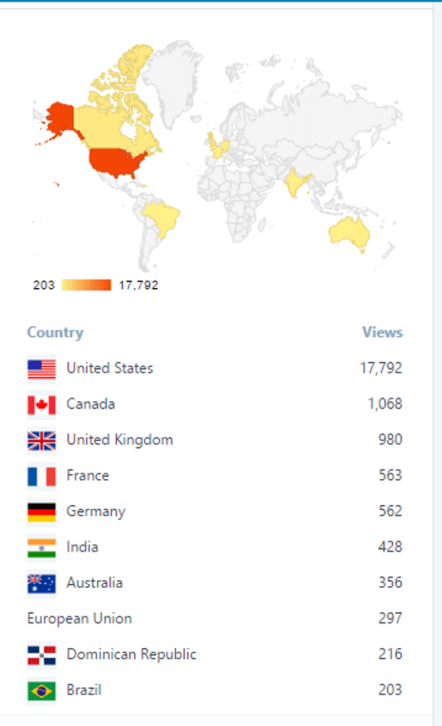
The 2016 views listing shows the US is the first visitor to my site, followed by Canada. Canada in turn is followed by the matron culture of its philosophy and theory — the UK. Both Canada and the UK are ahead of the US as social geographers and social medical geographers; the US is and has often been tied with or slightly ahead of the UK with the scientific aspects of medicine. But these rankings are hard to prove at 100%; there is a major ethnocentricity born within our judgments of where the most important scholars resided in history. The UK, and by default Canada, have the originators of many of the social aspects of geography and some of the best methods for more completely analyzing medical geography data. Statistics and epidemiology were probably born and promoted by England, and many an British scholar came up with important new uses for mapping and health. But remember, many of these techniques weren’t invented by the U.K., just made better and propogated further, and perhaps because they translated these methods into English, made it possible for followers to attempt same applications of their skills.
My review of medical geography history shows that the Prussian, Germanic cultures were in some ways ahead of the British with mapping concepts. But until their findings and discoveries could be translated into books published in the English language, those lessons were not going to impact enough substantial scholars. For this reason, a lot of traditional medical geography works are still unpublished, undiscovered, were it not for the attempts at this site to find them and bring them back into the global knowledge bank (i.e. Schnurrer’s first map of disease, 1827).
US disease cartographers of the early 1800s were some of the most important discoverers of medical geography techniques. Samuel Mitchell is my primary example. He is one notch better than Benjamin Rush, and singlehanded made “Medical Geography” a publishable medical term. Early US cartographers like Mitchell made discoveries that were often dropped, remaining unused until their rediscovery by geographers and mathematicians in this field after the late 1960s.
For a number of reasons, determinism is why geography was dropped by most academicians and medical scholars. Coupled with pro-socialist and pro-Marxist ideology, this particular behavior of geographers made them an unwanted group at many of the annual science meetings. More than thirty years ago, as a science major in two fields of science, I myself felt this breed of scholars was very much into its own paradigm, its own ideology with its own philosophical underpinnings. Now, decades later, I appreciate these older teachings, because they explain some things better than scientific thought and reasoning can do.
There are a number of philosophies or interpretations of disease and geography, founded and first published in the early 1800s, that have direct applications to today.s spatial analyst processes. And this is the reason one third of my site is devoted to the history of medicine and medical geography. One has to understand and read about the philosophy to then better apply it to the modern world.
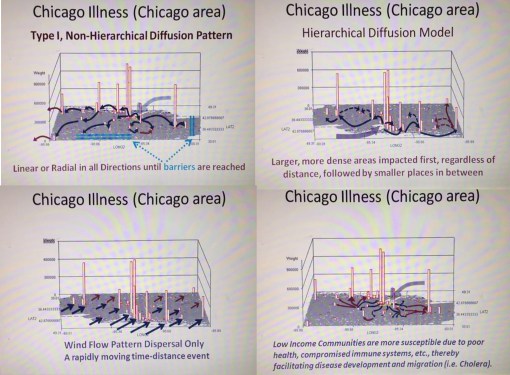
Two examples of Sequent Occupancy
Let’s accept the fact that epidemiological transition is not as good a model as Sequent occupancy modelling of disease patterns is for the United States, at least when it comes to the details of the new public health issues.
The hierarchical diffusion theory, published in the late 1890s by US Geographers, was first penned in the late 18th century by Benjamin Rush, although mostly in theory and riddled with political opinions and prejudice. But its version stated by a NY physician upon observing cholera strike the US for this first time, enabled hierarchical diffusion ideology to be trained at the US medical schools and be published as an aside in the medical journals and many theses then published on this topic.
Medical geographers are, or can be, ahead of the masses in medical science. Science alone cannot describe some of the things we now can document in this new information technology dependent world.
I can guarantee you, that if you read through all of my pages and learn the philosophy presented on the history of medical geography and disease cartography, that you will be several steps of others in this field, including many of its passing leaders.
If you want to be ahead, be like Valentine Seaman: observe, learn, test and discover, and then apply it by trying something new.

May 3, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on The Gate Theory & “Herd Effects”
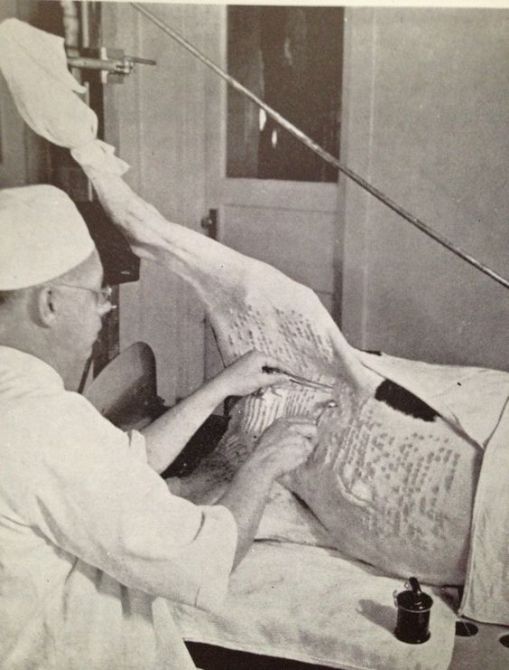
Figure: From my old Pharmacognosy text by Evans, ca. 1940s. The first vaccine ever developed used “kine pox” (the serum extracted or scraped away from a cow with pox infection in the skin.) This process for manufacturing vaccines for the Pox maintained the use of the cow into the mid 20th century. This is how the pox was extracted from cattle during the 1940s. Whether the cow in this picture was bred to be “hairless” (reduced hair) or is just very cleanly shaven is uncertain.
Reading the news story about the Harvard Mumps outbreak in the dorm–there is really just one line you have to walk away remembering from this story:
[Quote] ” . . . people in college dorms often share living spaces with dozens of people, giving them more opportunities to be exposed to the virus, either on surfaces or through contact with other people, Adalja said. Although being vaccinated against mumps can prevent a person from getting sick if he or she has been exposed to lower levels of the virus, for people living in dorms, vaccination may not be enough to ward off an infection, he said.
“The exposure that they have to mumps is so high in these situations that it overcomes the ability of the vaccine to protect them,” Adalja told Live Science. “It may be that, in these special situations, a much higher level of antibodies [against mumps] is needed to keep the virus at bay,” Adalja said.”
[END QUOTE]
Wait a minute . . . wasn’t being vaccinated supposed to have a “herd effect”? This would mean that if all the college students in the dorms are vaccinated, we needn’t worry.
See http://www.foxnews.com/health/2016/05/02/mumps-outbreak-at-harvard-why-do-vaccinated-people-get-sick.html

OLYMPUS DIGITAL CAMERA
A portrait of a past mentor of mine, Dr. Daniel Fox. An MD at SUNY Stony Brook and expert Medical Historian, he was a major influence on much of my work. He removed from SUSB around 1989 for a Chief Editor position with the Milbank Quarterly, a medical journal devoted to the federal programs that define the healthcare system and provide rules and regulations in the establishment of the current managed care system, the development of HMOs, and the establishment of many of the Federal programs devoted to health, such as Medicare and Medicaid.
The “HERD EFFECT” provides a very false sense of security to people in medicine, in particular those who contest my past three years of reminding people that 1) theories are perceptions, not facts or truths, 2) theories are good some of the time, not all of the time, and area based on the culture of the places they are born, where the definitive observations are made, and 3) theories in medicine are, in many cases, just as good now as they were back then (remember the lancet?).
The purpose of theory is guide us into understanding a phenomenon we are observing. A person into innovation and change works with multiple theories, multiple options, multiple routes to take in the analysis. A genius is a skeptic of theories, because all theories require skeptics. In medicine, it was the skeptics who decided the theory of four humours was off, or that the alkaline theory of blood and disease so common around 1790, did take into account the chemistry of the blood, but made some false conclusions.
We should be thankful that theory got replaced, right? It was replaced by the nervous energy based theory of the body, which enables scientists to argue sensibly about how life was an process totally derived from natural energy, and the “medical electricity” was the panacea of the future. And in a few years it was the future, people changed their minds about older ideologies in medicine, decided the old time teachings were out of date, and that the theory of disease and how to cure it had to somehow be replaced by more welcoming philosophies.
The discovery of the vaccination using kine pox serum, and the nearly synchronous discovery of the magical powers of homeopathy is not coincidentally proven around the same time as vaccines for any different reasons. The two were derived from the same theory, and took different paths in the philosophical synthesis and use in medicine. Franz Anton Mesmer would be steadily arguing with Volta and Hahnemann, each contesting the other “experts'” claims, not realizing in a decade too, they too would not longer completely correct, that their ideology would have to be changed to be practiced, again and again and again, until doctors finally got it right.
Allopathy’s gate theory of pain still remains a basic idea that we are taught in introductory nervous system courses. The herd effect is taught as a lesson and a rule, but it should be hypothesis, less in value than a theory, and in today’s classes used as a reminder of a theory that this ideology or philosophy medicine relied so heavily upon is failing. It is not a theory any more, and to mention it as your guiding lines of reasoning in the discussion of the failure of infectious disease vaccination programs, enables those who see failure happening to point to you as the cause–you and your old, out of date theory.
Medicine is no longer like it used to be when the philosophy of “Herd Effect” was born. We are more observant, and needs to use the imagination less to know when the events that ensue and the theory that supposed explains them, are a mismatch.
The above statement – – – “The exposure that they have to mumps is so high in these situations that it overcomes the ability of the vaccine to protect them,” – – – is an excuse for a failed theory. It demonstrates lack of acceptance of being wrong. Physicians and medicine are not humble. They hate to admit they are wrong when they are. But in the end, such a stubbornness only embarasses the profession further.
The younger generations, going to college as premeds, are either with you or against you in allopathy when your theory fails to hold its ground once changes happen. Patients, students, shouldn’t be assumed to be part of some great Pavlovian experiment that medicine is engaged in, mesmerizing you until you either given up and accept what is claimed, or are somehow tricked into believing that the gold leaflet they wrote this “Truth’ upon has to be correct, because of who wrote it, not the work and evidence developed to prove it is still true.
It is very easy to eliminate this problem. Open the gate and let the new theories in.




