January 2015
Monthly Archive
January 31, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Has Culture Defined A Hudson Valley Measles Nidus ?
State Health Department: Measles Vaccination Remains Vital to Protecting Against Highly Contagious Disease ALBANY, N.Y. (September 21, 2012) – In light of confirmation of a measles case in a school…
Source: rhinebeck.wordpress.com
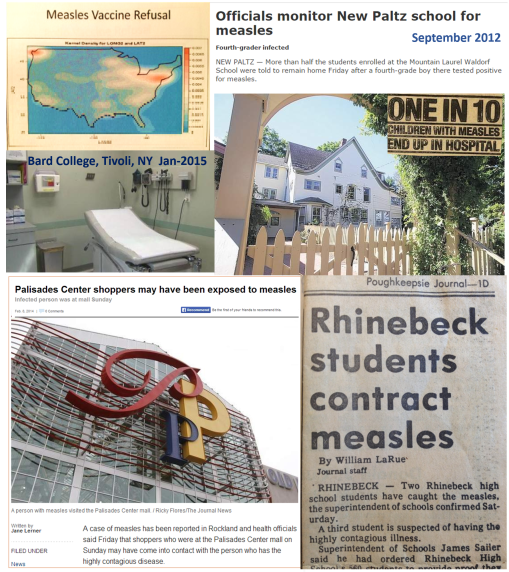
"Nidus" is a mid 19th century term used by medical geographers used to describe what we today might call potential hot spots for disease. A nidus is the "nest", where the first cases develop and from there spread to other locations either radially or along specific kinds of routes such as along a waterway, through a valley, by following a particular assemblage of plants and animals. Medical geographers in the mid-19th century had perfected this way of understanding disease development, to such an extent that they could use such unusual physiographic features as aspect of a hillside and the slope of that location to define where the disease might fester, due to the "animalcules" or microbes that lives there naturally. (Unlike what common teachings like to profess, bacteria was the first small organism we related to diseases.)
Since the 1980s, there have been at least four outbreaks of measles in the valley, and they share certain common population, travel, and business or economics features. And they represent a classic example of the hierarchical diffusion process (see my page on this – http://wp.me/Puh6r-5TT ).
Three of the articles and discussions of these four cases have one town or village as a common source for the cases. The case that emerged just a day or so ago is somewhat to the north, associated with the local railways system returning a student to his/her college setting. The case from two or three years aback also involved schools in some way and local international travel–in that case it was the school that allowed 50% of its students to not be vaccinate, per their personal belief or faith. The association of the Rhinebeck-Bard-Tivoli cases with those in New Paltz across the river also shared university-international travel or foreign students features.
The fourth location to the south is where the first recent mention of this problem returned to the local newspapers, down by the Palisade Mall in lower New York.
See also See also: http://www.skepticalraptor.com/skepticalraptorblog.php/measles-case-confirmed-york-state-school/
Now, it is easy and at times too easy to draw these comparisons between regions and see similarities. Culture itself for example is not the cause for this part of the valley showing a tendency to be a nidus. Statistically, I might call it a covariate. The main factor in this migration of measles into the eastern U.S. is the population health behavior features, and the fact that the Hudson valley has a unique behavioral feature–programs that bring together many people who demonstrate a strong support of personal beliefs, personal rights to chose, and "alternative forms of medical beliefs or thinking."
We all have the right to be "different". If only we knew how our differences influence the right of others to live a secure life, without fear of that terrible Scarlet letter coming close to our kids, elders, or family members engaged in critical quality of life related health care. In this case, cultural diversity works against the continued survival of these different communities. There are some rules that must be followed by all cultures, no matter what sacrifice of personal rights may be required.
We map physical and human geography all of the time when we research spatial epidemiology. Small scale area analyses may be used to define specific natural ecosystems or niduses required for west nile to develop in this region (I posted my example of successfully using this technique in 2002 and 2003, a while back). We can also use small area analyses to identify niches of unhealthy communities or shared communal settings.
One has to wonder, how much of this type of cultural analysis of disease (if any) is engaged in locally?
In the past few days, a comparable social behavioral pattern has emerged recently in Minnesota as well (http://www.startribune.com/lifestyle/health/290151131.html ).
See on Scoop.it – Medical GIS Guide
January 30, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on 5-Year-Old Girl Dies After Catching the Flu, Even After Getting Vaccine

Kiera Driscoll, 5, had a slight fever on Sunday morning, but she seemed to be feeling better after taking some children’s ibuprofen, said her father, Patrick Driscoll. “In fact, she was playing outside that afternoon with my wife and even made a comment that it was ‘the most fun time ever,'” Driscoll said. But then Kiera’s slight fever returned and her cough worsened and included phlegm, Driscoll said. She didn’t have asthma but occasionally had a barking cough as a baby, Driscoll said.
Source: gma.yahoo.com
There are seven ways debaters can go with this news story. The writer of this story and editor of its source took direction #7 — the worst approach. It will be interesting to see how many ways that those with ulterior motives go with this sad story.
My first impression, however, is, based on the ill-conceived, misdirecting title, that this tale is going to add fuel to the fire already out there about vaccinations, namely linked the events linked to the recent measles outbreaks on both the east and west coasts over the past year.
But these measles outbreaks and the issues they relate to are not related to why this girl died. She died because she caught the flu, but the flu alone did not give her cardiac arrest and take her life. One could argue that if she had the shot . . . . (I don’t know really if she did or didn’t.) One could also argue that even if she did, it doesn’t matter, since the flu shot available this year doesn’t match the strain that is going around this year.
Still these reasons have nothing to do with this her death.
I next read that she was put on ibuprofen, which reminded me of my freshman years in pharmacology and medicine when myself and others felt the aromatic ring added added to salicylic acid was "bad for you", and toxic to the liver, and reduces the purported effect that salicylates have upon EPA, PC and PG pathways it was felt to work with, unlike tylenol. All of those "truths" about what makes these common OTCs work and so different from each other are now dead and gone. Guess I didn’t learn only the facts back then after paying my medical school tuition.
Ibuprofen couldn’t cause the mucus plug that blocked her airway passage, nor did the flu. It was the asthma medicines that caused these mucus plugs. This is a classical lesson about the use of asthma medicines in emergent care, that all of us have to learn and relearn as clinicians and as patients (or parents of), lest we forget it at the worst of times.
Up until the 70s, you could by the daturine and analogs needed to "treat" asthma. I say "treat" in quotes because that’s not really what you are doing. The Acetylcholinesterase Inhibitors [AChE-Inh’s) like daturine, hyoscyamine, belladonine, scopolamine, atropine, and the like, work by drying air passages, making the mucus thicker, unable to to be expectorated. This was the primary reason we stopped the distribution of products like Asthmador and the like in the 70s.
Today’s complementary-alternative medical [CAM] field has practitioners who still support this very old line of therapy. So this story brings us in circles–CAM is also strongly linked to the anti-immunization movement that is now happening. Could CAM be the reason for her death? Unlikely. (I hope).
CAM isn’t responsible for this asthma drug related tragic death, nor is the asthma drug probably (unless it’s an overprescribed 100% AchE-Inh against HEDIS/NCQA/FDA/APhA recommendations), nor the flu shot, nor the use of OTC ibuprofen, nor the flu, nor her history of a flu shot.
But I am providing this background about the probably cause, forensically, due to the Title of this article. It is misleading, and very much showboating.
Kiera Driscoll did not die after catching the Flu, or after getting her Vaccine. She died due to her need for asthma medications, the administration of the wrong type, and the lack of emergent care received on time. The flu was a co-morbidity, and initiator, but not the cause. The Vaccine had nothing to do with this event. Still, due to Pop Culture, the editor and author wish to follow their ulterior-motive/personal ambitions with their title, pointing their fingers in all the wrong directions.
This is biased reporting, if ever I wished to see a perfect example of such. That makes it a lesson for the day in public health.
See on Scoop.it – Episurveillance
January 28, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on A History of [Un]Immunized Diseases
Review of the history of Vaccination and Inoculation, and the diseases that have been reduced due to the immunization program. An epidemiological transition a…
Source: www.slideshare.net
I have also posted this in video (minus audio) form at : https://www.youtube.com/watch?v=LOp-KGd4hV0
I produced a lengthy review of this vaccinated diseases topic that has evolved in recent weeks. I have been watching the anti-immunization movement grow for quite a few years, and decided it was time to publish my rendering of what this movement could do to the history of medicine and how these diseases can impact the lives of kids who don’t get vaccinated. This version lacks an incidence-prevalence statistics review, but covers the history of inoculation/vaccination in detail, going back to the 1770s. A few recent postings show the graphs I was developing for this, with the results of my temporal analysis of the immunization programs and immunizable diseases. I avoided several “hot topics” for now, but will re-review them and add them in at a later time. The major point here is to provide a detailed visual presentation of what the diseases look like within the clinical setting. People seem pretty much decided upon this matter for the time being. So I may be preaching to the choir with this posting.
See on Scoop.it – Episurveillance
January 27, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Melinda Gates has the perfect response to the anti-vaccine movement
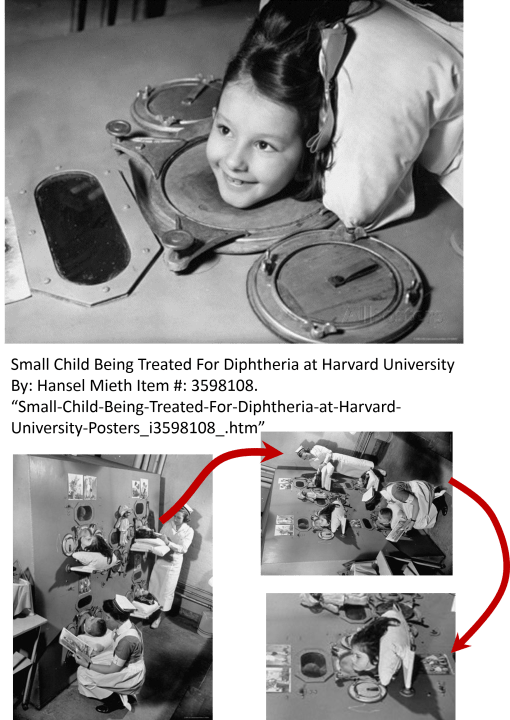
Melinda Gates: “Americans have “forgotten what measles deaths look like.”
Melinda Gates was very much right about how much too many of us have forgotten. This set of pictures I have on display here say it all. As pop culture historians interested only in today, as we personally see it, we remember the least, but retell the past as if we were “experts”.
Source: www.vox.com
Ahh, the mistakes we make!!!!
See on Scoop.it – Episurveillance
January 17, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Historical Medical GIS – Eight 1890 Census Mapping Examples
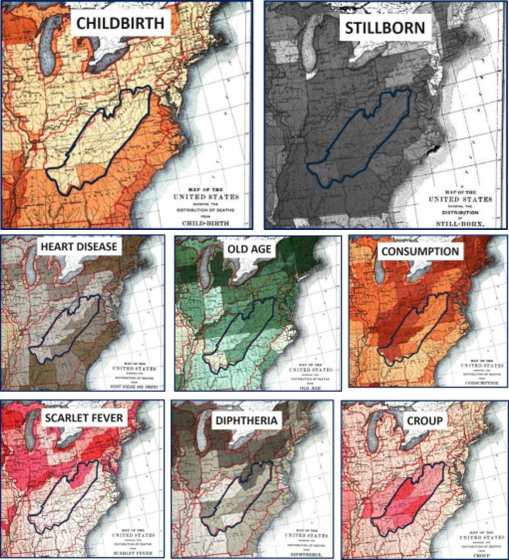
The disease maps in the 1890 Census provide us with some of the best insights into American medical history just after the bacteria was discovered. Disease mapping was about to experience a major change in significance, as scientists began to focus on the microbe, something you did not easily map. We started to focus a lot on population health, due to the development of the sanitary theories for disease popular from the 1870s onward. This is from a page I posted on the 1890 Census Disease maps, a part of which is focused on the health of Appalachia, where some of the poorest parts of the United States still exist today.
These maps can actually tell us a lot, if we take a moment and think about the US population during this time.
Westward Expansion was well underway.
One direction the US population flowed was directly westward, across the northern edge of Appalachia, through western NY into Ohio and from there over the Illinois and then south the Missouri. We can see the impacts of these populations on diseases or conditions related to population density and increased likelihood for survival. for example the map of "Old Age."
The US population also continued to follow the eastern ocean shores, forming many large cities, but still decades way from establishing a megalopolis. Heart disease hugs the short of part of the Atlantic for this reason. The were some of the most developed parts of the US at the time as well, and demonstrated the impacts of less poverty than the rural mountain regions heading through the Appalachians. Does this mean the northern New England region and Southern Diets weren’t at all good for the heart?
Consumption is a western slope disease. Originally noted to be most prevalent in the NY-New England sector, it managed to head deep into the interior but seemed to like a specific environmental setting. There are two unique strips of this disease, one along the mid-Atlantic oceanic-bays states regions, the other on the western edge of mountain, eastern end of the Great Plains.
Scarlet Fever is very much a population-bound disease, following the migration roads, shipping routes and adjacent railways laid through central Pennsylvania along the Ohio River, staying at the south edge of Ohio, Indiana and then heading back north towards Chicago and the Great Lakes.
Croup wasn’t picky about what side of the mountains it was on. It was just searching for susceptible kids.
Diphtheria for some reason has a more northern tendency. Part of it traverses Pennsylvania, another part follows what seems to be a latitudinally define path, heading north of the mid-latitude line of Ohio, then over the Northern Michigan and Northern Chicago into Wisconsin.
Childbirth is a product of populations and people. The Southern coastal state rates were higher than the northern There are also two very distinct sections of the southern Atlantic states with higher numbers. For obvious reasons, more people are seen living along the coastal regions, so more babies are born there as well. Higher birthrates are on the eastern shore of the Mississippi River in Illinois, not the more rural western shore with larger farms in farmland communities. The shores of the Great Lakes bear more children (shipping towns). From New England to Ohio and lower Illinois, birth rates remain lower than the same longitude down south, along the Gulf of Mexico.
Finally, stillborns were a happening that occurred nearly everywhere. This ubiquitous nature of stillborns in the late 1800s is very different from what I expected for midwest farming communities, the medical school books of which are filled with cases and chapters on teratopathy and birth defects.
See on Scoop.it – Medical GIS Guide
January 15, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Washington state teen who was shaken as a baby dies; father likely to be charged
By Victoria Cavaliere SEATTLE (Reuters) – A Washington state teenager who suffered life-long injuries when she was violently shaken as an infant has died, and a Seattle-area prosecutor said on Wednesday he would likely charge her biological father in her death. Baylee Duggins, 15, of Tacoma, died on Sunday from respiratory failure linked to pneumonia, according to her mother and the Pierce County Medical Examiner’s Office. Duggins’ biological father, Christopher Schwanz, was convicted in 2000 of second-degree child abuse for shaking the girl as an infant, leaving her severely physically and mentally impaired, according to Pierce County court records. Pierce County Prosecuting Attorney Mark Lindquist said he expects to bring a second-degree murder charge against Schwanz pending a review of the medical examiner’s evidence.
Source: news.yahoo.com
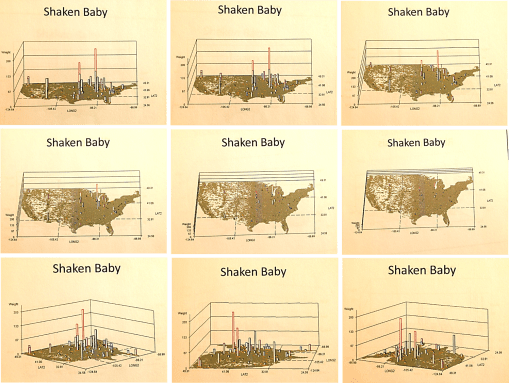
The answer to this growing problem? Perhaps it’s all in the mapping.
My video on the national distribution of this public health problem –
https://www.youtube.com/watch?v=Y3c4A-oagjg
(other child related public health issues are included as well on this page).
Shaken baby.
Teenage/childhood suicides.
Bullying.
These are the three most important socially and culturally related public health issues for 2015.
Aside from not accomplishing much clinically in terms of surveilling this public health issue, very little has been done to evaluate it in detail at the national spatial epidemiology level.
If there are programs out there that are trying to aggressive research this social phenomenon locally and regionally, I would like to hear about these actual events. With spatial statistics, we can evaluate these problems and search for the cultural and social "triggers" of these events, issues such as poverty, family unrest, sense of shame, day to day financial issues, inadequate social services programs . . . I am more than ready to develop a national population health study project devoted to this topic.
See on Scoop.it – National Population Health Grid
January 13, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Jenny McCarthy’s “One Shot Rule” for vaccines

[linked to an Article by Jenny McCarthy] The “One Poke per Visit” or “One Shot Rule” for Vaccines. Sounds reasonable.
Jennifer McCarthy states in this article:
“I am not “anti-vaccine.” This is not a change in my stance nor is it a new position that I have recently adopted. For years, I have repeatedly stated that I am, in fact, “pro-vaccine” and for years I have been wrongly branded as “anti-vaccine.” My beautiful son, Evan, inspired this mother to question the “one size fits all” philosophy of the recommended vaccine schedule. I embarked on this quest not only for myself and my family, but for countless parents who shared my desire for knowledge that could lead to options and alternate schedules, but never to eliminate the vaccines. . . . I believe in the importance of a vaccine program and I believe parents have the right to choose one poke per visit. I’ve never told anyone to not vaccinate.”
Source: chicago.suntimes.com
Jenny McCarthy can successfully "backtrack" all of her criticisms about childhood vaccinations with this logic. Her reasons or explanation for the strongly worded versions of her criticisms posted several months ago about vaccinating children seem reasonable.
In her article she explains her criticisms as follows:
[Quote]
"
Blatantly inaccurate blog posts about my position have been accepted as truth by the public at large as well as media outlets (legitimate and otherwise), who have taken those false stories and repeatedly turned them into headlines. What happened to critical thinking? What happened to asking questions because every child is different?
For my child, I asked for a schedule that would allow one shot per visit instead of the multiple shots they were and still are giving infants.
"
[End Quote]
In a review I drew up ten years ago about immunizations for a Medicaid Program working at 95-96% success if providing complete shots, one of the major causes I uncovered for overimmunizing and underimmunizing children was the use of combinations, and how much they varied in their rates of administration.
Was this a supply problem? I asked the team. Perhaps. Shortages two years before had caused a more than 25% reduction in normal year to year immunization series completions for children less than 2 years of age.
The availability of combinations certainly lessens the number of injections a kid has to receive significantly. The administration of three or four, or even five different single shots per visit to kids seems to be bordering on torture. McCarthy complained about six, and probably not all on the same body part.
McCarthy continues
[Quote]
"
“People have the misconception that we want to eliminate vaccines,” I told Time Magazine science editor Jeffrey Kluger in 2009. “Please understand that we are not an anti-vaccine group. We are demanding safe vaccines. We want to reduce the schedule and reduce the toxins.”
This is what I believe:
I believe in the importance of a vaccine program and I believe parents have the right to choose one poke per visit. I’ve never told anyone to not vaccinate. Should a child with the flu receive six vaccines in one doctor visit? Should a child with a compromised immune system be treated the same way as a robust, healthy child? Shouldn’t a child with a family history of vaccine reactions have a different plan? Or at least the right to ask questions?
[End Quote]
So, let’s do the math here – – –
There are 49 vaccinations required by the age of 6 (http://www.nvic.org/CMSTemplates/NVIC/pdf/49-Doses-PosterB.pdf 😉
36 between the ages of 0 and 2.
13 between the ages of 2 and 6.
36 vaccinations/24 months, or 1.5/month, 3 every two months, on the average. Ideally, the first 12 month’s worth of visits are at least every two months, if not monthly the first quarter of life. Including day zero or one as a vaccination day as well (for HepB), we have the possibility of 7 visits to given the bulk of these vaccines. That leaves a 15, 18 and perhaps 21 month visit, leading up the the end date of 24 months visit, totaling somewhere between 10 and 12 visits total for 36 shots. (The page linked to has one less visit for year 1, and no real visit counts implied up to 18 months, but the same range given above, minus 1).
the explanation McCarthy gives seems reasonable. But if you look at the combos required, there are just a few ways to produce the combinations needed to make fewer shots. The calendar is too complex for between shot periods. Based on the way the immunizations are sequenced, assuming traditional combos where they can be applied, the sequence for completion before two years of age is as follows (in numbers of shots).
1-8-7-8-1-10-1 (36) types of immunizations administered as:
1 + 4 + 3 + 5 + 1 + 5 + 1 (20) injections.
(again, see http://www.nvic.org/CMSTemplates/NVIC/pdf/49-Doses-PosterB.pdf
This logic, by the way, doesn’t take into account the 2, 3 and 4 vaccination combos out there (i.e. DTaP, MMR, the rare duplexes for the latter, a new 4some or two being tested).
The diversity or the product line is why we over-administer some more than others. The fact that some immunizations need 1, 2, 3, 4, 5 or even 6 administrations to meet the requirements (18 if you add the 12 influenzas requied for 7-18 years of age), only adds to what you may find, if you are searching for reasons to complain.
The point is, there is limit to the math skills required to determine if and how you are going to abide by recommendations. I guess the real question here is ‘what value do you assign to your kid’s life?’ These problems exist because of the value we assign to them. (And I admit, I wonder how many kids, if any, get the total numbers of flu shots recommended by the time they reach 18).
Parental responsibility is the issue here. If the kid had to take an epilepsy medication in some unique cycle, you would probably do it, right? A kid with diabetes needs that medicine when he/she needs it, not when some calendar says he/she should take it. A kid with asthma doesn’t wait until it’s too late (I hope). A kid in need of regular visit because he/she is unhealthy–wait, that’s also required for healthy kids as well–kids in need of well visits must attend to them for the same line of reason.
So imagine what Jenny McCarthy was telling us did happen, that there were people who abided by the rule of one shot per visit. How many visits would that require.
The math above says a minimum of 20 shots are needed with the combos available, or 20 visits in two years. That’s a little less than one per month. 12 visits the first year to be sure you meet the expectations, 8 the following year. Maybe with the first two months turned into frequent biweekly visits, to lower the pressure even more.
At 20 visits, $10-20 copay each, that $200/year. Not too bad, if you can afford it. On Medicaid, this could be a totally different problem to resolve.
So, let’s try no co-pay per well visit. Now you’re demanding much more physicians’ office time, maybe even doubling it per year per patient for pediatrics and newborn specialists, or kids with chronic diseases so young in life. This is just for 20 visits total. If you miss one, you narrow the time frame significantly about how and where to make up for that loss. If you skip it again, your chances drop further for completing the series on time. If you skip a third visit, even in the second year, you have little to no chance of recovery.
Now let exchange this for what if you skipped some visits, never fully vaccinated your child, and he/she was taken ill. How much would that event cost you? your insurance agency?
It not only costs you the cost of treatment and hospitalization for the illness, but also the possibility of post-infection consequences, changes in cognition, hearing, onset of epilepsy due to febrile seizures, potential for later life autoimmune and re-exacerbation consequences.
In 2011, a cost of $799,000 was assigned to a 2008 measles outbreak (14 cases, 363 suspected), involving the care of 7 people, in two hospitals. (http://www.modernhealthcare.com/article/20131130/MAGAZINE/311309983
The cost of having your child cared for if and when you mess up with an immunization isn’t cheap. Can you or your insurance agency afford the bill? (Celebrity status not included.)
In a very recent study it was shown that vaccinations save us $13.5B in direct medical care costs (Zhou, F., et al. (2014). Economic Evaluation of the Routine Childhood Immunization Program in the United States, 2009. Pediatrics, 133(4):577-585).
***********************************************
REFERENCES and other resources:
Is the Anti-Vaccination Movement to Blame for Disneyland’s Measles Outbreak? By Jennifer Swann | Takepart.com. January 11, 2015 3:56 PM. Takepart.com. http://news.yahoo.com/anti-vaccination-movement-blame-disneyland-measles-outbreak-205657288.html
For more on costs and immunizable disease outbreaks, see
Parker, A. A., Staggs, W., Dayan, G. H., Ortega-Sánchez, I. R., Rota, P. A., Lowe, L., … & LeBaron, C. W. (2006). Implications of a 2005 measles outbreak in Indiana for sustained elimination of measles in the United States. New England Journal of Medicine, 355(5), 447-455.
http://test.naccho.org/topics/HPDP/infectious/immunization/upload/2006NEJM-Parker-Implicationsofa2005measlesoutbreakinIndianaforsustainedeliminationofmeaslesi.pdf
Sugerman, D. E., Barskey, A. E., Delea, M. G., Ortega-Sanchez, I. R., Bi, D., Ralston, K. J., … & LeBaron, C. W. (2010). Measles outbreak in a highly vaccinated population, San Diego, 2008: role of the intentionally undervaccinated. Pediatrics, 125(4), 747-755.
http://pediatrics.aappublications.org/content/early/2010/03/22/peds.2009-1653.short (more than $10,000 per case, 750/day for quarantine.)
Zhou F, Shefer A, Wenger J, et al. Economic evaluation of
the routine childhood immunization program in the United
States, 2009. Pediatrics. 2014;133(4):577-585.
Mona Patel, MPH; Laura Pabst, MPH; Sajal Chattopadhyay, PhD; David Hopkins, MD, MPH; Holly Groom, MPH; Stuart Myerburg, JD; Jennifer Murphy Morgan, MSPH; and the Community Preventive Services Task Force. Economic Review of Immunization Information Systems to Increase Vaccination Rates: A Community Guide Systematic Review.
http://www.thecommunityguide.org/vaccines/vpd-jphpm-ecrev-IIS.pdf
The Value of Vaccines in Disease Prevention
http://www.pfizer.com/files/health/VOMPaper_Vaccines_R7.pdf
See on Scoop.it – Episurveillance
January 4, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on “Ebola” on the Medical GIS ScoopIt!
In the past 14 months, I posted 556 pages on my ScoopIt devoted to GIS and HIT (sum, approx. 8500 views, 4250 viewers).
85% of these viewers visited the 3 sections of this ScoopIt! known as ‘Episurveillance’, ‘Global Health Care’, and ‘Medical GIS Guide’.
I then dissected the postings down further to evaluate those related to the current Ebola outbreak. These are my results.
Medical GIS: 2653 visitors, approx. 5600 views total; 217 postings total, 91 for Ebola (42%)
Episurveillance: 736 visitors, approx. 1400 views total; 222 postings total, 78 for Ebola (35%)
Global Health Care: 401 visitors, 783 views total; 117 postings total, 61 for Ebola (52%).
To define the pages posted, I evaluated the primary purpose and content for the main article(s) cited. Some pages contained by to 50 articles with links provided, with articles varying considerably in their content.
The primary topic of the posting was the focus of this review (which was a consolidation of the articles content). These articles, publications, books, speeches, quotes, photoessays, and news items referred to one each page were evaluated, and the primary theme defined.
At the time these articles were posted, there was of course my own biasedness in selecting what to post once October 15th was reached, and it was determined that Ebola appeared to be past the prime of its potential ecological migration to North America in the immediate future. I ended the evaluation of all articles on the internet related to Ebola on October 31st, but continued reviewing the main news features or topics about Ebola as the total numbers of these articles accelerated considerably throughout November and December 2014. I posted pages detailing to primary hot topics as new ones arose or content and reactions to the disease changed.
I provided 2090 links (references provided) at my entire ScoopIt! for these three sections, 1090 (51%) of which were in direct reference to Ebola (excluding my history writings). By the end of 2014 I had posted 230 pages on Ebola, 138 pages on other surveillance matters such as the measles, mumps, whooping cough, polio, MIRS, Chikungunya, and encephalitis outbreaks, as well as a number of socially important surveillance related diseases or disease matters such as immunizations and refusal to immunize (36 postings, 62 links), infibulation and other cultural issues (64 postings and links), and teen age suicide and similar teenage or children school and health related matters (14 pages, 70 links).
I used this to identify the hot topics in medical GIS for 2015 (more details on this part of my study later).
These findings in turn provide reason for establishing a live Medical GIS station at the typical standard health insurance company, managed care, PBM, and large university hospital/teaching institution settings.
The purpose of such a GIS would be to monitor: 1) in-migrating disease patterns, 2) cultural and ethnically linked public health matters, 3) ICDs, E-code and V-code indicators of the most socially important public health concerns (abuse, violence, poverty-realted ICDs and V-codes), 4) local low SES related population health patterns, 5) local standard infectious and environmental host-vector disease rates, 6) immunizable disease rates (whooping cough, etc. outbreaks) and anti-immunization V-codes, 7) culturally-linked or specific ICD public health indicators (Tb infected newborns in Pac NW), 8) culturally-bound syndrome ICDs, and 9) complete disease pattern profiles (75-150 ICD profiles) for the major ethnic groups in the region, such as African American/Black (subtypes?), Hispanic/Latino/a (and subtypes?), Asian (subtypes?) and Native American.
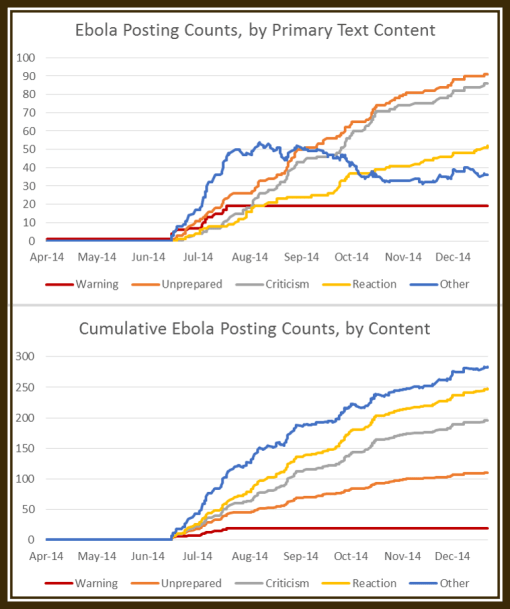
For this study of the Ebola topics referred to in the illustration here posted, the line charts demonstrate the periods of different behaviors related to this outbreak. I categorized the articles content in what I call: [RED LINE] the warning period (people like myself voicing our concerns/need for an immediate WHO/CDC response), [ORANGE] articles that focused on the CDC, WHO and agencies being and acting as though they were unprepared for the outbreak (even months into it), [GREY] the articles in which public and professional criticisms about this lack of preparedness emerged, and [YELLOW] the articles occasionally posted focusing just on the official reactions to these criticisms by WHO, CDC or the attached governments.
The articles counted as ‘other’ [BLUE] did not fit into these four classes and were usually about non-critical case/death counts, news about the Ebola spread without judgmental statements or conclusions made, news flashes about the results of new studies of Ebola or its treatment, pharma news, stock investors news, African economy and ebola news, etc.
See on Scoop.it – Medical GIS Guide
