
Unani Symbol that appears at the beginning of or in many Islamic writings about medicine. . .
“He is the Healer”
The first third of this project was on Unaniism, an ancient form of medicine about to become extinct. Unaniism is a subgroup of Arabic medicine that was almost lost to history. It was brought back to life in the 1970s by its leading promoter Dr. Hakim Mohammed Said (1920-1998). He brought its knowledge to several international programs and WHO during the late 1970s. This resulted in an attempt to preserve this nearly extinct piece of Arabic tradition.
The assassination of Dr. Said in 1998 (see his biography at http://en.wikipedia.org/wiki/Hakim_Said), led myself and others to be concerned with the possible extinction of this unique cultural form of medical practice. However, a few years later, 9-11 came. For obvious reasons, the official research project stopped, but I continued my work on completing a combined qualitative-quantitative research portion of it as part of a 15 month certification program. I completed this work in Spring of 2002.
(This will probably put me on a watch list for Homeland Security.)
Hakim Mohammed Said is to the back left, in the white shirt.
Significant parts of this combined Quantitative-Qualitative review of public health pertain to the method I designed in 2001, and are based upon a program that I taught every year at the university from 1992 to 2000. During that time I researched, taught and wrote about Aztec, Native American, Inuit, Southeast Asian, East Indian Western and Ayurvedic, Chinese (TCM), and Sufi forms of medicine, to name just very few.
Combining Two Distinct Methods of Research and Analysis
Combining qualitative research methods is the best way to produce a more credible quality assurance or treatment methodology-based research program. Traditional researchers place much of the emphasis on a single or few methods of researching outcomes, and usually opt to focus on just a parametric approach or a non-parametric approach, with the opposite of whatever approach was selected as the primary method of research, used to add details and otherwise important “fillers” to the research project and its final reports. This is for the most part how traditional QIAs and PIPs are carried out for employee health, Medicaid, Medicare and other HEDIS/QA-assessed, annually evaluated medical programs.
The problem with this methodology is first, the qualitative work that is employed in most projects is never completely engaged in, but rather added as decoration to the project as a whole. This way, the methodology put to use is often simply overlooked, not at all described, or detailed in such a way that its identification as a qualitative analysis method is never confessed to in the final reports. This way the qualitative research methods put to use rarely if ever undergo the same scrutiny as the overall quantitative portions of the report.
Recent events in the design and improvement of medical program review methodologies have also included the requirements that more detailed, much lengthier reviews be carried out with each knowledge-based teaching activity and every clinical skills training program that is out there. The best and only way to do this is by combining qualitative and quantitative research methodologies, noting from the beginning the needs for engaging in this type of research method.
![]()
Examples of Application
Part 1. Designing the research project.
A good rule is to chose a broad-sweeping question and then dissect it down into its research defined subcomponents. To accomplish this, you must first provide a very brief description of what you wish to do and why it has to be done, and then try to put it into perspective with the recent, current and potential future needs related to this topic.
Research question: what impact will Unaniism have, if any, on the local health care system in the upcoming future?
Argument for need for this research: Unaniism is a unique medical philosophy practiced by a fairly small population of Middle Eastern people residing in Iran, Iraq, India and the neighboring countries. Unaniism is important to the local cultural anthropology of the people who practice it due to its pivotal role as a part of their heritage. This philosophy very much relates to other philosophies already in practice, many globally, such the philosophies related to homeopathy, ayurvedics and Chinese medicine. Due to recent political clashes and turmoil in predominantly Islamic communities, the more western tradition of Unaniism is at risk of becoming eradicated as a part of the multicultural heritage of the Middle East. This in turn results in the migration of people practicing Unaniism to other parts of the world, in particular the United States. Like any past culturally defined medical practice, this implies that in the future, Unaniism could very well become a part of the medical traditions practiced in the United States, much like the development of chinese medicine and acupuncture, ayurvedics, Hispanic-Mexican-Hispaniolan medical practices, some Native American traditions, and certain Carribean and Cuban medical traditions such as hoodooism and voodism.
![]()
The reason we have to combine quantitative and qualitative methods is that in most research programs involving small group analysis, qualitative analysis offers more insights and solid results for people-related issues. This analysis process is carried out with a restricted group of eligible participants, who are defined by a particular feature they share such as participation in a health education program and follow-up process, participation in a specific activity that the results of have to be monitored, or engagement in a particular event or change in health that qualifies them for the study. Such examples would include an individual who makes use of specific over-the counter remedies in combination with a prescribed drug therapy for hypertension or some other chronic disease issue, individuals engaged in both alternative and regular procedures designed to target a specific biopsychological problem like Restless Leg Syndrome, or a culturally-bound syndrome linked to a specific population such as the Sudden Unexplained Nocturnal Death Syndrome (SUNDS) involving Laotian immigrants. Each of these require human behavioral and thought-process evaluations that cannot be researched effectively using just the standard quantitative research methods. Instead of substituting the quantitative method with a qualitative method, it is recommended that the two methodologies get merged to form a single, reasonably flowing research plan that combines both quantitative and qualitative measurement processes.
Depending on the study topic, the size of the focus population and the research methods employed, “small” group values can be as large as 1000 for large population settings, but are usually <100 and involve topics that are hard to develop significant eligible population sizes for. When defining your start-up population, it is important to note that there is a certain amount of loss of participants that will take place in the research program, for which reason the methodology has to take into account a later response frequency that is far less than the response frequencies experienced at the beginning of this study. One has to assume from the beginning that the research project is going to end with exceptionally lower counts of participants, and take this into account when predesigning the statistical methods to be used.
The best way to prepare for such a program means that you have to assume and be able to begin the study with a valid quantitative method, with adequate numbers of respondents or research participants, and then expect and prepare for an intermediary measurement process that involved fewer participants, hoping of course for a 100% response rate. This second phase should have 50% or more of the original population engaged, but may be as low as 25% or 33% (one-third). The problem with having a lower second phase response or participation rate is you have to make up for this loss as part of the third phase of this research process. It is safe to assume that the third step can involved as few as 6 or 7 individuals. The only problem is, the smaller this final group of participants becomes, the more details your work has to be sure to focus upon during the second and third stages of study and analysis.
![]()
Part 2, Designing your Methodology
As a graduate student and public health worker, you have identified several hundred people on campus or affiliated with the university hospital settings who are from the Middle East. In passing in your conversations with these students/patients, you learn that some have a heritage related to one or more of the countries known to be practicing Unaniism. You then ask them if they have heard of this practice, and their responses demonstrate the need to further pursue this research question.
You decide you would like to determine how many of them are familiar with Unaniism and its distinct medical traditions. The following are your possibilities for researching this group. You may choose to perform one of more of these.
-
Develop a Survey targeting the entire campus population, with a selection process that depended solely upon upon students passing through an area such as the campus union building or cafeteria, and convincing them to engage in this survey process. You might at first decide to perform a brief survey of 7 to 15 questions designed to determine the relationships students have in general to possible students familiar with Unaniism. (Targeted number of responses for this = 600 (there’s a reason for this n; n > 576 are statistically more viable population related response counts, a tradition relied upon heavily by NCQA-related health study methodologies; this allows for 10% failure or exclusion due to ineligibility, poor responses, and uses a reached total 2^n value).
-
Develop a more focused study targeting specific individuals with some sort of awareness with Middle Eastern traditions in general, inquiring into such traditions as Sufiism, Old Testament and Islamic medical traditions and Unaniism. (n ~preferred 275, but possibly as low as 100)
-
Develop a focus group project on this involving 10-20 students, of various age groups. Repeat this focus group project once or twice, to define changes in attitude and knowledge base that may have taken place due to your project.
-
Develop a way to independently perform a case studies review of specific students and professors and other staff members who are recruited in order to help to understand and define any generation-related differences that could exist. Produce a detailed flowchart of the case study method. Define possible measurable outcomes of this type of review.
-
Produce and apply an open system classification review of the results of the previous three studies. Use this to develop some sort of grounded theory approach to analyzing your findings. Quantify the qualitative outcomes of this open classification-grounded theory approach to analyzing the data (using a bimodal and/or ranked score approach).
How would you go about doing this?
![]()
An ideal pattern of participation and responses would be something like 100 initial respondents, 40 to 60 stage 2 respondents, ending with 15 to 20 final responses. A plus or minus 10-15% in counts is allowed for this population size plan. The main reason for these limitations with numbers pertains to the validity and reliability of the statistical processes involved. The third stage of a review might only require a half dozen respondents assuming each respondent provides a fairly thorough set of responses enabling ample amount of qualitative research methods to be applied to the study. With these small groups analyses procedures, we want to treat the qualitative review as some sort of focused ethnographic research method or a related content analysis research method. It would not be unusual to applied a grounded theory like of approach to this data assuming there is enough content, but it might be better to assume that an analysis performed for this third and final stage should be more a query of content that can in turn be applied to the more important results and suppositions made based on the stage 2 analysis.
The steps involved with the Stage 2 research process are perhaps the most important part of this 3-step process. If stage 2 processes are muddled or not properly engaged in, the links that can be drawn between the initial findings and the long-term end results of the program (stage 3) can be absent from the results that are produced. This is the most important process in engaging in a 3-tiered combined qualitative-quantitative research process and is the reason these types of program normally failed in the past. The large amounts of criticism drawn by performers of combined research programs fail due to methodology mistakes that are made and the lack of adequate planning or appropriate planning and application of the combined qualitative-quantitative research process. The types of topics these methods are applied to can also influence overall success of the program. It is important to make sure the types of topics reviewed using this combined methodology have components that are measurable numerically, and others that can be recoded into numeric values for engagement in frequency analyses at the statistical level, and overall outcomes finds, which are very much qualitative in nature, than are linkable to the intermediary and initial research stage findings.
We cannot apply this 3-tiered process to a study of Heart attack history, followed by changes in prescription drug use, followed by changes in cardiac output measures. These are all numeric biological measures; none of these measures are biopsychological in nature. This latter project is best performed using typical ANOVA-like procedures or some other quantitative measurement evaluation method. But if we add to this study reviews of patient attitudes, preventive practices, physical and emotional activity performance, and preventive habits, we have the human biopsychological components needed to perform the 3-tier process for evaluating the overall prevention program being tested. The use of this method over standard quantitative procedures heavily relied upon by other cardiac disease programs for example, provide more of a humanist value to this project. It requires a little more work at the researcher’s level, but provides more valuable information in the long run in terms of preventive practices and developing public health disease prevention or reduction procedures.
![]()
Example 2. Culturally-bound syndromes.
Research question: Are there any culturally bound syndromes that could be related to the possible influx of Unani or Middle Eastern people?
Argument: Culturally-bound syndromes are a common consequence of in-migration into this country by migrants with a unique background, philosophy and tradition. The in-migration of Laotians during the late 1970s for example led to a syndrome known as Sudden Unexplained Nocturnal Death Syndrome (SUNDS). The assimilation of Native American groups in the mid-1900s led to the development of a “New World Syndrome” complete with the early onset of diabetes, gall bladder disease an obesity (currently linked to the western cultural renaming of this health problem as Metabolic Syndrome).
Follow-up questions: What types of culturally-bound syndromes may develop in communities formed by the in-migration of older and younger generation Unaniists? What cultural beliefs may play a role in the development of these conditions? What additional costs and stresses could such features produce on the current social services agencies and attached health care programs?
Conclusion: a significant amount of planning has to go into the implementation of the above two examples of this kind of research. Targeting an audience in regard to culturally-defined topics does have risks attached to the study process. If just students are involved, one could take the typical Psychological programs approach and post descriptions of these study topics, require that basic psychology enrollees participate in two or more of these, or offer a 50 dollar reward or Starbucks card for participation. The clinical avenue could be taken as well, asking for patients to become more active in this process. The MSW approach involves the engagement of social services agents well trained in serving the particular group being researched. Either way, the value of the study and its application is fairly significant. The main barriers to over come include the Human Subjects Review evaluation of your method, and how and whether or not to involve the actual clinical setting in with this process, or to engage in this research at more of a community level, such as within a community meeting room setting.
Research Question follow-ups/study questions: what the culturally bound syndromes for such a cultural setting? What physical conditions or health concerns are there? Is there an epidemiological transition process that might have to be considered?
![]()
![]()
Typical Combination Methods Research Populations
The research populations and study processes therefore have to be multidimensional in nature. The population involved has to be fairly well-defined, and the qualitative and quantitative measures to be taken well though out and planned accordingly. The problem is, the second phase of this type of program requires the application of grounded theory methodologies, which begin with no assumptions on behalf of the population and their outcomes. This method begins with the assumption that the researcher will evaluate results, find those results that stand out the most, begin to categorize these outcomes in order to review the same data for a second time in order to determine what types of relationships exist between the various findings, followed by a review of specific types of outcomes with the goal of quantifying their incidence. Population size is what determines how detailed and how long this stage 2 evaluation process will take.
Once again, to avoid loss of data and participants, carefully select your initial population if the beginning population is too large, or choose a research topics that results in a population find that meets certain size restrictions and research standards. For many such studies, numbers is not much an issue, expect in terms of often resulting in too small a number for the research population. In the case of asthma studies for example of Medicaid members, even a sizeable Medicaid population could result in just a handful of asthmatics that meet the study age, for example childhood onset asthma cases in which the need to determine causality (emotional/stress, biological, allergy-induced, environmental living conditions-induced, etc.) and future prevention practice planning processes have to be developed. In a research population (all members, all ages) of 30,000, it is not unexpected to have only a few dozen childhood asthma cases to related this research methodology to. This may be too small of an initial population to initiate this type program with. If we were to apply this program to the same overall population, but instead focus it on another biopsychological, social concern, such as teen pregnancy and child care review, we could obtain more participants, enough participants to produce a beginning population of 100 or more, allowing for a 15 month overall project to be engaged in with a projected follow-up response rate of just 10% or less. This small number of long-term follow-up participants would be enough to allow for some detailed analyses of the focus group data or follow-up survey responses to be engaged in.
Summarizing this group size related problem: in some cases drops in participation can be as much as from 1000 students, to <500 initial respondents, to <200 post-respondents, to <50 long-term follow-up respondents. In the best applications for this methodology, we should try to target these values as 200-300 initial participants, reduced to 50-125 for stage 2 activities, followed by a few dozen stage 3 activities. By applying and targeting these estimated response and participation rates, the results and applications of this research methodology can be extremely effective. For this reason, it is best to apply these medical research activities by focusing on specific medical conditions and treatment modalities, involving just a couple of hundred participants, even for the more common medical conditions like diabetes, hypertension or mental health related matters. These low numbers make it a necessity for a research group to have highly skills quantitative and qualitative researchers standing by, with methods in place for transferring the focus of an activity from one pertaining to high numbers or participants or response pools to exceptionally small pools of results.
![]()
![]()
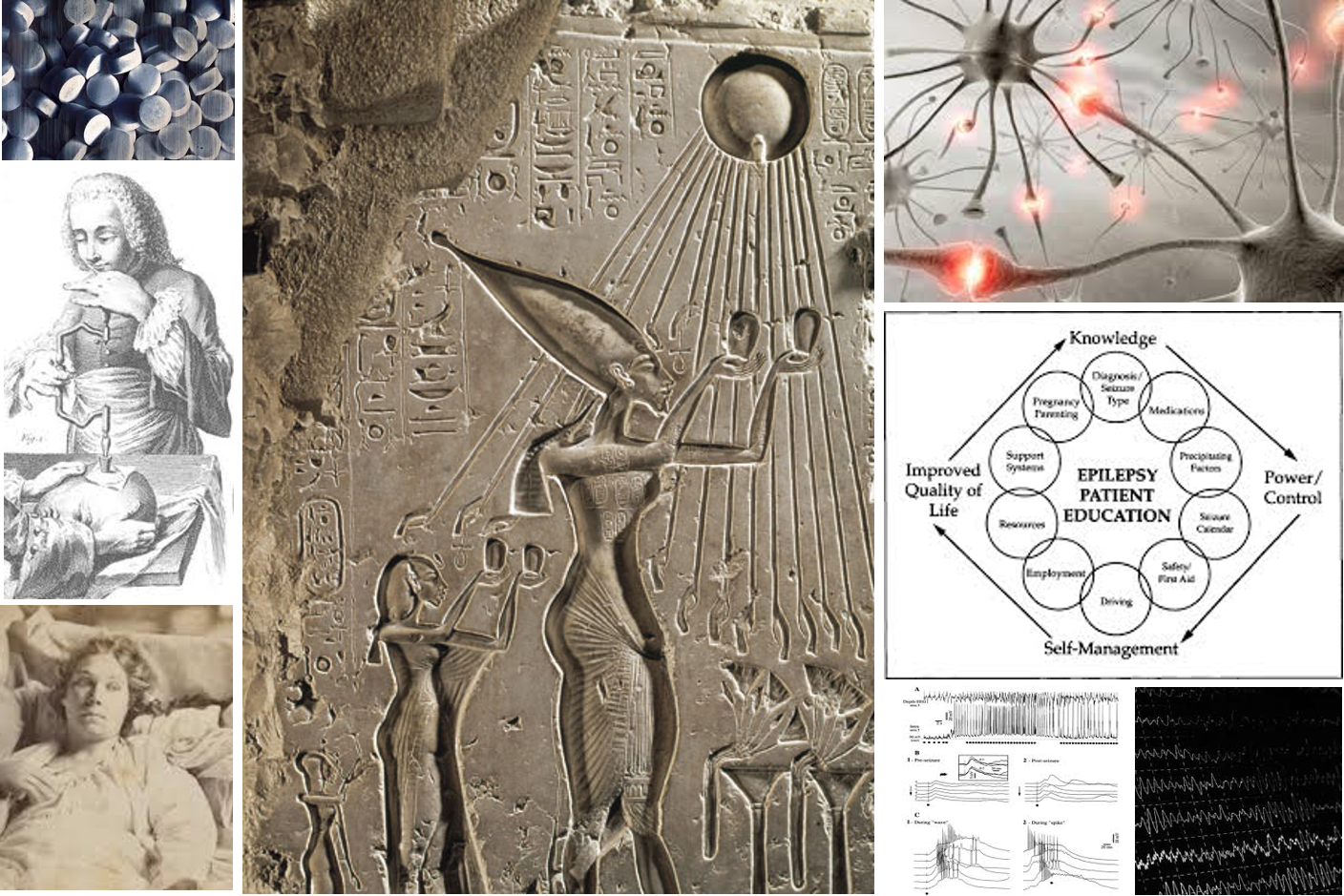
Example 3. Epilepsy.
Research Question: Are there any cultural differences when it comes to a personal viewpoint regarding epilepsy and the impacts this condition can have on the quality of life issue in other communal or cultural settings?
Epilepsy is very much a culturally-bound disease in the social context, even though we usually don’t consider it as such. The impacts society and people have on people with epilepsy relate directly to their quality of life and their long term medical treatment and history. Past studies have demonstrated that within certain cultural settings, epilepsy is a condition not revealed due to the value society places on people with this condition. In some cultural settings, the history of seizures seems to have certain “values” attached to the diagnosis culturally and financially, making it more common in some countries according to WHO statistics. For example, one study showed that in Nigeria its frequency was higher due to the attachment of epilepsy with a stable income source akin to welfare and the limited employment expectations for these people. In parts of Canada and Russia, it may be culturally perceived as an even attached to the culturally-bound syndrome Pibloktoq or shamanism.
Very large university settings have the unique opportunity of researching the interpretations of this condition, involving individuals (domestic and foreign students and staff) with varying experiences both culturally and personally, with regard to the popular viewpoints and behaviors related to this disease at home or abroad.
The types of question that could be pursued with this study can focus on: does the student being surveyed have knowledge of someone with epilepsy and the social reaction that exists for this history abroad within other cultural settings? if yes, what parental reactions to this condition did the student learn in the traditional home setting? if no, what attitude does the person have about this condition or medical history? what aspects of biology and life does the individual perceive as the cause for this condition and the potential cause(s) for this condition as it recurs and worsens over time?
We can add culturally related aspects of this study by engaging people from other known national or cultural upbringings. It would be very interesting for example to identify the distribution of traditional knowledge of disease with modernized knowledge of disease within Hispanic student settings. When they were kids, these individual were raised in a household setting where tradition sometimes impacted the quality of care a person with epilepsy received in their community. They are witnesses to how that community treats these people. In addition, a Mexican community is not homogenous. How does an indigenous family treat a child with epilepsy versus a family of Spanish descent? or of a neapolitan coastline nature versus high elevation nature? There are indigenous and Euro-indigenous peoples and more recently European post-Santa Ana families with very different lifestyle traditions and medical beliefs. WHO statistics show epilepsy is about twice as frequent in Mexico than in the U.S. How will the higher epilepsy statistic in Mexico transfer into the United States? Does it follow the in-migrant patterns, or does in-migration have the same effect it was noted to have with very health Italian descent Alameda communities in California? (They came in with long life expectancies and healthy outcomes in spite of their diet; after a few generations they were Americanized, social inequality then developed in the communities, and therefore diabetes and heart attack rates increased.)
![]()
In sum, the ongoing problem of researching specific populations in order to produced the best, most effective prevention programs requires that a combined qualitative-quantitative research method be developed that can be used to take advantage of the different research techniques and skills available to the research team. The development of a fairly sophisticated cross-matching method is required such as combining information obtained from quantitative methods with information obtained from qualitative research methods. This is the best way to analyze a fairly small population over a period of time of more than 6 months, especially if the study lasts a year. This requires a combination of predetermined and undetermined measures to be produced as the result of such an activity. The predetermined measures are the standards which such a program begins with, followed by un-predetermined findings that have to be developed through the use of grounded theory analysis, combined with non-parametric-based measures thereby quantifying these outcomes, and then followed by a post hoc follow-up review with the goal of linking the stage 2 process and outcomes to the stage 1 standard outcomes measurement processes, whilst also providing additional support and proof of the stage 2 findings, further proving the efficacy of this research methodology. Not an easy process.
To produce open responses that can be correlated with the rest of the study, specific rules of coding and evaluating response content should be used. These general rules are applicable to all such clinical studies and do not introduce any likelihood for biasing the results and evaluation process. Since these studies are to be performed on public health related clinical studies as part of a long-term 12-15+ month evaluation process, these topics that are reviewed and then redefined in some statistical oriented fashion are standards, at least some of these will always exist within the researched activities or actions engaged in. They are based on the standard protocols that already define the clinical activities which all types of health givers are required to engage in.
![]()
Example 4. Pregnancy-related Diabetes.
Research Question: Is there a relationship between Age and Body Mass Index and the onset of Pregnancy-related Diabetes in mothers who first become impregnated at an age <30?
Methodology: Review past medical records for all women in that age range between the years defined for the study. Focus on mothers with a history of 2 to 4 pregnancies for the years selected for this research period. Document BMI, age, ethnicity, and other useful information regarding pre- and post-partum visits and any documentation of ongoing BMI changes witnessed due to these visits. Information on these cases is obtained using the standard NCQA/HEDIS methods and requirements for eligibility. A focus group study may be required for this study.
![]()
This last example resembles a typical combined qualitative-quantitative research project for a managed care program. In fact, this example is based upon a real program I developed, initiated and tested for such a reason. To fully develop this program prior to use, the following questions had to be answered and/or processes needed to be developed to find answers to them. In addition, a projected outcomes could be defined based on this overview of the topic in general.
- What people’s behaviors (expecting mother’s behaviors) could make prenatal mothers more susceptible to diabetes?
- What possible reasons for pregnancy-related diabetes are not easy to prevent or treat?
- What barriers exist to patients with regard to engaging in these prevention behaviors?
- What are the advantages of focusing on the BMI issue for this kind of study?
- How can one correlate a BMI analysis for this study to some other standard study such as an obesity, immunizations, well visits performance, or nutrition/maternal care study in order to produce a culturally focused quality of life/neonatal-infant health outcomes study?
.

.
3-Part (3-Tiered) QA Programs: the Clinical Study
There is a way to better analyze population health and remain personal and culturally-minded in your approach to population health, even when large populations are involved. More thorough evaluations of patient health data provides us with more ways to evaluate, treat and then use these results to develop better prediction models for health programs. One value that qualitative research methods have over quantitative methods is that personalized approach that is developed, meaning the focus turns to the patient, not the system or the parts of the system engaged in the health care process.
One can look at each research question proposed for a given PIP or QIA and ask the following: does this research question address an issue that is mostly 1) systems/policies/protocols, 2) PCP service provider (nurse, doctor, technician), 3) facility/office/hospital, 4) cost/insurer related, or 5) patient behavior related. Most outcomes are reviewed with the goal in mind of identifying possible barriers and then developing interventions or action plans. The first four of these five barriers are the most common actions taken when a study is over and the report is developed trying to define whatever next actions need to be taken. The purpose of incorporating qualitative methods into these projects is to more fully understand the barriers that exist specifically for patients. More targeted, more direct changes can be made and overall outcomes improved by involving the patient in this process personally and even behaviorally, by engaging them in specific intervention activities.
A Study of Insomnia treatment as an example. In another study I did, this time using grounded theory methods, the initial methodology question I asked was how do I make the best use of case reports to document changes in clinical practice? For two CMA credits, a physician participating in a program was asked to provide 5 pre-education case studies per patient, which would be followed by another set of 5 post-education case reports for patients treated using the new methodology he was taught. On day 1 of this activity, the 5 base reports were handed in, with options of 10 and 15 reports for those who wished to receive more credit for their work. They then underwent the day long education program, with standard pre-post knowledge based surveys administered. Then they were asked to go home and treat patients over the next year, providing case reports in sets of 5 to document their post-education behaviors.
These case reports consisted of a number of standard short answer and open ended questions to be asked of the caregiver or asked about the patients of the care giver. Once these cases were reported to the primary instructor, the data was then entered into a spreadsheet. As part of the evaluation process, attention was paid to content being entered during the data entry process, and repeated phrases or specific terms that were repeated were cataloged for grounded theory use (i.e. recognized and highlighted/color coded, and if time allows, copied and pasted into a separate column).
The focus of this study was patient-doctor interactions. So some of the questions pertained to physicians’ change in practice (implementation of a new protocol, changing the drug that is given, entering more data about patient’s S/S, applying a survey or specified set of diagnostic questions), others to patient behavioral change (engaging in a survey, keeping a sleep diary, noting impacts of sleep schedule changes, engaging in better pre-sleep and nutritional supplement related behaviors, seeing a counselor if needed for insomnia or sleep apnea complications). Text analyses were then performed in which the key words previously entered and cataloged were then quantified, and pre-post practice habit changes quantified.
Three-Part Programs. Unlike QIAs and PIPs, this methodology focuses on the health care system instead of just the physician or just the patient. The measurements for such a method of research require that both clinician and patient activities be evaluated and assessed or scored, and that certain intervention activities or plans be designed and implemented, and that a follow-up measurement be taken at least once to statistically determine whether or not long-term changes took place. These changes will be either in physician performance and outcome, or patient response, performance and outcome.
For example, in the case of ongoing asthma, hypertension, diabetes or epilepsy treatment, all of these chronic disease require or necessitate that some sort of personal involvement on behalf of the patient become the standard for long-term assessment processes. This type of event requires that patients monitor their health status on a regular (daily+) basis, by documenting such things as changes in health condition and their suspected triggers, documentation of certain vital signs or symptomatic readings (comfort with pollen in the air, frequency of seizures that day, regular blood pressure readings, blood sugar levels, etc.), or emotional and psychological reactions to specific stressors. This would be a measure of the patient engagement process produced by a physician-patient interaction, and is a measure of physician performance.
As another example, there might be a certain requirement or protocol recommendation for treating specific medical conditions, such as an ongoing periodic review of antiseizure medication blood levels, the quarterly measurement of HgA1c in diabetic individuals, the measurement and documentation of at least 2 or 3 blood pressure readings per office visit, the review and documentation or recent COPD-related signs and symptoms, the review and entry of patient medication histories when assessing certain types of biopsychological or psychiatric cases. The ability of the PCP to engage in this process and then document the results is essential to long-term care of these individual; by measuring its absence, dismissiveness or presence, we document the value of the visit and PCP activity as a whole, not necessarily just the health of the patient.
For a third example, it helps to visualize the most important parts of an office visit with your required PCP, or due to a specific disease history, your required specialist. In the case of an office visit with a cardiac specialist for example, the most standard parts of the office visit are
1) a review of the overall medical history,
2) a review of the specific reason for a given visit (a specific medical condition the doctor is supposed to treat, discussion of its history, etc.),
3) the methods in which this problem have already been dealt with,
4) the physician’s notes on his/her clinical observations of the patient with regard to the specific medical condition,
5) a review of any comorbidity-related problems possibly linked to the reason for the visit
6) the activities the physician asks the patient to go through personally pertaining to this problem,
7) the activities the physician asks the patient to go through in terms of further his/her personal and professionally-defined level of involvement in diagnostics and treatment (visits with others, ongoing education and psychological counseling activities, etc.)
8) the current state of medical treatment for the condition (script and non-script, OTC and non-OTC, behavioral activity or non-activity based),
9) discussion, development or design, and documentation of some planned intervention process for dealing with the condition,
10) engagement of other specialties and specialists for this condition and its comorbidities,
11) the definition of recommended or expected changes in script and non-script related treatment modalities,
12) the follow-up and review any or all of the above recommended practice activities or patient activity changes, to serve as evidence for ongoing intervention and change at both physician and patient levels (evidence for patient compliance, patient engagement in note-taking, dietary changes, recommended activity changes, or self-imposed additional help practices such as counseling, etc.)
Measures can be established to document the absence or presence of each of these twelve important steps in the patient-doctor intervention process. To produce these measurements in a combined qualitative-quantitative manner, a standard method of documentation and analysis of patients medical state is employed, followed by a more detailed review of the same information but with more attention paid to specific measurable therapeutic or clinical details, followed by an even more focused review at the patient level, physician level or both, pertaining to the perceived accomplishments made due to this intervention activity.
The standard method to engage in these intervention programs, a standard pre-post-postpost or year1-year2-year3 approach is made focusing on population health features to determine whether or not internal practices and practice changes resulted in measurable outcomes. This method uses a standard chi squared, t-Test, or occasionally ANOVA method to measure changes and outcomes. These measures, although highly valued due to their quantitative method, are not necessarily the best ways to measure failure or success in terms of ongoing (>12 month) review processes. To make up for the problem brought about due to over-reliance upon the standard quantitative method, the qualitative steps of this type of program need to be redefined into some more detailed qualitative way of measuring outcomes that can be related with the standard quantitative format. Such a change in methodology is this purpose of this new method.

A highly controversial cultural topic in U.S. medicine is infibulation. The most common form of this is a ceremonial and traditional African Muslim practice in which a physician surgically closed off much of the vaginal canal outer orifice, preventing sex but allowing for menses flow, until she is married. My study of the distribution of this practice in the US revealed four peak age groups, two of which were representative of age groups that had this done before their in-migration into this country. The other two age groups (young children, and young unwed years) suggest this process is being done in the U.S. See Infibulations_Project. [My study of the national data for this ICD9, over a ten year period; released for the first time; it takes a while for the pdf to load. Key to interpreting these results: pink-blue population pyramids are counts of female-male; dark brown and tan are prevalence rates; the major gender researched here is female. The age bands evaluated are in one year increments (another first). Look for recurring age spikes. Data available upon request and submission of proper IRB approvals and releases. The above maps are reviewed briefly as well in Pinterest at http://pinterest.com/pin/568790627908909180/]
Patient-and Provider focused 3-Part (3-Tiered) QA Programs
A 3-Part/Tier methodology of intervention program planning and management was developed for teaching, training and reassessing clinical performance of clinicians performing a single series of tasks targeting a specific medical need or specific type of intervention preventive medicine process. This method is applicable to numerous topics commonly reviewed as a part of a combined clinical education-clinical performance QA review, and works best with medical problems or quality-of-life issues common to recommended Quality Improvement programs.
The 3-Part/Tiered system consists of three steps in teaching and skills training:
- 1) teaching/learning process= increased information availability and acquisition,
- 2) planning/implementation process=increased knowledge on how to apply this educational material, along with improvements in practice-skills related confidences combined with the opportunity for implementing these practices, and
- 3) execution/documentation process=individuals engage in the education program demonstrates knowledge and skills for performing these the measurable skills by developing the confidence needed to apply them to a clinical setting, documenting these skills both before learning the actual clinical application skills and after learning these skills, following their return to a clinical workplace setting.
This methodology also requires three information gathering steps be engaged in:
- a) pre- and post-testing in order to measure knowledge base and competence of each clinician,
- b) pre- and post-case reviews collected in order to quantify the qualitative information normally provided as part of a standardized patient case review, and
- c) a long-term post-activity follow-up designed to ask one or two questions pertaining to the program, with the goal of obtaining fairly lengthy text responses detailing the most important benefits, outcomes and limits to the program under review.
![]()

![]()
Example 5. The Insomnia Study
Physicians who are primary care providers are asked to engage in a program that involves a new treatment plan for insomnia. This new treatment plan consists of several steps–documentation of a full history using a standardized survey tool, documentation in the medical records of the kind of insomnia experienced by the patient, medication monitoring before and throughout the research process for treating these patients, the education of the patient with regard to medication use, involvement in a specific number of training sessions designed to teach individuals how to better deal with insomnia, make distinct mention of the use of a sleep diary, include diet-beverage related activities in the dairy, and a discussion on the role of personal engagement in processes designed to prevent or reduce insomnia problems. (I base this on a real study I was the statistician for about ten years ago, resulting in a brief revitalization of grounded theory approaches in the business world of medicine; a new OTC supplement or a similar product in the form of a prescribed medication could be promoted.)
A survey is administered to the primary care provider before, during and after this 15 month study of insomnia treatment program. PCPs are encouraged to submit as many cases as they can up to 15 for each of these three time periods. These cases studied are provided with unique identifiers, entered into a database, and their content then qualitatively reviewed for key word identifiers (open classification system approach). Grounded theory is then applied to further develop these text results into quantifiable metrics. These measurables include: variety of different responses, kinds of responses (reactive, proactive), patient initiated versus PCP-initiated, relationship of key words in responses to key words used in training, changes in medication type (Rx or not), history of medicines, mention of caffeinated beverages consumption, increase in recommendations made and entered into the medical records by PCP for reducing patient’s insomniac events, recommendations made for engaging in sleep diary activities, recommendations made for specific programs (visualization, etc.).
A reduction in the variety of clinical practices used by PCPs is expected, along with reduced non-insomnia medications and changes in OTC related products, increased notes in the medical records related to sleep diary events, and a reduction of uniquely applied therapeutic practices (reduced uses of specific forms of treatment by only 1 or 2 PCPs)
![]()
The methodology I used successfully around 2009 to successfully implement one of the first case-focused qualitative analytic methods for documenting changes in physician practice behaviors following attendance of a continuing medical education program. I used the most popular method to analyze the information provided by overseers of this new teaching plan designed to demonstrate long term clinical success attached to a CME program–grounded theory. This process required the application of two types of statistical approaches to review the overall success of the program.
The first review was a standard quantitative review of the pre and post-test information, provided in order to document the outcomes and success educational program using a fairly standard methodology that was already in place.
The second and third steps (b and c) require a combined qualitative-quantitative and a completely qualitative method implemented to review the outcomes. These two steps I engaged in use two totally different qualitative measurement activities. Whereas both methods focus on text content, meaning, and implications, the first required the additional use of grounded theory methods to analyze and then quantify the results of the pre-case/post-case process. The quantifier tool used for this method is semi-automated.
The last method of analysis required the use of a text content analysis tool for the open ended responses. It involved the use of a method for identifying key words repeatedly used to refer to the barriers physicians experienced with their clinical settings. The method I used was in quite similar to how I documented practice-related barriers to change. There are already a number of text content analysis tools out there. But in 2007 these tools were still in their initial stages of development with SPSS company technicians, programmers and other employees. By 2009 they had a preliminary version of this tool out there for public review at the special classes they gave, the first major successful tool generated by SPSS, but it only tested the text content for emotional content such as happy versus sad, complainant versus non-complainant, classes went too quickly versus too slow, etc. A few years later, in 2012, examples of this methodology were also seen being employed for analysis of comments generated by the social networking tool Twitter, using location of where the comments were generated to indicate if the text content probably pertained to a nearby consumer product provider being studied. The ‘tweeks’ generated via Twitter were analyzed for word content, and classified as either positive, negative or neutral. A simple manual review of these tweeks and their rating revealed that the vocabulary used to identify neutral responses resulted in the least correct ratings for that response. This didn’t disqualify the methodology from being used, it instead suggested that manual process or redefinition process be allowed if the size or number of the responses makes such a manual process applicable.
In the clinical setting, the terminology limits the use of this more generically applicable consumer analysis method. However, it does have applications, which like my version involving the insomnia study, benefits from having increased ability for the researcher to redefine some of the vocabulary used for metrics analysis–applying the supervised classification technique so to speak for it making it very much like a grounded theory project. For the physicians’ case studies example, this latter method can be employed, analyzed and then reported under the assumption that any improvements the program made in a clinician’s practice behaviors, according to his/her responses, also suggest where important barriers that once existed with these clinical settings prior to engagement in this 3-Tiered Education program.
This review process for an educational requires that some of the outcomes review processes be engaged in prior to the start of the educational portion of the program (pre-test be completed and 7-15 pre-case reports be filled out and handed in). After the educational portion is completed, the patient is allowed to return to the clinical practice setting and asked to over the next several weeks to few months keep track of cases that occur in the practice that related to the course topic at hand. For each of these cases, a standardized reporting form is used to avoid patient identification information from being shared, in compliance with related HIPAA requirements. This report consists of specific topics included on the form, meant to measure the amount of impact the program had on the various aspects of clinical performance. The types of information requested make use of totally open-responses with the header for each entry site requesting information on such things as primary diagnosis and specific illness-related diagnoses (the course topic), patient evaluation and history taking processes engaged in, intervention related activities that then ensue, and the therapeutic activities the clinician uses to deal with the particular problems at hand pertaining to the educational programs (Tier 1) topic(s).
The analysis steps require that each level (Tier) in this activity demonstrate some sort of relationships between the different measurement tools employed to analyze overall program outcomes at all three levels. Ideally, the pre-test should have questions that focus on what is expected to be covered by case reports, which in turn have entries that should be related to the follow-up responses on the program. Programs that demonstrate interrelationships between all 3 of these levels provide much stronger evidence suggesting that the program was a success.
Stage 1. To avoid planner/researcher-generated biasness from effecting the results, a blindness is introduced by allowing the analyst to engage primarily in a grounded theory based methodology for the second stage in this work. Likewise, the third phase in this work, the follow-up responses, can be analyzed by a third party or by the grounded theory analyst, but primarily approached as a topic-related barriers analysis methodology of analyzing responses.
The most important process in how to analyze the outcomes related to the grounded theory approach. This approach, by rule and methodology requirements, begins with a blinded approach to reviewing the data. In typical grounded theory studies, not all text content may become part of the data recorded for each entry made; in this case, due to the nature of the report–a case report asking for specific types of information–this use of the grounded theory method has some grouping of response types implied prior to performing the analysis and statistical review and so all text from the cases has to be entered.
Stage 2. Typical data entries pertain to: diagnosis, secondary diagnosis, reason for visit, medical history, clinical assessment, signs/symptoms, recommended interventions(patient-involved or not), patient education practices, therapeutics recommendations, prescription recommendations, and much of the above for primary comorbidities. The comorbidity, correlation information usually forms a major part of the QA program and includes topics that are typically noted or referred to during the education process for the illness; they are also often found and/or rediscovered as part of the first and second stage s of the grounded theory analysis. For examples: Diabetes-Hypertension and Obesity reviews, or Asthma Case Management-School/Home stressors, survey on living environment features.
The Grounded theory stage in the text analysis requires that all text responses be entered completely. Predefining some entry formats is a good step to take in this part of the data entry process, in order to complicated things later by prevent the need to evaluate text content for the use of abbreviations, medical shorthand responses, and such; this makes the data more capable of being analyzed fairly quickly.
Once the test is entered, it is analyzed quantitatively in the same fashion that many survey responses are analyzed. Total text response is evaluated (a word count), followed by counts of different sections of the responses signifying different types of responses (i.e. knowledge-based, clinical, therapeutic, by major type or subgroup and counts). Then each response line in the form is analyzed for the various measurable responses, categorized as above, with some changes made based upon needs for these reclasses defined during the second stage in the Grounded Theory analysis routine. This subgrouping of data constitutes step 2 in the Grounded Theory process.
Stage 3. The third stage of the grounded theory analysis assigns a value to each type/group of changes made. This is based on a predefined set of measures that have to be analyzed as part of the outcomes analysis procedure. Counts of individual who give particular responses, or counts of particular responses, or counts of a particular grouping of response types, can be statistically reviewed pre versus post. Presumably, an effective program will have certain parts of its teaching content appear more frequently once the program is completed. This pre- versus post response rates for these favored replies are counted, compared and then evaluated for statistical significance. This method quantifies data output generated using a grounded theory-derived, qualitative analysis technique.
To plan such an activity requiring three levels or three tiers, it is important that some 3-part/3-stage flowchart diagram be drawn up to demonstrate relationships between the test-response components for these of the three levels. The more lines there are connecting the boxes from Part 1 to Part 2, and from Part 2 to Part 3, the more congruity there is to the project as a whole. The best outcomes for this work require significant contacts be made between all three levels, beforehand if possible, but this may also be measured as a post-activity follow-up to decide how well the overall course fits this type of project need or requirement. The best programs will have a significant amount of interlinkage of these different components, for example one pre-test question linked to 3 out of 12 Tier 2 measures, linked in turn to 2 to 4 follow-up responses provided (Tier 3 responses=barrier notes). This measure can be duplicated for each initial question and then summed up, or linked a series of predefined goals linkable to the different part of the overall program, to determine overall success of the program.
.
.
The Next Step in Grounded Theory Approach.
In 2010, I entered the next stage in this manner of melding qualitative measurement techniques with the long-lived qualitative techniques. Late in 2010, I determined that this would have some of its better applications and proofs of success produce if it was applied to the study of cultural or ethnographic issues prevailing in some of the medical communities. My attention was drawn to this by the tendency for clinics to show preferences to certain visitor types by how they advertised their settings and where these advertisements were posted. Since these special facilities were in purportedly no different than the regional expectations, after all they had the same funding providers and identical expectations in terms of performance, I needed to come up with a way to in theory quantify their unique roles in these local communities. An individual from a community several miles away was not expected to go out of the way to partake in the special offerings of these clinics, whereas people who attended these very specialized clinics were in fact travelling a considerable distance to receive their care spoken in their native language, such as Russian, Vietnamese or Hispanic.
I first tried developing plans to measure cultural sensitivity for these clinics visually and in terms of educational materials, for example percent of documents owned and displayed in foreign languages, etc. This was a standard requirement already evaluated for some standard JCAHO metrics underway each year, why not apply it to the next level of cultural training documentation required by other Federal agencies?
In 2011, as part of the full review of disease classification I underwent due to the changing of ICD utilization plans from 9 to 10, I saw the need for using the new ICD stratification of diseases as a means to develop a much more valuable cultural medicine research plan. For the prior 10 years in Oregon, I had developed studies of this type for African Muslim, Modern Judaism, Laotian, Hmong, Cambodian, Native American, Inuit, Hispanic, Indigenous Hispanic, Hawaiian, Alaskan Maritime, Russian, Japanese, Filipino, Mainland versus non-Mainland Chinese, and Cuban/Caribbean population groups. Those studies focused on what made each of these groups different from the population at large, as well as each other. Naturally, the next time through I increased my reviews from focused mostly of culturally-bound and specific ICDs to intercultural ICDs and their demonstrated health and longevity linked differences. This work led to a number of unique findings that to this date seem to be unparalleled in their value and applicability to the development of better health care and preventive health focused ‘integrated health care’ programs, for lack of a better descriptive phrase.
My findings in the population health studies led me to conclude that we can produce much better combined qualitative-quantitative methods of measurement, by simply starting with the following quantitative review of age-gender population health findings.

Takotsubo vs. Factitious Disorder
Example 6. Actionable Follow-ups to Quantified Population Study results.
When we review the population of a group of people, there is an expected age-gender distribution of cases and an actual distribution that is often uncovered. Whenever we study a cultural group, we have to ask ourselves the following questions about the local communities:
- Is there an age range domination within this group, or, does the group consist mainly of elders? of young high risk children?
- Is the group primarily made up of young people in their earliest marital reproductive years?
- Does it contain mostly children who made their way here due to in-migration, or a local adoption agency?
- Are those who arrived all of the same religious, ethnic, sub-cultural, socioeconomic group and treated within as one group?
The above images/population pyramids depicting four age-gender distributions for four diagnoses comes from my Socioculturalism and Health page devoted to understanding and analyzing some of the most unique aspects of health care related demands and needs for different ethnic groups. It demonstrates the reason these latter questions have to be asked.
The results of the initial qualitative analysis illustrated above focused on four conditions commonly related to the culturally-linked (my term) syndrome of Takotsubo. Takotsubo has a very commonly cited physiological-anatomical (functional cardiac) theory for its existence. But the age-gender distributions demonstrate that the physiological-anatomical are probably false. The 429.83 Takotsubo syndrome is experienced mostly by Asian- or Filipino-descent Hawaiian families residing along the Pacific Rim; cardiomyopathy patients are distributed natinwide and have a very different age peak. Takotsubo does however compare with patients diagnosed with Factitious Disorders, a primarily psychological-psychiatric diagnoses that occurs mostly in elders, and like cardiomyopathy is most often diagnosed indiscriminantly across this country.
Takotsubo is a culturally-linked disease (my term), meaning it has a very specific and very highly related cultural affiliation thereby making the diagnosis most common with just people of this descent. Factitious disorders is a syndrome that was probably first identified as such, as its own behavioral diagnosis worthy of a distinct ICD, due to western medical traditions in combination with socially-defined expectations regarding the behavior of older people.
Takotsubo, on the left graph, displays a gender and age specificity that best matches which of the other three? Factitious Disorders of course. Yet, one of these is almost completely fictitious and culturally defined in nature, and the other strongly based on biological, anatomical and physiological claims to the diagnosed state.
The research questions posed here for use as an example of using Grounded theory and qualitative research techniques in general to address a modern day western medical quality of care question are as follows:
- how do the two ICDs compare with each other, first be age and then by gender?
- how does one quantify these qualitative relationships to see where the biggest differences and most significant differences exist? (hint, I designed a technique for quantifying the differences in pyramid shapes or forms, at one year age intervals–covered on other pages.)
- how do you prove to a clinical director or case manager that this is not a simple case of cardiomyopathy brought about by aging?
- how might you prove to a clinician in behavioral health or in cardiology qualitatively and then quantitatively that this is not simply a case of psychogenic cardiovascular disease?
- Next, to validate your claim that Takotshubo is possible a genetically-related cardiovascular disease predisposition complicated by cultural impacts, how do you develop a research and control group project designed to test out whether or not an anatomical-physiological finding has to be noted in the medical records for a true ICD to be attached to the Takotshubo disease?
- What is the best way to engage in this using qualitative research techniques–as a focus group study or as a case study? (Both are possible)
- Assuming one time you chose one path of research, and later another, what were the parameters that determined which way to go–focus group or case study?
- What are your initial metrics to be applied for testing your hypotheses?
.
The above example is based upon true results obtained from a population health based case review (n=millions+), so the age-gender pyramid data relationships are valid and reliable.
Physiological-anatomical diseases follow the general rule of gender equality. Only specific ICDs demonstrate differences across genders when it comes to a condition or disease that is totally anatomical and physiological in origins, nature and clinical manifestations. Some disease demonstrate cultural impacts on the differences in gender distribution over years or ages. These suggest there is some form of culturally related psychosomatic effects ensuing with the condition, such as gender linked expectations related stress, or in fewer cases, gender-linked physiological differences due to different gender linked morphologies and chemistry (i.e. the shape of the body/organs, or the impacts of steroids on the physique and disease manifestation.) Usually, physiological-anatomical diseases, when they demonstrate a distribution as balanced as that of the above displayed cardiomyopathy, are due to changes in form, physique, functionality that are genderwise indiscriminate. This is usually why cardiomyopathy is unexpected as the sole cause for the deaths in women more often than men in such cultural settings with elder-linked heart disease induced deaths.
Psychogenic disorders are still possible here, but tend to prefer younger people in terms of prevalence and incidence. Such is opposite for Takotsubo, thereby ruling this option out. Notice also the changes in gender preference with aging, with young men more likely to be diagnosed for such when the population is in its twenties and thirties, versus women in the older years of life, with a gender ration F:M rates similar to those of Takotsubo and Factitious disorder. If your base population was just elders, this diagnosis would probably also surface in the differential diagnosis algorithm. Notice how in such a case, knowing which of these three old-age complications in life is most likely the case for a patient, will determine the diagnostic and prescription drug parts of the regimen that are engaged in. A simple case of psychogenic cardiovascular disease is indeed treated much differently from a age-related Factitious problem or a culturally-linked physical-emotional Takotsubo patient. For the first two, American medicine suffices. For the last of the three possible conditions, culturally sensitive treatment protocols need to be adhered to.

Uppermost layer=Takotsubo and Fictitious Disorder noted in same settings,
Middle layer=Takotsubo only,
Lower layer=base map with Fictitious Disorder afflicted regions (barely visible)
.
FOR MORE ON THIS INTEGRATED QUALITATIVE-QUANTITATIVE APPROACH TO MANAGED CARE PROGRAMS AND THE DEVELOPMENT OF MORE COST EFFECTIVE CULTURAL, SOCIOECONOMIC STATUS ‘QUALITY OF CARE’ PROGRAMS, GO TO THE FOLLOWING PAGES . . .
Combined Qualitative-Quantitative Research Methods – Part 2
AND
