
Introduction
“Changes of Types of Diseases” is a term that refers directly to the modern epidemiological concepts of epidemiological transition and my rendering of the sequent occupancy related review of changes in living patterns, occupations, culture, etc. and ultimately the changes in disease patterns that ensue due to these lifestyle changes. Although easy to understand, it is a fairly detailed concept that in history is sometimes hard to delineate a chronology for. This is because of the changes in disease philosophy and terms over time. I can look at disease writings in retrospect and better understand this philosophy based on prior readings, than try to understand it by reading the new philosophies as we progress through medical history ending up the the recent to modern stages in medical history.
The evolution of this concept of changes in diseases over time has several things influencing its change. The changes in disease philosophy and reasoning over time naturally make it difficult to relate one generation of beliefs with those practiced two or three decades later. It is hard to compare anything that developed pertaining to “changes in disease types” for example between the writings of New York Doctor Samuel Mitchell, and German disease geographers Schnurrer, Berghaus and nosologist Friedrich Canstatt, and England’s William Farr, John Snow, and William Aitken. Yet it helps to be able to do this comparison in order to better understand disease mapping.
There are two way to look at the changes in disease type theory. The first is to consider disease change as a product of the ways in which we change our interactions with one another, such us between the diseased person and the people at large and the diseased person and how he/she interacts with the earth. This combined sociological-anthropological-physiographic interpretation is used to explain natural science differences around the world, such as why certain parts of the world have certain diseases and others do not, or why certain groups of people have differing susceptibilities to disease in general, versus others who seem to never get ill in certain circumstances.
The second way to interpret the disease type theory of the past is to add it to the ongoing debate out there about religions versus science. Religious leaders might interpret a change in major epidemic disease forms to be a consequence of both God’s ongoing lesson to humanity, modified by how humanity changes its interaction with God’s environment. New forms of interaction mean new versions of older lessons are being developed. Whereas scientists state that these new lessons are a consequence of our ability to see more precisely all that nature comprises, and along the way changing some of this former wilderness and natural habitat into a manmade living space, at times interacting too much with the older version it once was still remaining in some underdeveloped regions on earth, traditional religiously minded fatalists state that disease is a consequence of our inheritance and responsibility pre-ordained to us by some higher power.
This way of interpreting disease culturally assigns cause to ourselves, not nature. We are passivists at the hands of a higher decision maker. Were such truly the case, then there not even a reason then to question the implied statement telling us we cannot move to new regions, take over different parts of the world than where we originally lived. This is obviously the results of a mindset not thoroughly thought through. Anti-evolution is a movement that is only superficial in its ways of looking at “God’s Gifts” to us. ‘Changes of Types of Diseases’ indicate that nature is at play, not only some higher power, and that nature is making most of the decisions, not us and the way we migrate about the earth’s surface.
This latter philosophy prevailed beginning in the second quarter of the 19th century when Charles Mason Good put out his very naturalistic interpretation of the world and its environments, with and without man. Even though Good’s work in today’s sense seemed a bit too generic and simple in nature, over-exaggerated in terms of its depth in meaning, it was still important to the field of sciences and medicine because Good was brilliant in that he pulled the various natural sciences findings back into a single writing, a very Humboldtian way of interpreting nature, with or without its being a result of God in mind. Much of Good’s writing served as a bridge between the simplistic interpretations of nature in the first decade of the 1800s and the complex, very specific forms of science nature became by the time the 1840s were reached.
Also during this time we find the works of Erasmus Darwin reaching their peak in use and presentation, making way for Erasmus’s grandson Charles to take the stage with his evolution-selection based theory by 1850-1855. Prior to Charles Darwin’s teachings and parallel to Erasmus’s teachings were the teachings of Lamarck, and the concept that nature’s stresses, natural selection processes, and the ability of organisms to learn from these experiences and adapt to them subconsciously and physically, without knowledge such a process is taking place, resulting in a smarter more fitting family of children produced as a result fo this stress. In many ways, Haughton’s “Changes of Types of Disease Theory” fits the Lamarckian paradigm of time and changes, learning and adaptation, in a very sensible way. Like a giraffe growing a longer neck due to the need to indulge on taller trees for foodstuffs, we either develop changes in our body to adapt to the new environments we move into and have to adapt to, or we develop diseases due this lack of adaptability.
Our constitution, inheritance, temperament, and other very internal, somatic and mental traits make us who we are and what we will become by moving to some new location, new place or residency. This philosophy also enables us to understand why some of us who do move into a new place can tolerate this change in living place and still survive and then adapt, whereas other people with other constitutions cannot adapt or get better within the next one or two generations of descendants. When we compare this with the philosophy of 1800, we find the most significant change to be the transition of how we fight disease from a fairly non-biological passive process to a very self-engaged scientific and naturalistic, biological process.
In 1800, a fatalistic interpretation was made about disease and the cold for example. To live healthier, we had to grow sheep to produce warmer woolen clothing, and continue to produce our traditional foodstuffs that we have become so used to. These were the thoughts of Samuel Mitchell and the Livingstons when they removed from the urban setting out into the wilderness of New York just north of the city. By 1850, we have learned more about the environment, and can now determine when and why we don’t have to be so non-engaged with nature’s stresses placed upon our bodies. Whereas from 1800 to 1825, if you got a terrible disease and decided to move south to avoid its causes for exacerbation or return, in contrast to simply buying and wearing new clothes that are warmer, a quarter century later, between 1825 and 1850, you learned you had to move to another region for other reasons–certain kinds of diseases require specific conditions for specific problems. You learned to be prepared for exposure to other illnesses in that setting, but you moved there anyway in order to get better. Extending life and longevity became your primary goal.
Changes in types of diseases is also a concept that ultimately relates very well to Benjamin Rush’s changes in styles of living and occupations discussed in Manchester, England in 1786/7. These two ideologies are 80 years apart, and not intertwined together as much as they should have been. Haughton’s thoughts have come up before in medicine, and each time were only taken in consideration for brief periods of time. Today, we can use this logic to come up with the notion of disease evolution as it relates to environmental and ecological changes. The notion that an E. coli bacterium can obtain the genetic make up required to become the seriously pathogenic and fatal illness it is once it inherits shigellatoxin or choleratoxin is an example of this. Sequent occupancy theory tells us this is a more recent example of the major changes that took place a century or two ago. Changes in disease types progress from the outer world to the inner world, from the macrocosmic level of interpretation to the microcosmic level, from the environment and ecology involving man, domestic animals, occupation types and living space, on down to what we eat, what we make contact with that is minutia.
So, Haughton’s article is helpful to read and learn from for several reasons. It gives us insights into how we use logic to construct, deconstruct, and again later reconstruct and promote particular theories in health and disease. A very early writer and physician who led in the development of this philosophy, Sydenham, claimed that the most common epidemic disease patterns for the time, fevers, underwent this change in type behavior. Sydenham’s way of classifying diseases differentiated cyclic and recurring from continuous or constant raises in in body temperature. He went further by focusing on the cycles that recurring diseases had, twice a day, thrice a day, etc., and then added those kinds of cases that also had chills intertwines with those periods of hotness. Such a philosophy later allowed others to differentiate fever into even more subgroups, those that were bilious in nature, those that were specifically yellow and bilious and deadly, those that produced a black skin and deeply sunken eyes just before death, those which made use tremble and seem overly excited, nervous, and expending our last vital energies in the minutes or hours before the final collapse.
Without any knowledge of disease and its causes, just the focus on its symptoms and presentation, we were able to differentiate the typhus from the malaria, and later the true typhoid of warmer settings from the more ubiquitous wintertime typhus. The “mal aere” generated disease patterns separated into remittent and intermittent fevers and ague (the true malaria of today). With such a differentiation, we were able to see the regional geographic differences between bilious fever and yellow fever, and learn to separate the very deadly yellow fever from its similars, and the very deadly Asiatic or malignant cholera from the less deadly cholera morbus and cholera infantum. Then it was up to our improved understanding of anatomy and physiology to help us further differentiate diseases into the subtypes, or “Changes in Types.” seen over time.
Haughton’s “Changes of Types” is really a sequent occupancy idea in disguise. As the development of an area led to changes in land use and populations, it became a popular belief that as we migrated to new places, built new dwellings, developed new hamlets and ultimately gave rise to big towns and cities, that disease changes would be the ultimate consequence of this building of new empires. It was the physicians’ responsibility to understand this concept so he/she could compare for the future when removing to a new region to practice medicine. This is why “Changes in Type” is a concept that comes up time and time again in the early medical geography writings of ca. 1680 to 1890. In 1891, with the “discovery of the germ or bacterium as the cause”, came a changes in type philosophy that focused on the organism and its victims, animal or man, not the place and climate needed for the consequences of a poisoning or infection to ensue.
.

The other way a few medical geographers looked at disease type was its relationship to altitude and the magnetic poles. With this philosophy, there could be a transition in disease patterns over space from south to north, with diseases changing types by major latitude change, and major forms (system they present in) via temperature region changes. A few interpolar defferences in disease types may be explained this way. But this logic was used extensive to explain how a disease from the south migrates in what appear to be cycles to the other latitude regions. Magnetic fields cycle and fluctuate high and low, leading some to speculate this was the cause. This philosophy came from an associate of Haughton, Robert Lawson, who was well supported by Haughton at the time this article was published.
.
ARTICLE
.
The American Journal of the Medical Sciences, Volume 52. Oct. 1866. Pages 389-396. [LINK]
Art. IX.—On the Changes of Type of Diseases. By R. E. Haughton, M. D., of Richmond, Ind.
Change is written on all things temporal. If we look back but a few years, we shall find that very remarkable changes have taken place in the history of disease and its treatment—that the forms of disease which were called sthenic, attended as they were by a high grade of arterial excitement, are now superseded by the asthenic forms, in which all the symptoms are modified by a strong tendency to general debility from the very commencement of disease. By the sthenic condition is understood the inflammatory reaction or excitement, attended by a burning skin, injected eyes, intense headache, flushed face, wild delirium, and throbbing pulse; in which conditions the physicians of former days used the lancet freely till relief was obtained. This condition has been replaced by the asthenic, which has manifested itself more fully since the advent of cholera in this country— 1832, 1853. In this asthenic type of disease, debility of the heart’s action appears from the first, and often requires active stimulation to support the patient, conjoined with nutrients. This is no delusion. Why is this remarkable change, and do such changes present themselves to us in our visits to the bedside? The history of medicine in the past fifty years affords ample evidence that medical opinion and practice have passed through radical changes, and that the treatment of disease, as we see it to-day, is vastly different from what it was at the former period.
Contrary to this view, however, Dr. John Hughes Bennett, of Edinburgh, in a work entitled ” Clinical Lectures on the Principles and Practice of Medicine,” declares that the diminished employment of blood-letting and other antiphlogistic remedies of late years does not arise from a change in the type of disease; but that the present advanced state of pathology and diagnosis has proved the former treatment to be erroneous; and he therefore concludes that inflammation is the same now that it was in former years. That antiphlogistic treatment is not used to the same extent, or is hardly used at all in the forms of disease of to-day, is not controverted; and that the indications we find most generally do not demand its use, is quite as well established. That medical men of to-day treat fevers and inflammations by agencies which they had never thought to use thirty and forty years ago, and are still the successful physicians they were, is not to be doubted, and it seems to me that were we to deplete the diseases of this day as was done formerly, we should lose many more of our patients; proving so far that depletiou could not be borne now as it was then. To sustain the proposition of a change in the types of disease it is only necessary to examine the history of disease in our country during the various cycles of the last half century.
In looking back as far as 1807, and from that time to 1820, we find an epidemic of typhus fever prevailing, often complicated by pneumonia, which Dr. Wood says was erroneously called pneumonia typhoides, as it was a complication of epidemic typhus fever. The treatment, both in fevers and inflammations was at the time of the irruption of the typhous epidemics decidedly antiphlogistic; yet when a change occurred in the type of the disease as it did in 1812-13, the consequences of such treatment were fatal. In Philadelphia the celebrated Dr. Parrish, a young man, at that time, saw these unfortunate results of treatment, and treated the epidemic by active stimulation and support, and with the result of saving nearly all his cases. “So fatal was the treatment by copious bleeding that professional as well as popular opinion received a set against it.” (Dr. Wood.)
Here at once was a decided change in treatment, corresponding to the type of disease which had most evidently changed from the more sthenic and prevailing types to one most decidedly asthenic, and which modified all the then prevailing forms of disease. The history of the various typhous epidemics shows that typhoid and not typhus fever has been the prevailing fever of the New England States, and though not confined to such geographical limits, that fever was not known in the Western States. The malarious types of fever were alone known in the early settlement of the country, except only isolated cases of typhoid fever occurring in persons who had come from the East. For twenty years back, epidemics of typhoid fever have prevailed over large districts in the West with considerable severity, but a diminishing mortality. When I commenced practice, in 1850, the first epidemic of typhoid fever was prevailing in a certain locality in Indiana, and since that time I have seen three epidemics of the same disease. Malarious fevers also prevail to a certain extent every year; bilious fever being regarded the common type of fever in the autumn. As time has passed on, bilious fever has become rare in the same region, and intermittent fever as well as remittent, when they occur, are influenced by some depressing agency, which sometimes converts a truly periodical fever into a continued form. An opinion consequently prevails that typhoid fever has a tendency to replace intermittents and remittents, as these diseases are growing more unfrequent, and typhoid fever is now in many places in the West the predominant fever. Here we have a blending of types presented to us, beginning as malarial and ending in typhoid; to such blendings of types Dr. Woodward has given the name of typho-malarial, which exactly expresses what we observe in the history of such cases. Dr. Austin Flint, now of New York city, says:—
“That typhoid fever has to a great extent superseded the remittent form, and in a brief enumeration of the distinctive traits of remittent, typhus, and typhoid, published by us in this journal [Buffalo Med.’], we mentioned this as a sentiment generally entertained by the profession in this region.” He says further: “We think there cannot be a doubt that a striking change has taken place within a few years past, and that typhoid fever from having been, to say the least, of unfrequent occurrence, has become frequent, and is becoming more so, remittents diminishing in frequency after the same ratio.”
These views are corroborated by some conclusions to which M. Boudin has arrived more recently. He says “there exists an antagonism between typhoid fever on the one hand and intermittent fever and phthisis on the other.” In the ten years which are past, and in which we have been presented with an ever-varying succession of disease, the typhous element seems to have predominated, and to control both the inflammatory and febrile types of disease, complicated, as these last frequently are, by some local inflammation, in all of which prostration is the common attendant. Since the advent of epidemic cholera in 1832, up to the present time, we have had conditions in disease which forbid the treatment so commonly resorted to prior to that period. Before 1832 the antiphlogistic treatment was practised; but soon afterwards cathartics were found to produce great disturbance where formerly they were used with benefit; and even to this day they are not nearly so ranch needed, nor even indicated, except those of the very mildest kinds. Intestinal mucous irritation is set up as the result of such practice, and prostration soon manifests itself. Blood-letting is abandoned, except by men who are averse to improvement, and who shut their eyes to the results of a more enlightened experience, based upon the changes in the types of disease. Another proof of the changes in the types of disease is afforded by some of our epidemics during the last five years. We have had, since 1860, an epidemic of diphtheria, and to some extent of erysipelas, also cerebro-spinal meningitis or cerebro-spinal fever, which we have found exhibiting evidences of prostration; and the last disease I have seen begin as cerebro-spinal in all its manifestations, and terminate in well-marked typhoid fever; the spinal and inflammatory symptoms subsiding, and the patient recovering slowly, as from typhoid fever. There was the same redness of tongue, the tender and tympanitic abdomen, the diarrrhoea and rose-coloured spots of typhoid fever, not those of spotted fever so-called. Dr. Pierce, of Mechanicsburg, Ohio, in a paper published in the Lancet and Observer, in speaking of an epidemic of typhus, typhoid, and cerebro-spinal fever occurring in his community, discusses the community of their origin and identity of character. I have no doubt of the truth of his observations, as I know very well in this region also that cerebro-spinal fever frequently merges into a genuine typhoid fever, and I believe that there is a community of origin, cause and effect, bearing their true relations in these three forms of disease, capable of being converted from one into the other, or, in other words, convertible forms of disease. It is true that with us we do not see the genuine typhus, as described by British writers; but it is believed that cerebro-spinal fever is a modification of the genuine typhus, and we have typhous manifestations which are known to belong to the group of typhous diseases. Dr. Kersey, writing on the same subject, says, “of cases he had seen, reproducing, in almost every feature, the mental impression made a quarter of a century ago by watching the progress of a few cases of typhus or ship fever.” These are not sthenic but asthenic diseases, and require a very different treatment from what was used when disease presented high arterial excitement. According to Dr. Hughes Bennett, who maintains that inflammation is always the same, the changes presented when disease is left to run its course undisturbed cannot be explained, for cases then recovered under the treatment which if applied now would prove certainly fatal in a large majority of cases. This is accepted as a fact, and I am disposed to think that there is another element not sufficiently taken into account. The force of the circulation has been carefully estimated in sthenic and asthenic diseases. But, if inflammation is always the same, why do we ind now such complete prostration attendant, if the causes, conditions, and elements which enter into it under all circumstances are precisely the same. In the sthenic forms, when bleeding and purging were freely practised, such rapid and overwhelming debility did not occur as do now, when we have asthenic forms of disease. The reason for such differences is, I think, to be found in the influence which the nervous system exerts upon the type of the disease and its force. .All diseases, except traumatic ones and those produced by poisons, have their first lesion in the nervous system. Lesion of enervation, as Dr. Southwood Smith wrote, so I regard the first lesion as that of the nervous system, and as the agency, or poison, or whatever it may be, which produces disease, may exert more energy or power in one case, so we may have the ever-varying conditions of sthenic or asthenic impressed by the vital forces as they are influenced by a more or less violent and depressing cause. Lesion of circulation, lesion of nutrition and secretion next in their relations are disturbed, and there occurs just what we are witnessing as the epidemics come and depart. The testimony of morbid anatomy is adduced by Prof. Stokes, who says:—
“Having had full opportunity of seeing and examining the recent examples of diseased structure, amounting to nearly 3,000 specimens, the products of the various hospitals of this city (Dublin), and this result is remarkable that the specimens of acute disease have had a very different character from that commonly met with in Dublin, between 1820 and 1830. As a general rule, these specimens all showed appearances indicative of a less degree, of pathologic energy.”
This is sufficiently full to indicate changes in the vital conditions which influence the type of disease. Disease is but a condition of tissues, a departure from their physiological state, and there is some rule which acts, not only to develop but to control, that tissue in its departure from its normal standard. Now either the vital endowments of the tissues are changed, or there would be no change in the tissues examined after death, if the varied influences which operate to produce and change disease were the same as observed under the sthenic types. But these vital endowments are changed, and the pathologic changes are not the same. In asthenic inflammations, the effusions were often copious and hemorrhagic; the inflamed surface of the tissue highly reddened; while now in pneumonia, as I saw in a recent case, the lung was of a purple or livid colour, not red, the effused lymph a grayish pasty mass, forming weak adhesions to adjacent surfaces; in other places, owing to the feeble energy of the inflammation, the effused products were in a pulpy or semi-fluid condition, having a strong tendency to form pus. This was in a case of pneumonia, evidently of the asthenic form, in which, by vigorous stimulation and support, I could not change the inflammation or its results. The same story is true of serous membranes. The firm bands of adhesion which used to be met with in pleurisy, in the peritoneum and other serous tissues, are not found now, but in their place are seen serous or bloody effusions; the lymph which was deposited does not become organized, but is thin and somewhat transparent, and collected into the serous cavities, thus producing embarrassing accumulations of fluid, with no tendency to be removed, but increasing as the disease progresses, impairing the vital tone of the patient. As Dr. Stokes says again, serous, or sero-fibrinous effusions tinged with coloring matter, replaces the old results of sthenic inflammations, and tallies exactly with the change in the vital character of the disease. Now let us look at the results of practice and the influence of remedial agencies under the conditions of disease, and see if there is not something which influences the same results. Formerly, when the more sthenic forms of disease prevailed in the country, blood-letting, cathartics, emetics, nauseants, and a system of starvation having a decidedly reducing effects, were followed in the treatment of fevers and inflammations, and there were no alarming symptoms; but after a long, protracted sickness, slow convalescence was eventually established. This was regarded as success, and the patient as eminently fortunate. At various periods of time, we have seen less and less of the sthenic types of disease, and as far back as 1842, the typhous element, the zymotic causes of disease began to invade the Western and Southwestern States, and the periodical fevers and inflammations governed by the influence of a periodical law, were gradually displaced by a type of adynamic fever, and the inflammations when they occurred, either as original diseases or as complications of the fevers, were not influenced or successfully treated as disease had been before. Quinia, which was known as the great agent in the cure of periodic fevers, did not cut short or benefit these diseases, but was often positively pernicious; mercury was seldom required, though often used to the serious detriment of the patient Purgations sometimes induced an early prostration, as did also tartrate of antimony, as used in the typhoid pneumonia. Sometimes in the early stages of these cases, the depleting plan was resorted to; but when prostration was observed, the whole plan was changed to stimulating and supporting—often too late for success. The idea of change of type did not, I conceive, influence the minds of the profession sufficiently to lead them to estimate the vital forces as acted on by a zymotic poison, absolutely depressing in its influence on all. This, as well as not knowing the full value of remedies, in their proper time and place, was a great defect.
The first epidemics of typhoid fever aud typhoid pneumonia were very fatal, in many localities in the West; but experience has improved, and the influences which operate to produce certain forms of disease being better known, treatment is more successful than formerly. These important changes are not due to an improved pathology, but changes of treatment, necessitated by the changes in the type of disease. As evidence of the change which the type of fever undergoes, Dr. Tweedie’s report for the year 1845 shows the low form of disease by the large quantity of stimulants demanded. “he states, that in the epidemic of 1843, when eleven hundred patients were admitted into the Loudon Fever Hospital, the quantity of wine administered was about eighteen hundred ounces, and sixty ounces of brandy, while the next year, not half the number were admitted, and they consumed fourteen hundred ounces of wine and seventy-six ounces of brandy, besides other stimulants.”
This evidence goes far to show that medical men had observed the change, and were acting upon that knowledge; and that, also, this change of type did not belong to the Western World, but had been observed in Europe. Now Dr. Bennett declares that the diminished employment of bloodletting and other antiphlogistic remedies, of late years, does not arise from a change of type, as supposed by Drs. Allison, Christison, Watson, Stokes, and many of the profession, but that the present advanced state of pathology and diagnosis has proved the former treatment to be opposed to a sound pathology. This proposition does not explain the fact that men scattered over the Western States, isolated as they often are, have not improved their knowledge of inflammations and the treatment of them, until the failure of remedies aroused them to the necessity of a change in the treatment, to meet the existing conditions of disease. We admit progress, but not in the same sense with Dr. Bennett. Dr. Parrish was not a generation ahead of his contemporaries, when he adopted the stimulant plan of treatment in the epidemic typhus of Philadelphia in 1812 and 1813. It was not his superior knowledge of the forces of disease, but the observation of facts, combined with tact, which built for him a reputation. So it has ever been with medical men. The recognition of a medical fact and its adoption leads to success, where failure stood in the way before. This is the progress which medicine has made through past years, and each successive generation becomes the depositories of the experience of the past for the benefit of the future. To be satisfied that changes in the types of disease do occur, we have access to all the sources of evidence, as to the nature of disease by its study in the past, as well as the present, and in the pathological changes observed after death, and in the effects of therapeutic agencies. We may further quote the evidence of eminent medical men upon this question.
Dr. Watson says: “I am firmly persuaded by my own observations, and by the records of medicine, that there are waves of time, through which the sthenic and asthenic characters of disease prevail in succession, and that we are at present living in one of its adynamic phases.” Dr. Stokes says, after summing up all the sources of evidence upon the nature of disease: “Looking at the question from any one of the sources of evidence, we come to the conclusion that the doctrine of a change of type is a true one, while if we take all the facts, and observe how they point to the same conclusion, we must, to use the words of Dr. Alison, ‘Accept the change of type as an ultimate fact in the history of diseases.'” It seems to be true, that of the very many causes of disease which I have no doubt have power to develop new forms or types, of which we may have had but little or no experience, that they travel from one portion of the earth to another, and generally from east to west, around the world, but simply proves what Dr. Watson has said, that there are waves of time, and I had like to have added periodic time, in which different types of disease prevail. These causes are evidently capable of inducing disease, and of influencing the character and type of disease, so that all forms of disease exhibit a certain degree of conformity to a controlling law, which is the law of the epidemic disease. “Dr. Robert Lawson, from investigations which are published, deduces a law, showing that a series of causes originate, or become apparent in the southern hemisphere, and travel northward with much regularity.” This influence he designates more properly ” pandemic” than “epidemic,” and in conformity again with the language of Dr. Watson, “he calls these successive waves pandemic waves.” Waves of disease upon the waves of time, and there is no doubt that very wide and radical changes have been presented in the successive waves of disease, from the higher and more active types to the lower or more adynamic types. Again, the same writer says: “These casual eruptions of new forms of disease have always taken place during the passage of a pandemic wave, and therefore concludes that this cause determines the occurrence of disease where it passes, while the forms or types are influenced by the meteorological, malarial-hygienic or social conditions of the population. He admits, however, that the facts of disease lead to the conclusion that the epidemic or pandemic cause can determine the resulting form or type of disease, though local and temporary causes may determine a different form yet impressed by the great law of epidemic influence.” So it has been in the diseases of endemic origin; they are impressed by a more powerful law, and show its existence throughout all its phases. We might adduce more evidence were it needed upon this question, and we now simply say that we have travelled over all the sources of evidence, no doubt in an imperfect manner, yet it seems to us with sufficient bearing, upon the question at issue. I regard the acceptance of the facts in this paper as necessary to the proper comprehension of diseases of this era.
[Dr. Frederick J. Brown, of Rochester, Eng., in a letter to the Editor of the Medical Times and Gazette (Aug. 4, 1866), gives the following as “an unanswerable argument” in favour of change of type:—
“Let me say that country labourers that used to be bled every spring thirty years since found themselves a few years later fainting after four ounces, whilst they formerly could lose sixteen ounces and walk miles without any sign of faintness. These are cases of people in health: therefore they are free from the fashions of sickness—treatment. The younger relatives and neighbours of these countrymen were similarly affected by bleedings: therefore it was not a case of men growing older and not tolerating bleeding from that cause.”
Connected as we have been with the profession for half a century, we can testify from personal observation as to the change in type which diseases have undergone within that period; and of those who remain of our early contemporaries, we have not conversed with one who has not concurred with us as to this fact.—Editor.]
.
.
NOTES
Biography [Pulled from http://countyhistory.org/books/doc.fayet/477.htm. Accessed on March 22, 2013]
Richard E. Haughton, M.D. Dr. Richard E. Haughton, who for forty-five years has been actively engaged in medical practice in Indiana, is one of the most talented members of his profession in the state, and has, perhaps, done as much to elevate the standard of medical excellence therein as any other man. Being of broad and liberal mind, and having enjoyed the advantages of a superior education, he has had the interests of the people deeply at heart, and has keenly felt how completely they are at the mercy of the medical practitioner, who, but a few years ago, before the present rigid regulations were put into operation, was often the most veritable charlatan, plying his arts to the jeopardy of his misguided patients. By pen and speech Dr. Haughton has used his influence for many decades in the advocacy of higher education and training for physicians, and the limitation of their once almost absolute power over the lives of their patients. He has always stood boldly forth as the champion of progress, and his wonderful influence has been exerted at all times on the side of right and truth.
A son of William and Sarah (Johnson) Haughton, the Doctor traces his ancestry, along both lines, to old English nobility. On the paternal side he is descended from Sir Wilfred Haughton, a baronet of the seventeenth century, and many of his ancestors achieved distinction in the business and professional world and as statesmen and authors. One of the eminent representatives of the family at the present day is Rev. Dr. Samuel Haughton, of Trinity College, Dublin, Ireland. The maternal ancestor of our subject was a nobleman at the court of James I, of England, and his descendants were among the first colonists of Virginia. They were wealthy landholders and slave-owners for some time, but, being associated with the Friends, they came to abhor the principle of human slavery and eventually manumitted their slaves.
William Haughton was born in Carlow, county of Carlow, Ireland, about forty miles from Dublin, in 1804. He was partially educated in Ackworth boarding school, in England, and in 1822 he set out to make his fortune in the United States. At first he located in Fayette County, Indiana, and subsequently removed to Union County, same state. Here for forty-five years he was known as an educator, one of the ablest in the state, and though he taught for several years in the old-time log school house, he later was connected with some of the leading educational institutions of Indiana at that day. For over a score of years he was a preceptor in Beech Grove Seminary, having under his charge young men from all parts of the country, some twenty states being thus represented. He was principal in the Union County Seminary and thereafter he became a member of the faculty of Earlham College, where he continued actively engaged in his beloved work of instructing the young, until, by reason of failing health, he was compelled to resign his position. When he had rested from his labors for a period at Knightstown, Indiana, he could not resist a resumption of his former work, when he was tendered a position as principal in the high school there, and death found him at his post. He died in July, 1878, of paralysis, aged seventy-six years. A birthright member of the Friends’ Church, he was a preacher in that sect for a number of years, his life being a consistent and beautiful example of the doctrines to which he was reared. His devoted wife survived him, dying in 1882, when four-score years of age. He had but two children, Richard E., and Mrs. Lucy White, of Texas.
The birth of Dr. R. E. Haughton occurred in Fayette County, Indiana, December 8, 1827. He found an able friend, companion and instructor in his father and at an early age was remarkably proficient in mathematics, science and literature. When a youth of fifteen he rendered his father excellent service as assistant teacher, and from 1845 to 1849 he devoted a portion of each year to the cultivation and management of his father’s farm, helping to pay for the property. In the fall of the year last named, he commenced medical studies with their family physician, but, his father having been called to Richmond, the young man took his place in the Union County Seminary. In 1853, however, he was graduated at the head of his class, with the degree of Doctor of Medicine, in the Cleveland Medical College, where he had pursued the prescribed course of study. For a short time prior to his graduation he had practiced at Knightstown, with a partner, and he now returned, and until October, 1855, he remained in that place. Thereafter he practiced in Richmond for a score of years, meeting with exceptional and merited success.
In the autumn of 1873, Dr. Haughton was urged to accept the chair of descriptive and surgical anatomy in the Indiana Medical College, at Indianapolis, after which he was professor of physiology and physiological anatomy in the College of Physicians and Surgeons, in the same city, for a period of four years. In the summer of 1879 he witnessed the fulfillment of a long cherished desire — the establishment of a new college, which should occupy a much higher plane than any of its predecessors. Thus, largely owing to his influence and zeal, the Central College of Physicians and Surgeons was founded in the capital city of the state. This institution was the first one of the kind in the west to require students to pass a general examination ere they were admitted, and the numerous restrictions and regulations which were put in force have proved a safeguard and benefit to the college, whose graduates are proud of their alma mater, in consequence.
A ready, clear and comprehensive writer, Dr. Haughton has wielded his pen for years on a variety of subjects. A valued contributor to the leading medical journals of the day, his articles on the diseases of the nervous system and on surgery (in which department he is especially expert) have been widely copied. Desiring to further qualify himself in special lines, he took a post-graduate course in Jefferson Medical College a few years ago. Since 1859 he has been a member of the American Medical Association, and is identified with the Indiana State Medical and the Tri-state Medical Association (of Indiana, Illinois and Kentucky). He is an honorary member of the Ohio State Medical Association, and belongs to the societies of Wayne, Marion and Union counties. He assisted to organize the Wayne County Medical Society and that of Union District. Since 1895 the Doctor has again been engaged in practice in Richmond, many of his old patients returning to him, and others, who have known him by reputation, have been glad to retain him as their family physician. He takes great interest in local affairs, and was one of the projectors and original stockholders in the Richmond Street Railroad Company.
In his religious views the Doctor is liberal and independent, as might be expected of one who has been a deep student and has had wide experience. Though he was reared in the Society of Friends, and has the most genuine esteem for that body, he prefers no other guide or rule of conduct than what he finds in the Scriptures, and is opposed to ritualism and formality in worship. After four years’ special study of religion, he was ordained a minister in the Methodist Episcopal Church, in 1898, though for two-score years he has preached the gospel of Christ, and from his boyhood he has endeavored to lead the life of a Christian.
In the First Presbyterian Church of East Cleveland, Ohio, on the 13th of February, 1853, a marriage ceremony was performed which united the destinies of Dr. Haughton and Miss Catherine Meeker. She died December 20, 1867, and left two children: Edward Everett, who is engaged in the real estate and insurance business in Chicago; and Louanna. The present wife of the Doctor was Miss Elizabeth Mather, a pupil of Earlham College, and a lineal descendant of the famous preacher, Rev. Dr. Cotton Mather. She is an earnest Christian worker and has been for years connected with the Woman’s Christian Temperance Union as a national evangelist.
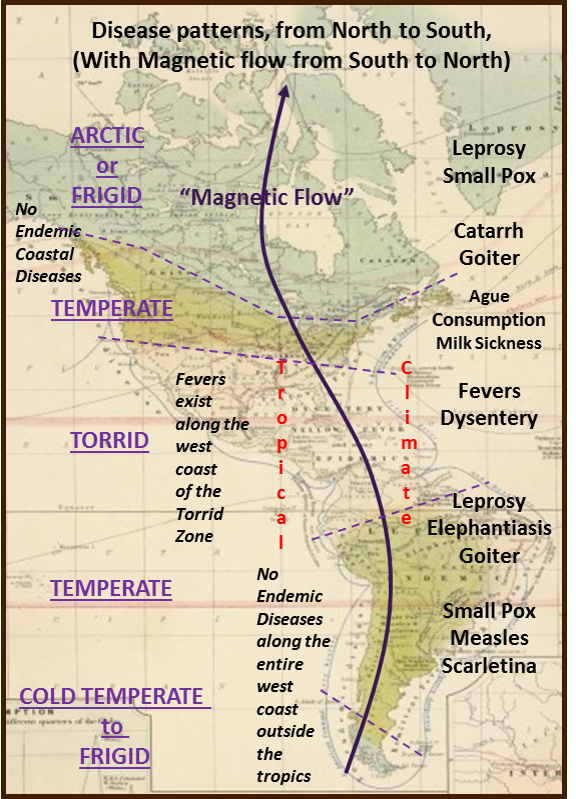
This same change in type based on latitudes for the other hemisphere. A review of diseases for the Americas showed that diseases to the north were far worse than those to the south. The magnetic fields theory could be used to explain this difference as well.

Leave a comment