
Introduction
E979 is the code entered into medical records when terrorism or bioterrorism is part of the patient’s story. This code is actually older than the actual events that took place in this country that may be registered as bioterrorism, if we exclude the earlier events in history that include such events as contaminating blankets with small pox infection or dumping some known toxin or obnoxious waste into the neighbor’s well or livestock basins. Terrorism came to be a term when it impacted us directly, with us being on the receiving end for the most part. Bioterrorism was conceived of for use in medical records coding only a number of years ago, soon after it became clear that bioterrorism could strike developed countries just as much as it could be used again developing countries.
Terrorism has its way of impacting our physical means for living and earning money. Bioterrorism is an attack on life itself, sometimes fast, sometimes slow, depending upon the weapons chosen. Terrorism occurs when some upper league company is penetrated, its physical being, wares and stores. Bioterrorism takes place whenever things inside us or related to life are infected or penetrated.
Terrorism and Bioterrorism
During my early days as a teacher, some people asked me why I was so much into poisons. I told them this related to some experiences I had in high school teaching survival skills at the summer camps and some of the mistakes I made during those years. One of the first lessons I learned to teach at the camp is to be as well trained in knowing the lookalikes for plants as you are trained in the plants themselves. I liked to call these plants “toxic look-alikes”, and pertained to plants that could be confused for something you were trying to consume as a food.
To this day, the two most common examples of this problem still occur on a fairly annual basis. The first is the mistake of a relative of the wild hemlock, Oenanthe, for an edible ‘wild parsnip’ found growing along streams in the western states; it’s oenanthotoxin is often fatal. The second is to partake in the consumption of an amanita mushroom, usually by a person or persons who moved into the region where they found it and whom based their gathering of this mushroom on their experiences in Europe or Asia; its cyclooligopeptide amanitin is irreversibly hepatotoxin and fatal.
The two mistakes I made when I was 17 were simpler than each of these, and not fatal. For the first, I accidentally gathered some Iris root from a plant emerging one early spring alongside a cattail colony. Even though the rootstock has a very different appearance, I learned that biting into it left you with a dry tongue feel as if you bit into a large calcium tablet. For the second, I ate a small piece of arum root fully boiled and soft like an overcooked potato. The second piece was two or three times larger, not thoroughly cooked, and so still had oxalate crystals in it to make their way into my tongue, entire inner mouth, on down towards the throat. These events made me sit down and write up a list of the local poisonous plants, preparing me for what would take place once I entered the basic sciences focused institution Stony Brook University.
When I went away to college, I tried to continue these outdoor ventures but schooling had its effect upon many of these activities, that is until I obtained a lab assistant position during the the first month of my sophomore year working in a neurotoxicology research lab devoted to nerve axon sodium-potassium exchange studies. The focus of these studies was plant and animal poisons.
I came upon this opportunity by strolling into a lab one day because of its fish tank and several items posted on the bulletin board. In particular there were a couple of cone snails in the aquarium, which are highly toxic marine animals that I learned came from the Philippines. The professor sitting at his desk there saw me staring at these molluscs, of which I only had an empty shell which I kept as part of my teaching collection. By the end of the discussion with him I had a position as a research assistant studying squid-axons and their ionic channels. Although his work was not devoted to the cone snail venom (that topic was undertaken by the person he shared his lab with, whom I later became good friends with), it involved the use of tetrodotoxin, that toxin from the puffer fish that makes your mouth numb, some triethanolamine (tea) a potasssium binding site specific channel blocker, and a series of series of amazon arrow poisons all of which were plant derived, such as several strophanthidins and the famous ouabain.
At the time I had also just enrolled in a neurophysiology course focused on the topics of this lab research I obtained. My roommate was devoted to the same. What he knew by his book and lab experiences as a neurotoxicology researcher focused on animal poisons, and what I knew about plant toxicology and my field experience with plants, made us an unusual set of roommates for the year. He was also pre-med, and it was our discussions about neurophysiology that ultimately turned me away from focusing on just the environment, weather , ecology and plants in order to take on physiology and the human body for the remaining years in college. For the next year or two, my focus was on these topics, and while completing a series of special environmental health/environmental engineering classes on meteorology and climatology, I also worked as an EMT and training officer for the fairly large (100+ members) ambulance corps housed on-campus.
Emergency medicine is one of the most testosterone-driven professions in allied health. It combines the prestige of being in a very active medical profession, merging it with the behaviors and beliefs that being a police officer or fireman made you imagine when you were a kid. There are two topics in emergency sciences that pertain to this kind of work–poisoning cases and drug overdoses. Occasionally you come up with that scenario where poisoning and crime are merged, those very rare murders rare involving poisoning that you hear about but rarely if ever see as an an emergency respondent.
Poisoning was the topic I often taught, and people liked to attend my classes, even non-ambulance corps members, just to see all of the poisons I had collected over the years–which were the main topics of my class. My classes began by showing them what these substances looked like, in small glass vials, with the argument that recognizing a product in the field is important to such emergency call.s I usually began with the examples involving suicide and overdose cases, but ultimately always ended up talking about curare, ouabain, physostigmie, pilocarpine, atropine, and having examples of these for others to see. Of course, the use/abuse of these chemicals was rare, whereas the abuse and misuse of medication/street drugs on campus was wide spread. No matter, this method of engaging the students attracted quite a few visitors to my classes, and several years into this, I even took the opportunity to hold these classes in classrooms and lecture halls on main campus, instead of off the beaten path at the far end of campus in the infiromary building, for which the doors were closed after 5 on the weekends.

The main topic for this class was the Abrus precatorius bean from the Carribean, and the discussion of the famous assassination of George Markov of Bulgaria that recently was linked to these toxins in such a way that only a secret agent kind of story could be told in my classroom. This story then led to my mention of the lectin abrin which came from some beans I had a sample of, these small red and black spheroidal half pea-sized beans found of necklaces brought up from the Carribean by unsuspecting travelers. I had one of those necklaces recently purchased at the local church used goods store. Another toxic plants with lectins I like to bring up was the local native plant which I had a sample of, obtained from campus grounds–Pokeweed. This pokeweed mitogen was a regular ingredient in most genetic labs on campus; since it was unregulated at the time, once it was outdated, it got tossed into the regular garbage cans.
Back in the late 1970s and early 1980s, toxicology had some very loose associations with terrorism in the public eye. For the most part, most of what we knew about poisons related to the deaths of the Jamestown people due to Datura or the use of atropine and belladonna alkaloids associated with such tales about witchcraft and the Borgia family affair. There was that massacre down in Jonestown that some people knew about. A common theme in some history classes on campus included the tale of ergotism and how it influenced entire villages some times, causing mass hallucinations and hysteria to erupt.

All of this changed however in 1982, the last year of my undergraduate schooling. That is when the Tylenol scare erupted. This gave new life to the unique medical specialty known as toxicology. A few years later, even more of a concern about poisons and their use against people in masses came to be when in Japan, the neurotoxin savin was released into the subway tunnels. “Terrorism” had become a regular field of study in criminal and forensic science, and emergency medicine. possible use of the new neurochemicals being developed to poison the masses of people using a subway in Japan, poisons mostly linked just to chemical warfare before that event. (It was during this time that I in turned to creating the toxic syndrome database for diagnosing/recognizing intoxication cases based upon signs and symptoms, a database still in use to this day, in 2013, for evaluating herbal medicine induced intoxication.)
When I removed to Portland, Oregon in 1985, I almost immediately wound up in the local university setting exploring the possibility of having my own lab to analyze these chemicals. My background in this field soon became known by the chemistry department, ultimately leading one of their professors to offer me his lab for me to engage in this research. His area of specialty was the terpenoids, including steroids, essential oils, and a group of toxins and allergens called sesquiterpene lactones. I followed up on his offer and after completing a basic course he taught on medical chemistry, began researching my own topics of choice, with free reign of both the lab and the chemical stores.
My interests in toxicology remained with me during this time, and quite soon my main topic of research was the benzylisoquinoline alkaloids group. This group of toxins involved complex chemicals, poisons, drugs and anti-cancer agents. My goal was to develop a theory as to how and why the plants evolved these compounds.
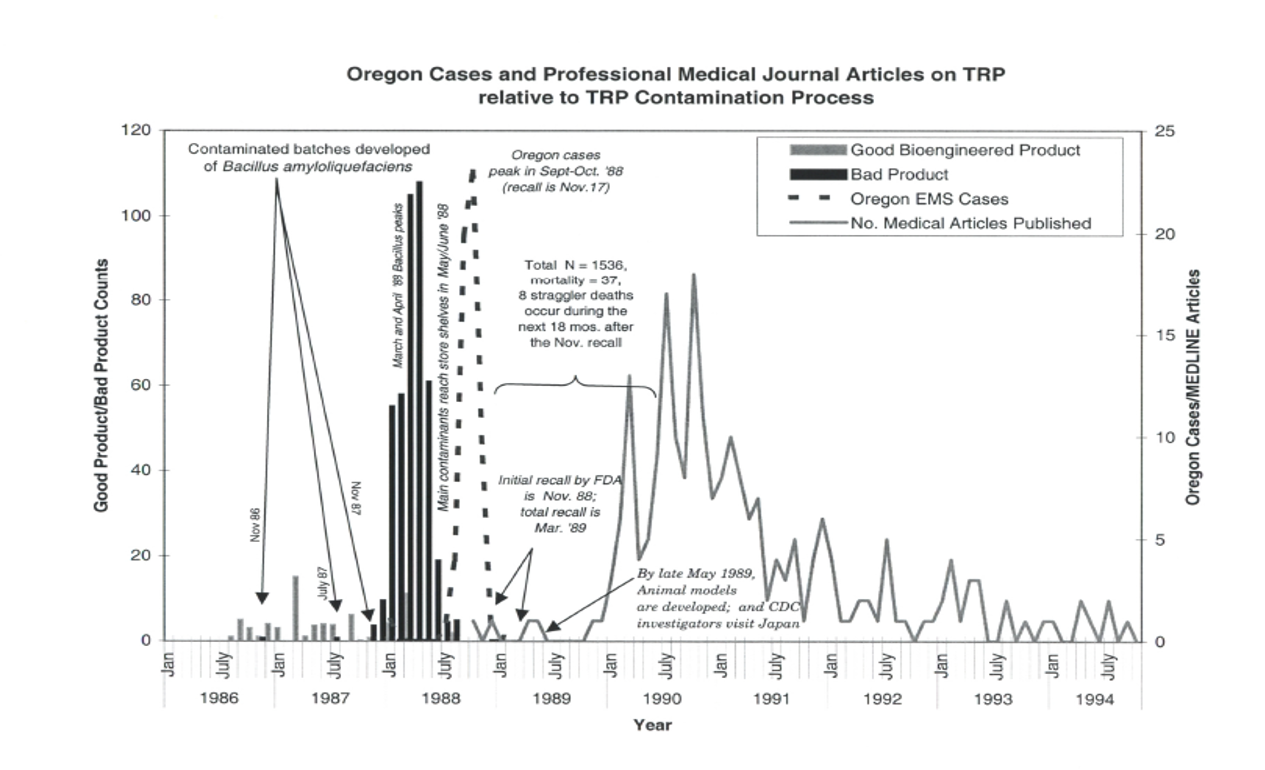
Then, the tryptophan tragedy happened. A student of mine (I was a medical chemistry lecturer and student advisor) had a cousin in southern Oregon who told her said she had just been diagnosed with a rare disease due to an over-the-counter. I was given her doctor’s name and number, and so called him so he could send me a sample of these medicines for further review in my lab. Based on the symptoms and type of disease presentation reported, the senior researcher/professor of my lab and I felt it had something to do with the use of Vanadium in sealing the storage containers it would have been stored or shipped in. Neither of us considered bioengineering as a cause, or the lack of regulation and adequate testing of OTCs produced using this new manufacturing method–the tryptophan was produced in excessive amounts metabolically, as a by-product of a genetically engineered bacterium that was then leaked into the growth tank and extracted in order to produce the over-the-counter product.

Three months later, the cause for these cases was revealed. A previously undiscovered by-product of bacterial metabolism–a uniquely bound ditryptophan. The focus of some of the lab’s work from this point on switched back to the bioengineering of plant derived compounds, including toxins (I first initiated this work in 1987/8, but the industry was still in its infancy.) One of the agents responsible for manufacturing substances from plants for specific food or drug products, was found to be using the waste left over to produce other compounds for use in the manufacture of poisons and explosives, for a foreign country places on a watch-list. From this point on pretty much, this field evolved into the field of chemical and biological warfare and terrorism that we hear about today.
The utilization of neurotoxins in the Japanese subway incident and evidence for the use of biological weaponry by Iran did much to bring to light the possibility of bioterrorism as a home-targeted or home-grown public health threat. The tylenol problem resulted in better packaging and safety precautions. The tryptophan problem focused on monitoring and regulating bioengineered products, with some of this political power used to deal with over-the-counter nutritional supplement marketing guidelines as well.

But these events were accompanied now by international travel and trade related events, suggesting to us the possibility that in-migration of foreign born diseases and the use of diseases as potential weapons could be in the near future. We were initially warned of this possibility when the first in-migration of Ebola occured via a plane to Toronto. Another example of the need to monitor diseases more effectively came when rats infested with Hanta Virus migrated from the southwestern US into the Pacific Northwest in the late 1900s, due to a drought.

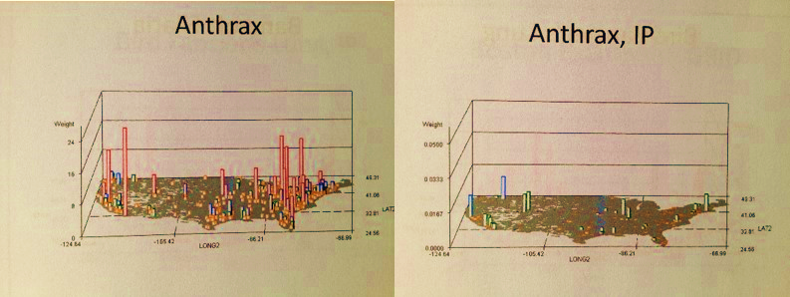
Then came the realization that bioengineered foodstuffs such as crops and livestock could be vulnerable to natural ecological threats and human-induced ecological threats to this important industry. These concerns in fact led to the initiation of a GIS designed specifically to deal with these particular national security and public health needs.
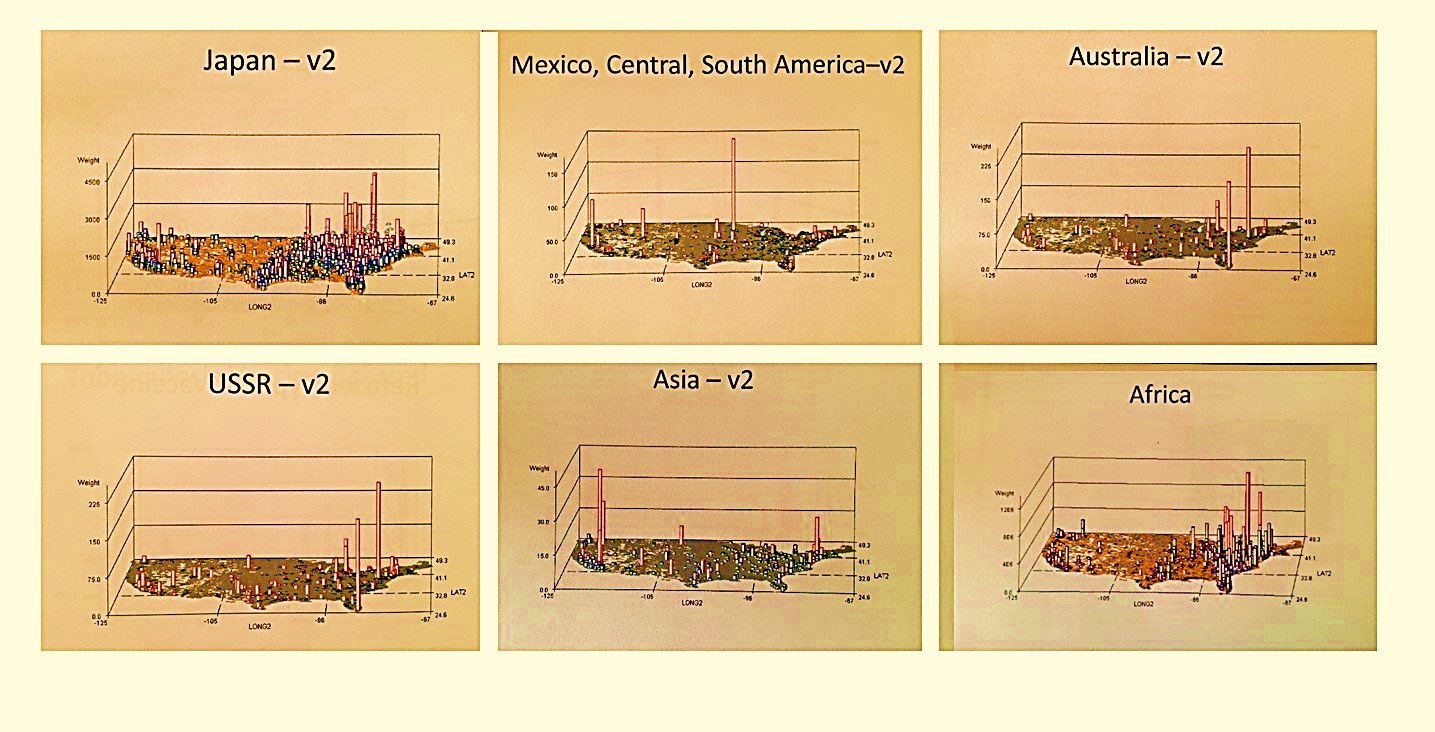
Distributions of sets of infectious, vectored, or ecological diseases that come in from other continents
Beginning in the mid-2000s, I reviewed a variety of psychological behavioral syndromes and conditions linked to terrorism activities. I found that Emergency Room visits codes could provide us with insights into this important public health issue. I wanted to see if behaviors like those which led to the Columbine incident in the state where I was then living, Colorado, could recur elsewhere. I found this behavior to be hard to link to such EMR data; the requirements for the next subway killer, school murderer, movie theater gunman seemed well dispersed throughout the U.S..
 .
.
With regard to terrorism as an E-code, however, my first impression was that it is more of an East Coast event, perhaps brought on by multiculturalism, or due to the crowded populations setting faced there everyday, seemingly making you more vulnerable to criminal activities and psychological events you’d rather not become a part of. But living in the Pacific Northwest I could also see another major social behavior that tended to result in social violence–like the anti-Global, and anti-World economy movement that was developing and giving rise to problems at the annual international trade groups meetings held in Seattle.
So it ends up that many if not all of these behaviors are fairly well distributed across this country. However, locality plays an important role in these behaviors and so need to be spatially monitored. For example, some problems I found to exist as pockets in certain urban-suburban settings were never included in my national database research. So the databases don’t capture everything you need to know about someone in this country. I personally found that important examples of social threats exist in the most rural anti-government parts of this country, such as rural Montana and the like, where gun-ready, self-governing survivalist communes have evolved and been raised in greater numbers in recent years, and which due to their lack of attendance to a regular health care system, remain undocumented for the most part in any EMR databases made available to the US Bioterrorism and Response programs.

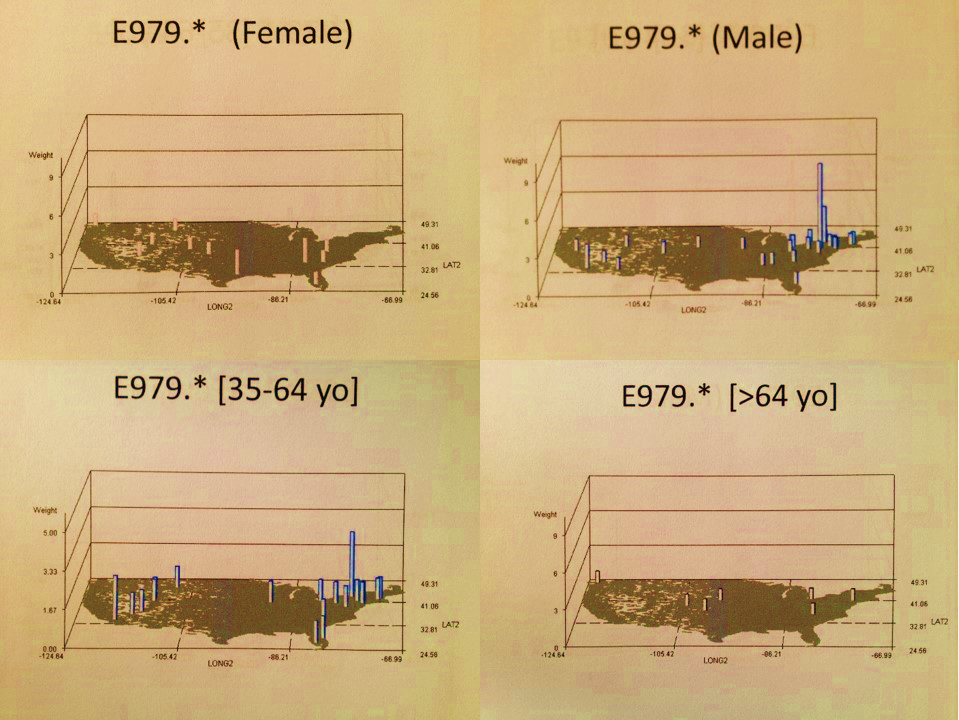
Nevertheless, we can still use EMR data to monitor and document population health in terms of criminal activities, the development of an effective forensics exploratory database, and the implementation of a profiling technique for evaluating behavior types at the personal, social and regional level. For example, the following spatial review I carried out for three conditions possibly related to terrorist attitudes, mass killing episodes and the like, failed to demonstrate a “predictable pattern” but still demonstrated “hot spots” in need of review or recall at some later point, should a new terror or mass murder event arise. In the least, researching why these small 25 mi areas form peaks would be of some benefit to such activities.
We can also look at these maps and then retrospectively try to give cause or assign reasons to these events after they have happened, but we cannot necessarily use past terrorism data and past psychiatric/human psychology to help us predict where these events are most likely to happen.
In the end, two rules do seem to prevail however for such terrorism and mass murder events.
- First, areas where there are a lot of people involved are at highest risk, the reasons for which are obvious.
- Second, areas where money and western capitalism live and thrive abundantly also define those regions which are most at risk.
Places like the former World Trade Center, threats made to the largest shopping malls, threats made to examples of some of the largest symbols of capitalism in this country, are anti-US events that were motivated not so much by a group engaged cause, but by individuals who considered themselves to represent that group cause–people who became self-motivated by their anti-corporate, anti-capitalist attitudes, enough to become “terrorists” in our mind, “heroes” in their own.
The recent tragedy in Boston represents another example of this antisocialism out there perpetrated by individuals, some of whom could be predictable. A detailed look at e979 shows that there are certain places where certain age-related behaviors linked to terrorism prevail. This will be covered in the next section of this work
.
To Be Continued

Leave a comment