July 2014
Monthly Archive
July 22, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on Plague (IP) – YouTube
As in Bubonic Plague, carried by various mammals, esp. prairie dogs in the western and southwestern U.S. Associated with flea vectors. Pest: Yersinia pestis….
Source: www.youtube.com
Geographically, you’d expect the plague to be western-bound. But significant numbers of cases are reported all over the United States since 2010.
The east coast peaks in cases demonstrate something unexpected about this diseases. Historically, we think of it as the great bubonic plague, once gone awry but now under considerable control. In the U.S., we often learn about the association of the plague with prairie dogs. Since the flea is its vector, you need only be near a prairie dog colony to potentially be exposed to this organism. (Not great news for us Western field epidemiologists out there dealing with other zoonotic diseases.)
But the matching high peaks along the west coast points to population density as well influencing where the cases are reported. This should be no surprise, since peoples’ presence is needed for human cases to be developed, and then later reported.
So initially, this map tells us that the plague could be transmitted by many other diseases, in both natural and human ecological manners, and unfortunately bearing reasons for its potential urban impacts that in some ways are very different from why and how it becomes a rural epidemiological event.
However, people travel, and in-migration routes makes their way to the heavily populated ports for international shipping.
Is latitude a feature in how and where an imported case of the plague might enter the U.S.? Perhaps, since climate does impact both vector and host activity patterns and willingness to travel or change both animal and environmental settings.
Population density is more a concern for international spread of Yersinia pestis should some new, resistant strain emerge.
Is the Pacific Rim a route of travel to consider? If you ask a west coast public health economist or epidemiologist, most certainly.
Still much of the commercial travel from the Orient follows traditional routes, and the more heavily, most heavily populated regions of the east coast are very likely to produce some of the first cases if their origins were abroad.
This leaves only a single isolated peak in the midwest to be better understood.
July 15, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on 500 in Africa, 350,000 in the Americas . . . Updates on the recent Outbreaks and more
The ratio of Mosquito diseases, like Chikungunya, to Primate hosted diseases like Ebola, is 700:1 (rounding Ebola cases to 500 total). yet the fatality of Ebola is so horrendous, visual and high in terms of percentages, that we focus much more on the Ebola outbreak than we do a disease creeping into our ecology slowly by means of ongoing host-vector behaviors. There are other diseases that penetrated the ecology of North America even more slowly that those which are mosquito borne.
Source: m.yahoo.com
The very slow migrating tick borne diseases such as lyme disease remains a very important public health issue, but its victims remain uncounted by most news writers. Lyme disease victims do have their issues you know.
See:
1. Lyme Victims from Around US to Gather at IDSA Headquarters and Demand Changes to Guidelines for Lyme
Thursday, 15 May 2014. http://truth-out.org/speakout/item/23732-lyme-victims-from-around-us-to-gather-at-idsa-headquarters-and-demand-changes-to-guidelines-for-lyme
2. Views: Give Lyme victims same rights as other patients
Holly Ahern. Poughkeepsie Journal. http://www.poughkeepsiejournal.com/story/opinion/valley-views/2014/06/14/lyme-disease-patients-chronic/10533911/?from=global&sessionKey=&autologin=
In August 2013 it was estimated by CDC that about 300,000 new lyme disease cases are identified each year (as many as twice of much are estimated however due to underreporting; CDC. http://www.cdc.gov/media/releases/2013/p0819-lyme-disease.html) .
If the same holds true for 2014, that means the ratio of the three diseases so far discussed are 700:600:1, for Chikungunya:Lyme:Ebola. [For CDC info page on Lyme, see http://www.lymediseaseassociation.org/index.php/resources/cases-a-other-statistics ]
Not add to this west nile cases, which are incredibly scarce. So far, perhaps <50 in the U.S., but it is still quite early. (see http://www.cdc.gov/westnile/statsMaps/preliminaryMapsData/ and July 8 data– http://www.cdc.gov/westnile/statsMaps/preliminaryMapsData/histatedate.html  😉
Still in spite of all of these significant number differences, the public is in general most reactive to Ebola, because it is so deadly (30-50%), and because there’s that expectation for what might happen.
West Nile is deadly too, but mostly to elders and children and those of a weak immune system or "constitution", and even so, deaths are infrequent to rare. There are no deaths as of yet in the U.S. due to Ebola, but such a case would take center stage if it were ever to happen. Lyme disease we’ve grown adjusted to. Chikungunya we’ve also got our eyes upon.
SO WHAT HAVE WE FORGOTTEN?
Anthrax, Arboviral diseases, neuroinvasive and nonneuroinvasive,
Powassan virus, Cholera, Dengue Virus Infection, Dengue fever, Dengue hemorrhagic fever, Dengue shock syndrome,
Hansen disease (leprosy), Malaria, Plague, Poliomyelitis – paralytic
Poliovirus infection – nonparalytic, Psittacosis, Q fever, Severe acute respiratory syndrome-associated coronavirus (SARS-CoV) disease, Omsk Fever, Russian Tick Disease(s), Shiga toxin-producing (STEC), Shigellosis, Trichinellosis, Tuberculosis, Tularemia, Typhoid fever, Vibriosis, Viral hemorrhagic fevers, New World Arenavirus, Crimean-Congo hemorrhagic fever virus, Ebola virus, Lassa virus, Marburg virus, Yellow fever, and dozens more which we can’t immediately recall the names of.
SEE:
My "Foreign Disease Intrusion" list (no NPHG video links) at https://brianaltonenmph.com/gis/global-health-mapping/foreign-disease-intrusion/
National Institute of Allergy and Infectious Diseases. Emerging and Re-emerging Infectious Diseases. http://www.niaid.nih.gov/topics/emerging/Pages/list.aspx and http://www.niaid.nih.gov/topics/emerging/Pages/Default.aspx
Deborah A. Adams, Kathleen M. Gallagher, Ruth Ann Jajosky, et al. (2012). Summary of Notifiable Diseases — United States, 2010. MMWR. June 1, 2012 / 59(53);1-111
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5953a1.htm
Ronald Barrett, Christopher W. Kuzawa, Thomas McDade, and
George J. Armelagos. (1998). EMERGING AND RE-EMERGING
INFECTIOUS DISEASES: The Third Epidemiologic Transition. Annu. Rev. Anthropol. 1998. 27:247–71. http://epa.gov/ncer/biodiversity/pubs/ann_vol27_247.pdf
Brian D. Gushulak, and Douglas W. MacPherson. Globalization of Infectious Diseases: The Impact of Migration
Clin Infect Dis. (2004) 38 (12): 1742-1748. doi: 10.1086/421268
http://cid.oxfordjournals.org/content/38/12/1742.full
Manny Alvarez. July 7, 2014. Dr. Manny: Is America on the verge of a major health crisis? http://www.foxnews.com/health/2014/07/07/dr-manny-is-america-on-verge-major-health-crisis-985339470/
Cal Thomas. (July 8, 2014). Immigration crisis: Our Constitution doesn’t guarantee entry to the United States.
http://www.foxnews.com/opinion/2014/07/08/immigration-crisis-our-constitution-doesnt-guarantee-entry-to-united-states/
The concerns about IN-MIGRATING DISEASE PATTERNS are reviewed in the following reports:
Robbie J. Totten. Contagious Disease, Epidemics, National Security, and U.S. Immigration. CDC, 2012. Historical Policy Responses.
http://ccis.ucsd.edu/wp-content/uploads/Robbie-J-Totten_Epidemics-and-U-S-Immigration-Policy-2.pdf
Association of State and Territorial Health Officials . (2013). Global Infectious Disease Impact on State and Territorial Health.
ASTHO Global Health Meeting, July 31, 2013, Washington, DC. http://www.astho.org/Programs/Infectious-Disease/Refugee-Health/Global-Infectious-Disease—Impact-on-State-and-Territorial-Health/
Ruth Ellen Wasem. Specialist in Immigration Policy, Congressional Research Service. April 28, 2014. Immigration Policies and Issues on Health-Related Grounds for Exclusion.
http://fas.org/sgp/crs/homesec/R40570.pdf
Other MEDICO-POLITICAL NEWS regarding disease patterns and immigration:
Immigration Issues. Illegal Immigration and Public Health (2009) http://www.fairus.org/issue/illegal-immigration-and-public-health
PolitiFact Texas. Dan Patrick has called illegal immigration an invasion and said immigrants bring ‘Third-World diseases’ http://www.politifact.com/texas/statements/2014/jun/20/battleground-texas/dan-patrick-has-called-illegal-immigration-invasio/
Marc Siegel. Fox News. Immigration crisis: US experiencing major public health crisis, too. http://www.foxnews.com/opinion/2014/06/30/immigration-crisis-us-experiencing-major-public-health-crisis-too/
Ryan Lovelace. William F. Buckley Group Fellow. Texas Immigration Center a Magnet for Disease. Border Patrol union says poor medical screening risks new virus outbreak. http://www.nationalreview.com/article/381101/texas-immigration-center-magnet-disease-ryan-lovelace
Laura Murphy. The Guardian. The Mexican ‘germ invasion’ is just the right’s latest anti-immigration myth. http://www.theguardian.com/commentisfree/2014/jul/02/border-patrol-diseases-anti-immigration-myth [note: potential bias noted due to relation to missionary activities]
MY RESEARCH on this (one of several NPHG video sets of foreign born viral, vectored, hosted and/or zoonotic diseases, in YouTube:
By diseases — https://www.youtube.com/playlist?list=PLWrApErk5byZnE0bWUqdfH4CYVmnETLg6
By regions or countries — https://www.youtube.com/watch?v=zQ60npQzdTk&list=PLWrApErk5bybFfsOWTXWjlwvIM7D4d6-h
July 11, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on Vectors or Victims? Docs Slam Rumors That Migrants Carry Disease

“Doctors say they are concerned about false rumors and “hysteria” that the unaccompanied children coming across the border from Mexico into Texas are carrying diseases such as Ebola and dengue fever.”
Source: NBC News. Maggie Fox. (dated July 9, 2014). “Vectors or Victims? Docs Slam Rumors That Migrants Carry Disease” http://www.nbcnews.com/storyline/immigration-border-crisis/vectors-or-victims-docs-slam-rumors-migrants-carry-disease-n152216
WELL WHAT ABOUT THE OTHERS.
Source: www.nbcnews.com
As is often the case, concerns, fear and even panic arise with some of the worst logic. The fear may be right and have good reasons for its existence, but unless we consider the alternatives for how else it might apply, we could result in two series of negative historical epidemiology events–ignoring the original claim because it is misapplied, and missing the boat as how to better apply it.
NPHG mapping doesn’t support the claim that in-migrating from Mexico and lower parts of the Americas in unlikely to bring in diseases for us to be concerned with.
Ecological fallacy is when you believe your observations and deductions pertain to a much larger area or population. Such is the case for those arguing these "false rumors."
The support for the "possibility" (a term we should even consider removing from this sentence) that in-migration patterns do not increase the risk of behaviors and disease coming in from other areas, peoples and culture is absurd. We can try arguing the point that immunizable diseases is not a concern, because we can simply provide these as soon as they come in, although many underprivileged classes in this country also in need of these medicines will most certain fell neglected, and rightfully so.
The article is right in stating the concerns about dengue fever are overrated (see video), and my Ebola work is appearing to show that this is also unlikely to be linked to Mexico in-migration, as much as Caribbean or Natural Animal in-migrating patterns.
The argument that sufficient quarantine and public health monitoring strategies are in place only holds for those who enter this country legally.
The real indicators here are the presence of in-migrated diseases from countries to the south, such as the most obscurest of ICDs with a well-defined cultural relationship–Chiclero’s Ear and Pinta.
But we can add more to this if need be. Vibrio cholera outbreaks from a strain bred in Peru, Brazilian blastomycosis, and venezuelan encephalitis.
As I recently demonstrated on one of my ScoopIt! pages about Ebola, the most likely route of entry naturally is via the Caribbean and/or South to Central American route, through the eastern Texas-Mexico border, directed Northnortheastward. The human in-migration route, more likely, involves major airports from Africa.
See:
Dengue, at https://www.youtube.com/watch?v=eHyehbfOwFo
El Tor cholera at https://www.youtube.com/watch?v=m5tccQopKFE (demonstrates a nidus in the NYC area, due to rule outs and high density of cases, but the major localized cluster in the Southwest)
Brazilian Blastomycosis, https://www.youtube.com/watch?v=bPgOWoC1lO8
Chiclero’s Ear (route very strongly demonstrated), https://www.youtube.com/watch?v=BmLlfLze1Lo
Pinta, using an earlier and very unique presentation technique, at https://www.youtube.com/watch?v=KCTueptEHlc
Venezuelan Encephalitis, https://www.youtube.com/watch?v=iuKuvqAlZFU
Disease distributions in the US for ICDs linked to Middle and South America, https://www.youtube.com/watch?v=dk7z6dbGuj8
My coverage of the disease in-migration for numerous parts of the world: https://www.youtube.com/watch?v=zQ60npQzdTk&list=PLWrApErk5bybFfsOWTXWjlwvIM7D4d6-h
July 8, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on 1st case of mosquito-borne chikungunya disease in Polk County
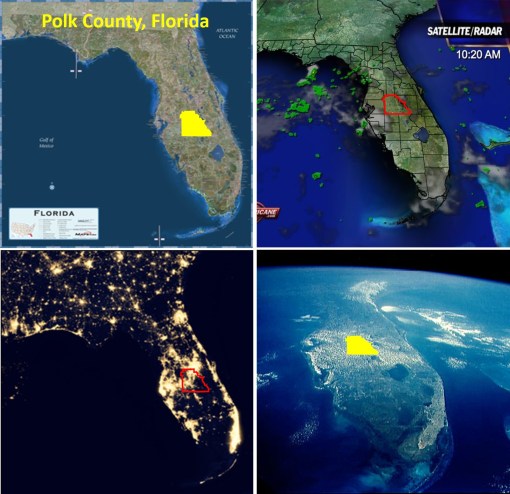
There have been 48 confirmed cases of the mosquito-borne illness in Florida.
Source: www.wtsp.com
This pattern is behaving very predictably, based on yellow fever behaviors documented since 1797, and some of the vibrio cholera patterns in U.S. soil since 1832. There is a northward transgression of mosquito born diseases (for obvious reasons). As documented in some west nile work from 2000-2005, ecological methods may be used to predict ecosystems most likely to harbor the species that serve as the most active vectors. (see my canopy light penetration field work for starters – at https://brianaltonenmph.com/west-nile/west-nile-surveillance-2/ ).
Further comparing vibrio and chikungunya, vibrio is water dependent and ecologically bound to it deltaic settings (i.e. New Orleans and Galveston area–though some will dispute me about this), and is fully dependent upon isopods. On the other hand, chikungunya behaves according to mosquito patterns much like the yellow fever and dengue, and lacks the stricter peri- and subaquatic requirements.
My standards for performing mosquito vector disease ecology research as a small area GIS study are provided at https://brianaltonenmph.com/west-nile/west-nile-surveillance-2/
Remote sensing methodologies are reviewed in detail at https://brianaltonenmph.com/west-nile/6-remote-sensing/
The following outline begins at https://brianaltonenmph.com/west-nile/
West Nile Surveillance – http://wp.me/Puh6r-rY The Research Area – http://wp.me/Puh6r-sa Vectors – http://wp.me/Puh6r-yJ Assigning Risk – http://wp.me/Puh6r-sd Host Surveillance – http://wp.me/Puh6r-sh Vector Ecology and Surveillance – http://wp.me/Puh6r-su Plant Ecology – http://wp.me/Puh6r-gL Topography – http://wp.me/Puh6r-sq NLCD Grid Mapping and West Nile – http://wp.me/Puh6r-sO West Nile – Light Penetration Study – http://wp.me/Puh6r-gN Remote Sensing – West Nile – http://wp.me/Puh6r-dH Case-related Surveillance – http://wp.me/Puh6r-sX
ENDNOTES:
Images from : Wikipedia, Florida and Polk County, MyFoxHurricane.com, National Park Service (Everglades project – “Lightscape / Night Sky” at http://www.nps.gov/ever/naturescience/lightscape.htm, and South Florida Aquatic Environments, at https://www.flmnh.ufl.edu/fish/southflorida/pisces.html
July 8, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on The Geography of Ebola: important spatial features influencing its diffusion patterns
This set of maps can be reviewed in detail at
http://www.pinterest.com/pin/568790627911639938/
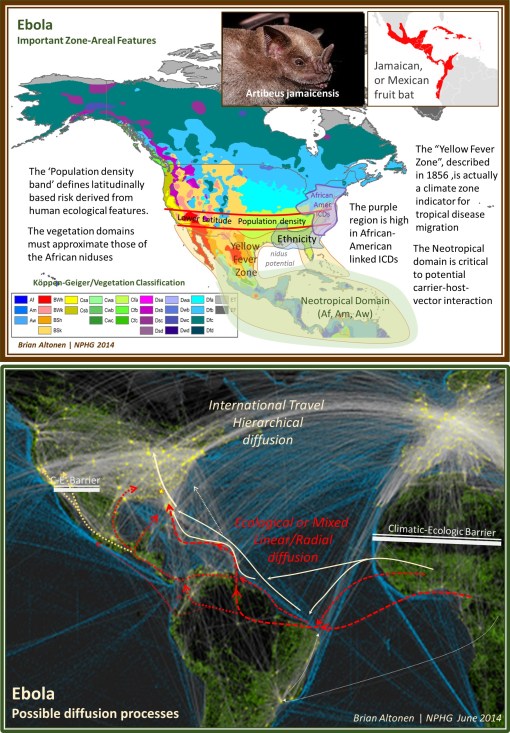
The Geography of Ebola, goes one step beyond the environmental ecological concept of Ebola patterns. Past geographers had a unique way of evaluating disease long before the microbial (pre-bacterial) theory became popular in the mid-1870s. Using some of these older methods of spatially reviewing disease behaviors, we discover some important insights worth pursuing as spatial epidemiologists. Amongst these are spatial theories linked to density, diffusion processes and the natural history of disease over time as natural endemic or epidemic disease processes.
By 1800, the latitude theory for disease was already well established. This identified certain regions close to the equator and hot, humid climates as most conducive to bad health (see https://brianaltonenmph.com/gis/historical-medical-geography/1814-the-latitude-of-pestilence/ ). Matching the latitude theory was the longitude theory, which had its support as well in the form of diseases that remained in the Americas and failed to infect Europe, at least in the initial years. The prime example of this was yellow fever during its first decade or two of infecting North American coastal cities (this are on the map is from Alexander Keith Johnston’s map, which I review extensively at https://brianaltonenmph.com/gis/historical-disease-maps/alexander-keith-johnston-health-disease/ ). Race and place of origin have also been linked to sickness, based on the argument of certain kinds of people being more “adapted” to specific settings. The belief that climate and weather were related to diseases was as old as the study of medicine itself. Adding to these early hypotheses by the mid-1800s were the ecological and natural history theories, based upon topography, soil, water, and unique features like slope and aspect (angle relative to the sun, for example for a mountain face).
20th century renderings of climate, weather, vegetation zones, and an areal feature known as the Köppen-Geiger climate classification system has become important in understanding global ecology. [for an original map see http://www.ie.unimelb.edu.au/research/water/hydroclimatology.html ]. Understanding global ecology is important to understanding the geography of Ebola. Ebola is specific to certain Köppen-Geiger regions ‘Af’, ‘Am’ and ‘Aw’ in Africa, and therefore similar regions in other parts of the work are more like to support the natural migration of this disease elsewhere. The Amazon Basin is the only part of the Americas that match the equatorial tropical rainforest region in African where Ebola erupted from. In the above map illustrated I have termed this the U.S.-Middle America Neotropical region. These region in both South America and Africa very much mimic the “Torrid Regions” defined around 1800 by famous geographer Alexander Humboldt. [See
http://libweb5.princeton.edu/visual_materials/maps/websites/thematic-maps/quantitative/meteorology/meteorology.html ].
The African bats linked to Ebola are fruit-eaters (frugivores). This differentiates them from nearly all North American bats which are insectivores. In Middle America, are a variety of nectar-feeding and fruit-feeding bats, in particular that Jamaican fruit bat (Artibeus jamaicensis), of which at least four varieties occupy the Caribbean environments (see insets in upper map above, and
http://en.wikipedia.org/wiki/Jamaican_fruit_bat ). Thus the link between the African diffusion process and the American diffusion process are these fruit bats, for the time being.
The barriers to Ebola diffusion in nature are the non-tropical forest, very dry and arid climatic regions along most of the western U.S. Mexican border. This barrier mimics the barrier the Sahara is to natural northward migration of Ebola. Thus only the entry though the San Antonio, Texas area appears to have feasible climate, topography and environmental settings required for such a host or carrier to follow nature and carry the disease northward to the more heavily populated latitudes.
The Neotropical shorelines of this region extend eastward towards Florida, which due to their combined climate and floral features could support the frugivore bats, but an even more adventitious route for the travel of Ebola from Brazil to the U.S. is via the Caribbean. This route was favored by yellow fever, Asiatic cholera, malaria, dengue, and most recently Chikungunya.
The transportation map at the bottom shows two types of disease diffusion routes–the natural ecology routes (linear, radial, mixed or non-hierarchical, red and orange) and the human driven hierarchical transportation based routes (white to cream). The above maps focus on the natural history of this part of the globe relative to the disease ecology for Ebola. It is just as possible for human transportation to be the primary means this disease attempts to strike the U.S. (white to cream colored routes).
Meanwhile, the natural history derived routes, for an in-migrating disease like Ebola, which I placed on the second map (in red and yellow), are for the most part speculative, but stand as useful and testable prediction models.
Readings and more related to the above:
Global Disease Detection Center. [CDC set up these facilities to monitor, perhaps suppress diffusion.] Info and a map detailing their locations (in Guatemela, as of 2006) is at
http://www.cdc.gov/globalhealth/gdder/gdd/regionalcenters.htm
Hierarchical Diffusion modeling, my review at: https://brianaltonenmph.com/gis/historical-disease-maps/john-c-peters-and-the-asiatic-cholera/1960-pyles-cholera-diffusion-and-migration-patterns/
and a contemporary application of it: http://onlinelibrary.wiley.com/doi/10.1002/sim.844/abstract
Studies and news quips about Ebola and other bat-carried diseases:
http://www.infectionlandscapes.org/2012/11/ebola-hemorrhagic-fever.html
http://www.infectionlandscapes.org/2012/12/marburg-hemorrhagic-fever.html
Pierre Rouquet, Jean-Marc Froment, Magdalena Bermejo, AnnelisaKilbourne, William Karesh,Patricia Reed,Brice Kumulungui, Philippe Yaba, André Délicat, Pierre E. Rollin, and Eric M. Leroy. (2005). Wild Animal Mortality Monitoring and Human Ebola Outbreaks, Gabon and Republic of Congo, 2001–2003. 11(2), serial on the internet, available at http://wwwnc.cdc.gov/eid/article/11/2/04-0533, or
http://wwwnc.cdc.gov/eid/article/11/2/04-0533_article.htm
Ivan V. Kuzmin, Brooke Bozick, Sarah A. Guagliardo, Rebekah Kunkel, Joshua R. Shak, Suxiang Tong and Charles E. Rupprecht. (2011). Bats, emerging infectious diseases, and the rabies paradigm revisited. Emerging Health Threats Journal 4, incl Supplements. At:
http://www.eht-journal.net/index.php/ehtj/article/view/7159/8775
Jorge Ortega and Iva´n Castro-Arellano. (2001). Artibeus jamaicensis. Mammalian Species, 662, 1–9. At http://www.science.smith.edu/departments/Biology/VHAYSSEN/msi/pdf/662_Artibeus_jamaicensis.pdf
Alfonso Valiente-Banueta, María Del Coro Arizmendia, Alberto Rojas-Martíneza, & Laura Domínguez-Cansecoa. (1996). Ecological relationships between columnar cacti and nectar-feeding bats in Mexico. Journal of Tropical Ecology, 12(1), 103-119. doi:http://dx.doi.org/10.1017/S0266467400009330 [Note: nectar feeders, Mexico species, not demonstrated to be a potential carrier as of yet.]
And
Yale Edu. 15 OCT 2009 REPORT: The Spread of New Diseases:
The Climate Connection. At
http://e360.yale.edu/feature/the_spread_of_new_diseases_the_climate_connection/2199/
The African ICDs work is from NPHG modeling of ICDs. I describe my process for this at
Defining and Stratifying Risk based upon ICD-Culture Relationships
The following also relate:
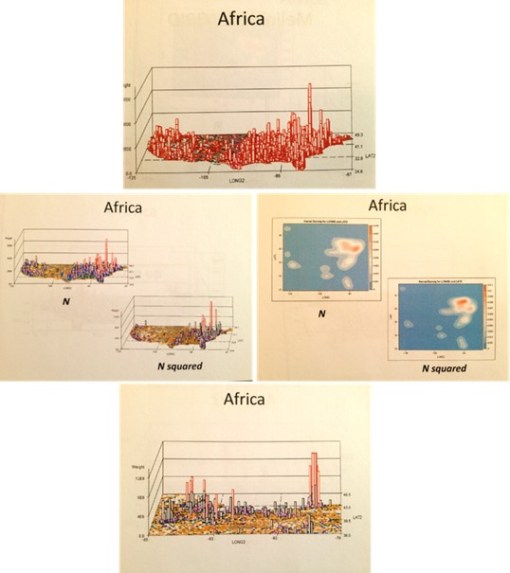
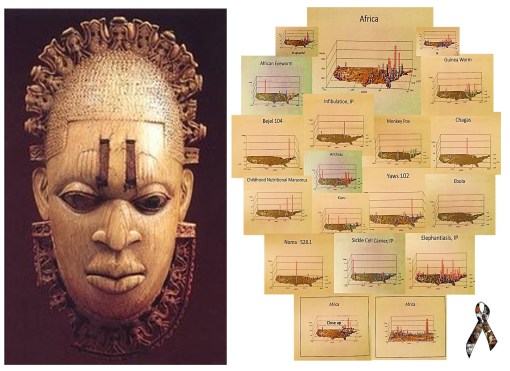
The blue maps are SAS produced krigged data maps. In other words they are very accurate. One has to image the US figure drawn on them, however, for some of the versions I produced.
The two maps are at http://www.pinterest.com/pin/568790627911639938/.
July 4, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on W. African Ebola epidemic ‘likely to last months’, says UN

JULY 4, 2014. Ebola News and Information Updates.
Source: uk.news.yahoo.com
July 14, 2014. The long term predictions for Ebola are not overly surprising.
A fairly realistic view of outbreaks like those for Ebola rely upon the assumption that these outbreaks are primarily of natural and human ecological in nature. In the long run this can means that they are more difficult to suppress than a disease diffusion process that lacks a natural ecological component, and is dependent mostly upon just people interacting with other people, mostly in human occupied places.
We learn about future disease patterns for a disease from other countries by looking at how similar diseases behaved in the past. The behaviors of west nile for example to date have been very much like those of the early 19th century yellow fever. The diffusion processes for the recent outbreaks from the Caribbean of Chikungunya are very similar to vector-host relationships, climate of origin and diffusion by transportation for the 19th century typhoid fever. As for Ebola, . . .
these few observations beg the question: If we apply to this same logic to Ebola, relying upon matchable natural and human ecological matching disease patterns, what might we come up with?
Current speculation is we are still far from the opportunity for a diffusion of Ebola to other parts of the world. Ebola’s zoonotic behaviors suggest a limited "metazoonotic" region (according to Pavlovsky’s and Voronov’s definitions) for the time being. Until the host-vector ecology is somehow changed, or its genetically defined tendencies to survive based on interactions with nature change, the "metaecology" of host, vector, organism and combinations thereof remain the limiting factor(s).
EBOLA LINKS/UPDATES:
UK NEWS. (July 3). W. African Ebola epidemic ‘likely to last months’, says UN. At https://uk.news.yahoo.com/w-african-ebola-epidemic-likely-last-months-says-185447906.html#fakodRB
CBS News (July 2). Ebola rages through West Africa, with no signs of stopping. At http://www.cbsnews.com/news/west-africa-struggles-to-fight-off-ebola/
The Guardian. (July 2). Monica Mark. Fear and ignorance as ebola ‘out of control’ in parts of west Africa. At http://www.theguardian.com/world/2014/jul/02/-sp-ebola-out-of-control-west-africa
ALJAZEERA. (July 2).
Ghana hosts crisis talks as Ebola toll rises.Ministers from 11 African nations meet to plan "drastic action" as death toll from haemorrhagic fever reaches 467.
http://www.aljazeera.com/news/africa/2014/07/crisis-talks-held-as-ebola-death-toll-soars-20147282632436552.html
THE TELEGRAPH. Mike Pflanz. (July 3). Ebola ‘out of control’ in West Africa as health workers rush to trace 1,500 possible victims. Fear, mistrust of Western medicine and difficulties reaching remote areas mean hundreds of potentially infected people have not yet been found. At http://www.telegraph.co.uk/news/worldnews/africaandindianocean/guinea/10942598/Ebola-out-of-control-in-West-Africa-as-health-workers-rush-to-trace-1500-possible-victims.html
CNN NEWS. Laura Smith-Spark. (July 3). Ebola virus: Can nations stop deadliest ever outbreak from spreading? At
http://www.cnn.com/2014/07/03/health/ebola-outbreak-west-africa/
BBC NEWS. (July 3). Ebola outbreak: West African states agree strategy. At http://www.bbc.com/news/world-africa-28156263
CBC NEWS. Daniel Schwartz. (July 4). Ebola epidemic unlikely to spread beyond Africa. Deadliest outbreak of the disease still a challenge to contain. At http://www.cbc.ca/news/health/ebola-epidemic-unlikely-to-spread-beyond-africa-1.2695879
CHIKUNGUNGYA. LINKS/UPDATES:
European Centre for Disease Control and Prevention. Chikungunya. http://www.ecdc.europa.eu/en/healthtopics/chikungunya_fever/pages/index.aspx
Eric M. Leroy, Dieudoné Nkoghe, Benjamin Ollomo, Chimène Nze-Nkogue, Pierre Becquart, Gilda Grard, Xavier Pourrut, Rémi N. Charrel, Grégory Moureau, Angélique Ndjoyi-Mbiguino, and Xavier de Lamballerie. (2007). Concurrent Chikungunya and Dengue Virus Infections during Simultaneous Outbreaks, Gabon, 2007
Emerging Infectious Diseases. Volume 15, Number 4—April 2009. At
http://wwwnc.cdc.gov/eid/article/15/4/08-0664_article
NBC News – MAGGIE FOX. Bugs at Your July 4th BBQ? Beware of Chikungunya and West Nile. At
http://www.nbcnews.com/health/health-news/bugs-your-july-4th-bbq-beware-chikungunya-west-nile-n147881
MICHAELEEN DOUCLEFF. Chikun-What? A New Mosquito-Borne Virus Lands In The U.S. At http://www.npr.org/blogs/health/2014/07/03/327760854/chikun-what-a-new-mosquito-borne-virus-lands-in-the-u-s
http://news.nationalgeographic.com/news/2014/07/140701-chikungunya-caribbean-mosquitoes-world-health/
For more on the Russian philosophy of disease ecology, by Evgenii Nikanorovich Pavlovsky (1884-1965), and A. Georgy Voronov, see:
—my thesis, Overview at http://wp.me/Puh6r-3HT, or full project and supplement chapters, not published except on the web, detailing the history of the medical geography and disease ecology fields, at http://oregontrailcholera.wordpress.com/
—my webpage and dedication to , "Zoonosis and Russian Medical Geography", at https://brianaltonenmph.com/gis/historical-disease-maps/zoonoses/
or, the following classical reference:
—Human Diseases with Natural Foci. (Abstract/Description for purchase) 1963. At: http://www.cabdirect.org/abstracts/19642702411.html;jsessionid=05B0F21042EF4956C63AE975AC35B36D
July 2, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on Ebola and the Present States of Surveillance

The Present States of Surveillance – the implementation of GIS and Remote Sensing in Spatial Epidemiology.
A Flowchart used to assign levels of engagement in the Medical GIS process.
Normal Ranks 1 to 9 (1=low; 9=high performance and success; 10 = ideal theoretically rank.
Status, in this illustration is almost 6. Although this score is based on interviews etc. analyses completed a half year ago These assignments are based on the forms of software/programming required for each step and its uses, i.e. presentation and/or utilization, levels of spatial math, spatial representation, and analytic tools/methods used. Note: last month’s second review demonstrated considerable progress.
Improvements in accuracy, presentability, complexity, dimensionality, utilization, and predictability are some of the major changes required for each step.
To effectively deal with Ebola, the higher end agencies are working close to levels 7 and 8, and testing at levels 8 and 9.
The circled level is where we need to be for outbreaks like those of Ebola and other foreign born emerging diseases. Research stations and facilities at major headquarters no doubt have these technologies in place. Where we are lacking is at the infrastructure level and the lack of engagement in upgrading our software and skillsets.
In some ways, this reminds critics of what happened due to the natural disasters we experienced over the recent years. There were a number events we were "unprepared for", resulting in limited recognition, delayed response, and inadequate long term follow up for these events .
The point here is that we should use cases like these as lessons, that very well could prepare us for a repeat in these same events next year, but with worse consequences.
This year’s spatial epidemiological events–ebola, chikungunya, polio in the Middle East, the polio-like condition in California, the measles outbreaks and other immunized diseases in the U.S., and most recently Whooping Cough (is mumps, rubella, or diphtheria next?)– demonstrate better systems should be put in in place at regional and local levels. These systems should match the level most of the better standard system in health care are at currently (Levels 6) and be able to progress rapidly to levels 7 and 8 (begin to employ NLCD, grid, DEM, RS, NIR, vector-NDWI, RADAR, LiDAR, live LS or equivalents), and even 9 (prediction/accurate risk assignment) for the most advanced.
The technology we need to accomplish this goal exists right now. Only human behaviors can be used to explain why Medical GIS, as a profession, has not reached its fullest potential.
Those companies and health care organizations that start right now will become the local Innovators and Supporters. Those that wait, but ultimately find a way in are Early Followers.
Which pack does your company or healthcare group belong to?
I am currently trying to document our participation and rate of implementation, including with this ANONYMOUS survey,
described at: https://brianaltonenmph.com/biostatistics/gis-in-the-workplace-survey/
and directly accessible at: https://www.surveymonkey.com/s/HZ7MH7Q
July 1, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on See the Terrifying ISIS Map Showing Its 5-Year Expansion Plan

For students into Government Security, Bioterrorism, Re-emerging Disease and Foreign Disease Migration, etc. , this is a nice demonstration of the value of maps . . . especially political maps.
These are two maps with almost an exact match!!! The question that leads me to is: Could they provide insights into the philosophy and history leading to ISIS and the ISIS objectives?
The top map depicts the goals of the Great Ottomon wars fought by Turks and supporters from the late 1600s to the early 1800s, on and off [ this more “lively source” is from
http://generalhelghast.deviantart.com/art/Greater-Ottoman-Empire-256901086 .]
.
The lower map depicts the long terms goals of the Islamic militant group ISIS, trying to produce a [re-]unified Caliphate Islam. [Source:
http://abcnews.go.com/International/terrifying-isis-map-showing-year-expansion-plan/story?id=24366850  ;].
Source: abcnews.go.com
Excerpts from the new ABC News article:
"The Islamic militant group currently marching across Iraq trying to seize territory in order to create an Islamic state has purportedly published a map showing their plans for the next five years.
The maps were widely shared on Twitter this weekend. They show parts of Africa, the Middle East, and even Europe shaded in black, to represent the territories that ISIS hopes will be part of its Sunni-run state.
ISIS stands for the Islamic State of Iraq and Syria, and is a militant group that currently has fighters in Syria and Iraq trying to seize territory."
MY OBSERVATION:
My initial query consisted of a plan to compare the ISIS plan with that of Adolph Hitler. But Hitler’s plan did not match the ISIS plan at all. [For Hitler, see the Life magazine version of this, from 1942, at
http://www.dailymail.co.uk/news/article-2032699/What-Nazis-invaded-America-Maps-published-1942-Life-issue-detailed-plans-Hitler-invasion-U-S.html ]
But then I noted the expected match to many of the medical conditions and behavior I tracked related to the Islamic lifestyle and Islamic belief system.
Reviewing the maps of the war, it was not a similarity I saw between these two maps, but more an exact match, except for the north western part of China the ISIS plans to [re-]capture.
July 1, 2014
Posted by Brian Altonen, MPH, MS under
Scoop.it
Comments Off on See the Terrifying ISIS Map Showing Its 5-Year Expansion Plan

A nice demonstration of the value of maps . . . .
Two Maps with almost an exact match!!! Could they provide insights into the philosophy and history leading to ISIS and the ISIS objectives?
The top map depicts the goals of the Great Ottomon wars fought by Turks and supporters from the late 1600s to the early 1800s, on and off [ this more “lively source” is from
http://generalhelghast.deviantart.com/art/Greater-Ottoman-Empire-256901086 .]
.
The lower map depicts the long terms goals of the Islamic militant group ISIS, trying to produce a [re-]unified Caliphate Islam. [Source:
http://abcnews.go.com/International/terrifying-isis-map-showing-year-expansion-plan/story?id=24366850 ].
Source: abcnews.go.com
My initial query consisted of a plan to compare the ISIS plan with that of Adolph Hitler. But Hitler’s plan did not match the ISIS plan at all. [For Hitler, see the Life magazine version of this, from 1942, at
http://www.dailymail.co.uk/news/article-2032699/What-Nazis-invaded-America-Maps-published-1942-Life-issue-detailed-plans-Hitler-invasion-U-S.html ]
But then I noted the expected match to many of the medical conditions and behavior I tracked related to the Islamic lifestyle and Islamic belief system.
Reviewing the maps of the war, it was not a similarity I saw between these two maps, but more an exact match, except for the north western part of China the ISIS plans to [re-]capture.


