The current Healthcare Management programs nationally have remained in this unfortunate state of limbo over the past decade. I make this statement based on a series of studies I performed in 2012, the results of a survey I posted for 3 years regarding GIS implementation by facilities and programs, and the current state of progress depicted by published Medical Geography articles.
There are some new processes underway, but in spite of their increasing number, not a single facility has emerged as the leader in this field. That is because all research groups involved remain in the experimental stage in their work.
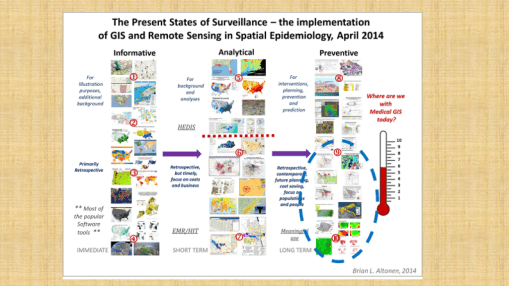
This is depicted in the above process defining flowchart I established around ten years ago, for scoring where a program of may be placed in my 1-10 scale for evaluating GIS-Remote-Sensing-Population Health levels of research, and applying GIS to health, at a large combined complete EMR database, and agency or corporation level.
Back in 2010/2012, some might recall I successfully mapped the entire United States using a national database of data related to 50 million – 120 million patients, depending upon the sets of data being analyzed, mostly focused on age-gender relationships and several thousand ICD groupings, for the most important ICDs in US health care.
In the more recent work, instead of size of population, I took advantage of a combination of population size and time details to evaluate care features. This allowed me to see relationships that exist between types of care, and the details of how patients and physicians engaged in that care. When considered together, the amount of care analysis reviewed at the total (gestault) level for care per patient, per healthcare problem, per personal health status, etc, ranged from just 1 to 21 years of care, with 1-16 years care as a better assumption, due to lack of completion of data entries per patient, at a per patient per year “continuous care” related level.
So, of about 12-16 million people reviewed, 50-120 M combined patient-years of data were reviewed. Multiple that value times 7 to get and estimate on the numbers of visits reviewed, and times 40-100 to get the total numbers of health care activities evaluated at the clinical level, minus the details, for whatever practice activities that physicians were engaged in.
With such a huge dataset evaluated during the recent stage of this work, a number of important types of studied emerged. These are some examples.
PROJECT 1
Epidemiological transition, amongst Religious Groups.
Goals:
- Develop general religious group maps of the region
- Develop three tables per group and gender: 2015, 2010, 2005
- Produce maps for specific health behaviors/ICDs/etc.
Major Groups:
- Non-committed (agnostic, atheistic)
- Muslim
- Jewish
- Asian/Cultural
- Christian (merge two subgroups)
- Natural Theologians
- Unknown (include?)


PROJECT 2
Recategorizing ICDs
Goal
Recategorize ICDs into well know subgroupings, and then develop newer categories for major comparisons
i.e. emergent vs non-emergent, chronic disease versus non-chronic, genomic/genetic related vs others
Steps:
- Produce tables of emergent vs non-emergent (with or without gender; replace gender binomial with E vs non-E. Perhaps relate to Race ethnicity religion groups
- Produce maps of the same
- Duplicate the first two for Chronic vs Acute
- Duplicate the steps 1, 2 and 3 for genomic and genetic/congenital, versus the rest
PROJECT 3
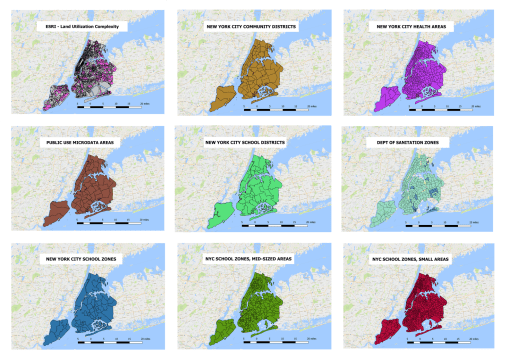
Applications of QGIS
Goal
Produce a variety of QGIS maps for the region, for different levels of data mining, restructuring, analysis and evaluations
Steps
- Demonstrate utility of this process across all forms of EMR data, including basic ICD, to Lab results, to risk related lab data features
- Produce maps of Height, Weight and BMI from data already pulled
- Reassess and remap for age-gender, add race-ethnicity-religion (RER) if time allows.
PROJECT 4
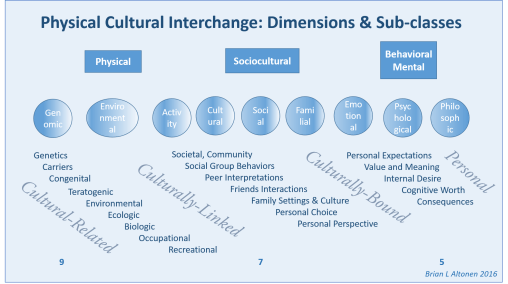
Cultural Ethnicity Influences
Goal
Identify Cultural-Ethnicity related ICDs of the four type previously defined by past studies (Cultural/Geographic Infectious disease and genetic), Culturally-linked (possibly genetic. systems related), culturally-bound (mostly behavioral health related), culturally-related (high risk due to race-ethnicity in the US).
Steps
- ICD analysis
- Groupings
- Tables and/or mapping