
Regional Health Planning and
the Pacific Northwest
Medical GIS and Regions series
.
Part I – Introduction
Part II – History
Part III – Examples
Part IV – the 3D Mapping LINK
Part V – Pacific Northwest Maps LINK
.
SUMMARY
For a review of this Pacific Northwest issue, see the following links:

During my years as a lecturer and chemical analyst in plant chemistry and the evolution of natural products (late 1980s to early 1990s), I had a number of friends with children who regularly skipped the immunizations recommended for their kids. Whenever I asked them about why they opted out, the same responses were given. One of the most frequent responses was that many feared there was an association between the Measles vaccine which contained a mercury salt and the onset of learning and behavioral disorders in children due to ADHD and Autism (see for article or brief note). Further discussion about the risks due to not immunizing were usually included as well, but the most typical response was that the infectious diseases these immunizations covered were now rare, and so the concern by parents about the likelihood of their child getting the disease was no longer common.
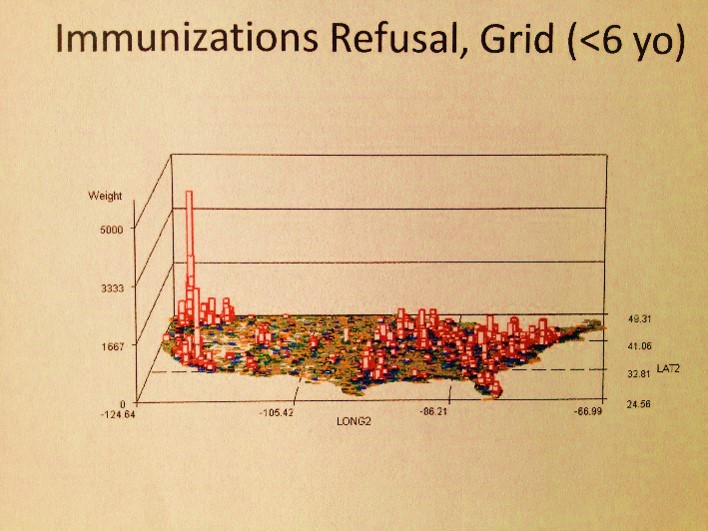
My 3D map depicting my findings in the Big Data
Another interesting group of individuals claimed that the natural onset of the disease itself was more valuable than the immunization process, for which the case of Chicken Pox was usually given as an example, but on occasion mumps and measles as well. Some of us may remember for example that during an outbreak of the chicken pox or measles during the 1960s and 1970s, our parents would get on the phone and converse with each other about the sick children and make plans to have a sleep over at the house where the infected kids resided. The purpose of this activity was to expose as many kids as possible who were not yet immunize to this same condition. These behaviors and beliefs are still shared today by even some of the most pro-allopathic mothers in the local communities. In the Pacific Northwest, many rural communities believe in practicing this small herd immunization philosophy due to their true communal nature, residing miles from “civilization”.
Applying this method to other diseases requiring childhood immunizations is not always beneficial. Such a process has also been used to expose children as well to such common diseases as mumps and roseola. Locally, in the Pacific Northwest, due to the rarity of some infectious diseases, I never heard much about these same behaviors taking place for diseases like rubella, diphtheria or poliomyelitis, but the same was not always true for whooping cough and pertussis. Any concerns out there about a child getting tetanus were often the least of these mother’s worries; the need for such an immunization rarely impacted whether or not a child went in for his or her well visits in some of the communal settings. Likewise, hepatitis B and Haemophilus influenza Type B vaccinations were often discouraged by the more naturally-minded, since it was expected that these diseases would be rare in low populated rural areas like the Pacific Northwest backroad communities.
The origins of this unique philosophy are interesting for the Pacific Northwest. In Oregon and Washington, there are numerous utopian groups residing in the farmlands and hinterland settings. These communities reside in regions where the roads have no names and the households or communal settings identified by just some numeric identifier for the newly laid dirt road and the number on the closest mile maker sign placed closest to the entrance to this place.
During my first several years residing in the Pacific Northwest, I had the opportunity to teach outdoor classes at some of these utopian communes or survivalist community settings. At least a few of these communes I knew rarely engaged in traditional well visit and immunization activities when caring for their children. I recall only one of them having an actual physician with an MD degree in charge of some on site health care program in the 1990s, and this commune was just a few miles southwest of the big city of Portland. Closer to Portland, there were also several families I befriended whose parents attended classes at either the local chiropractic, naturopathic or acupuncture schools. Not too unexpectedly, the mothers and children of these families were also not fully engaged in these programs. Likewise, for students who took my courses over the years in the University setting, I had some whose kids and grandkids appeared to adhere to these beliefs and behaviors as well, some of these mothers coming to take my class at the University residing as far north as Juneau, Alaska.
For this reason, it was a surprise for me to learn a number of years ago that the Pacific Northwest had better childhood immunization compliance than most other parts of this country according to at least one NCQA study for the year 2007 (link). This conflicted with my observations, leading me to suspect that those people I knew who avoided the immunization programs were just a very small portion of the local population.
Several years later, ca. 2002, I had the opportunity to test the prevalence of childhood immunization preventible diseases from a large population sample of this country while reviewing the state’s new database documenting the behavior of families in Oregon state. With this opportunity I developed a fairly detailed series of maps depicting the distributions of diseases that kids are normally immunized against. This was followed by a test of the frequency and distribution of V-codes used to indicate when and where parents refused specific immunizations for their children, with each immunization that is refused identified as a separate indicator. Five years later, this data was used to develop a new tool using a mapping program on a new XP system.
The maps that resulted from this work made me realize that there was an advantage to a detailed small area analysis of certain population health related features. You could immediately see the ways in which the Pacific Northwest differed from the reason of the country in terms of immunization refusals, but remained pretty much standard in terms of actual case development due to the lack of immunizations. The practice of immunizing and the mother’s decision to refuse to immunize are very different behaviors, each with a different set of underlying complications. Reviewing my maps I could tell that although refusals are at a peak in the Pacific Northwest, cases do not erupt more often in the Northwest due to these behaviors.
The best evidence for this lack of correlation is seen with the diphtheria cases and refusals. The peaks for each are completely unrelated, although suggesting of the possibility that refusals can sometimes make local rises in a normally rare infectious disease slightly greater than expected. The major factor preventing total immunizations is therefore probably not refusals to vaccinate or the development of a bad, inactive immunization program. This problem may be due to the in-migration of people yet to be vaccinated, whose children were not engaged in the US immunization programs due to a variety of lifestyle and cultural reasons.
This tells me that these maps are helpful because they indicate where outlier (communal) groups reside in the local community settings and where more aggressive intervention practices may need to be performed, and where the common intervention related activities we like to make use of probably will not work due to the ever-changing population. Due to in-migration and out-migration activities, at any time we could effectively immunize all the children residing in an area, and yet one year later find cases in which incomplete or total lack of immunization activities have taken place.
These maps have several layers of analysis that can be utilized, including raw data counts, n-squared and n-cubed models, and what I like to call relative independent prevalence rates. In addition, these maps were first developed as regional studies (based on HEDIS/NCQA defined regions, plus some), followed by state studies, zip code tract studies, and then finally square cell grid studies.
A number of presentible end products were developed with these results. The measured population health indicators pertain to infectious disease, cultural and socioeconomic diseases and related medical problems, sensitive social and sociocultural behavioral and psychological/psychiatric diagnoses and the like, and some very sensitive human and natural ecology indicators considered related to the disease migration habits for this country. ICDs, V-codes and E-codes were used to perform most of these analyses; HICLs and other codes were also on occasion employed.
Over the years, after nearly 15,000 runs, 1000 effective queries with solid, worthwhile results produced, some of which were repeated for multiple age groups, I was able to develop a better understanding of how to interpret population health, using a very effective method for mathematically engaging in these kinds of analyses. Of these analyses run over the years (some using very old, 10 to 15 year old data now, thanks to new software/hardware capabilities), about a third are worth reviewing and are covered in my blog (here and other pages). Of these, the following medical diagnoses, behaviors, conditions were found to have significant behavioral or independent prevalence differences within the Pacific Northwest (links to these will be posted in the last section of this page).
Primary Findings or Concerns:
- Immunizations (esp. Whooping cough, diphtheria, mumps, rubella, polio)
- 19-25 yo adult suicide
- Congenital Tuberculosis, but not Tuberculosis in general
Secondary, with highly prominent indicators of moral problems or social injustices
- Sexually abused adults (Portland) [and children?]
- Refused Care for religious reasons
- Infibulation
- Opium problems
- Crack Babies (Seattle)
- Fetal exposure to narcotics (Seattle, very small)
- Young Child Pedestrian Accidents [Seattle]
- Preteen Suicides (Seattle)
- Beriberi < 4 yo (Seattle cluster, small)
- Nutritional Marasmus (So. Oregon)
- Inadequate housing of less than 15 yos
- Off Road Recreational MVAs of children <13
- Young Child Pedestrian Accidents
- Desertion of Newborns, with Seattle more
- Low Birthweight Babies
- Child Neglect
- Child homelessness [mid-age to older childhood rearing problem]
Assorted Asian and Latino diseases
- Chiclero’s Ulcer
- Kuru Syndrome Peak at OR-WA border, well inland
- Takotsubo / Broken Heart Syndrome (half peak)
Other Categories/Concerns
- Mushroom growers Lung (notice peak is in Portland, not Seattle)
- Possibly Yellow Fever (north vs. south borders) – see Canada route(s) of entry due to reduced monitoring?
- El Tor Cholera – California (climate limitation? Astoria has natural ecology but wrong seasonal temperature patterns within the bay/harbor vibrio settings, excluding the oyster beds.)
- Obscure African Cardiomyopathy – Calif peak
- Machupo Virus Hemorrhagic Fever – Calif peak
- Takayasu’s Disease – Calif peak (interestingly, no other Hawaiian/Japanese diseases yet detected)
- Pinta- remains south for now (Calif peak)
- California Coccidiomycosis (Calif peak, however, may have a latitude-climate defined limiter of spread; counterargument=Amanita spp. did migrate north to OR between 1975 and 1985, so why not Coccidiomycosis?)
.
.
PART I
INTRODUCTION
What defines the health of a particular region?
There are several ways we can look at regional health.
- We can focus on the region as a physical entity and review its natural history, demographic history, and the history of its disease patterns.
- We can also be more specific in setting our goals and defining our methodology by focusing on the region as a spatial feature with a health that is defined by the various elements and forces of nature, such as climate and weather, temperature and humidity, soil and water, plants and animals, man and beast (environmental agents acting as pathogens), and how land use changes and changes in weather and populations have influenced the region temporally.
- Or, we can focus on the health of a region as a consequence of people first, nature second, time third, and place fourth, and then try to link these to where these events took place in history and on the earth, and how commerce, economy, poverty and success impact the physical and emotional health of a region, how regional differences can be used to define or predict where the least healthy survive, to better understand how and why some of the most domestic violence and psychiatric conditions exist in certain parts of the United States, and where the most turmoil is bound to happen regarding poverty and lifestyle, living habits and disease, emotions, socialization and progress or lack thereof, drug abuse and spouse abuse.
The last example is what defines this study of the Pacific Northwest as a specific region of the United States with specific health care offerings, wants and needs.
It is with this last interpretation that we are left with if the goal is to develop a realistic perspective on regional health patterns and disease, in particular for the Pacific Northwest. The Pacific Northwest is unlike any other part of the United States (see Wikipedia). It has connections to other countries and cultures that enable these people to influence what the Pacific Northwesterners do. The Pacific Northwest is rich in outdoor recreation areas, and has social groups that stimulate intellectual interests more than most “backwoods settings” in the United States. It has a variety of people with such differing viewpoints that the consequences of their beliefs and actions cannot help but hit the national news every now and then , such as during the late 1980s strike by lumbermen which resulted in the closure of downtown Portland by logging trucks, or the influences of overactive pacifists successfully interfering with a local meeting of major countries, or the attempts of Pacifists to stop whaling operations and Old Growth forest clear-cut operations in indescribable, often illegal ways.
.
Most urban settings have splits in the public opinion that can be used to define two socially different groups other than the expected rich versus poor, democrats versus republicans, blacks versus whites, rural versus urban families, indigenous or local natives versus non-indigenous or non-Pacific Northwest raised immigrants. Some urban settings have a special sociocultural need for these splits to form. In the Pacific Northwest, one example of this split involves the activities of groups like the alternative healers, for which there are purists who are against the combined or mixed allopathic-alternative healers, and the new age thinkers trying to obtain the rights to smoke marijuana or take some sort of alternative herbal recipe as part of their chronic disease regimen or cancer treatment plan. Some of these people in search for the cure are represented by the religiously bound, but since this is the Pacific Northwest, these religions may be non-traditional and consist of various metaphysical spiritualists, women healers, and scientifically minded atheists. But then there are those social Darwinian healers trying to eliminate selfishness and greed, emphasizing environmental sensitivity over capitalism, the lower class equality and socialism over a society run by a select few well clothed CEOs and upper middle class employees.
With health care, each of these social injustices are felt to exist by the Pacific Northwesterners, and in some cases it appears as though they do exist. What better way to say the upper middle class remains insensitive to society’s culture than to demonstrate how little the health care insurers and health care provider businesses provide full care to kids of the poor, who are barely able to maintain a good health, engage in preventive medical care, and receive the kind of care they need to engage in and be able to complete their most basic schooling requirements.
The health insured versus the non-health insured poses a serious question on the healthcare system right now in the Pacific Northwest. For decades this part of the country has had various forms of alternative care provided because the regular system will not cover or accept anything but the practices allowed by some of its industry’s major financial supporters. There are some programs offered by regular health care insurers that do allow “alternative” care to be provided as some form of complementary means for offering support to the client, and when such a practitioner is allowed, rarely do they allow such practices to convene that they believe will have an impact. Just in case these alternative forms of tratment work, these companies want the option of being able to enjoy to benefits of this success; their goal is not necessarily a healthier patient, just a patient who costs less to treat.
Health insurance companies much of the time allow patients to see chiropractors when the lower back pain needs such care. One can also go see an acupuncturist, usually for certain psychological medical conditions not for any conditions in need of changes in the flow of chi to assist in somatic healing process. Health insurance companies allow you to take your herbs, since of course they don’t have to pay for these, and for the time being realize that they cannot prevent such activities even when they fear it may result in increased costs later down the line, due to such complications as liver failure or kidney problems setting in due to the combinations of prescription drugs and OTC herbal medicines being utilized.
Part of the reason insurance companies behave this way is their limited knowledge base in anything other than allopathy and osteopathy. In cases where staff members are completely aware of the complexity of the alternative medical fields and their various theories for health and prevention, there is nothing these workers can do about any of this knowledge. The cost-benefits results capable of inducing such changes aren’t always there, ready to be cited.
In spite of all this resistance to non-allopathic care, the Pacific Northwest remains one of the regions where alternative care prevails more so than in any other part of this country. Now there are some places that are pretty cutting edge when it comes to implementing alternative care, but they are never regionally effective and so often have areas where the status quo prevails. New York City for example is full of alternative thinkers, as it has always been, but the local political prowess of the regular practitioners does everything possible, and effectively, to disallow alternatives from ever becoming a standard part of any health plan for most people. Likewise, parts of California have communities that would like to claim they lead in alternative medical thinking. The only problem is California has some kinds of alternative prevail less than the Pacific Northwest, having lost possession of the others through political means more than a half century ago. So even though California may seem ahead at times when it comes to new thinking and new philosophy, the legal system prevents California medicine from effectively becoming fully pro-non-allopathy when it comes to insuring all forms of health care. Income and the willingness of those covered by these insurance programs to pay for these services becomes the guiding principal for care options in most of California and the Pacific Southwest.
The one remaining feature of the Pacific Northwest that no other region can attest to is its production of licensed versions of an alternative doctor via schooling at accredited institution which do not exist in any other part of this country (for now). All other parts of the country that profess they have healers in naturopathy may also be promoting practitioners who are trained by non-accredited programs. The Naturopathic Doctor (ND) program with degrees offered in Oregon and Washington are four year full-time professional schooling, lab and classroom programs, not mailorder training methods that take place over two to four years, and which lack the accreditation needed for a degree worthy of coverage by some federally sponsored student loan program. There are two NDs or naturopathic doctors out there right now, the less of the two jeopardizes this profession as a whole, providing the opportunity needed by MD programs to develop some form of substitute for NDs, someone trained in the allopathic interpretations of the various forms of “alternative medicine”.
These features of alternative or complementary medicine in the Pacific Northwest also help define the individuality and uniqueness of its citizens. They define how the status quo view the health and well-being of its population, which in turn relates to how companies, organizations and societies play a role in how people make personal health decisions, how they chose their physicians, what medical philosophies they will be most supportive of, what types of doctors and healers they want to see, and what kind of lifestyle each individual is going to live in terms of diet, recreation, selecting medications, or engaging in prevention and cure health care practices. By focusing on people as their own causes for their health and disease, versus assigning natural causes for health and disease, a method often relied upon by medicine and blaming the victim for poor health, we are provided with a different point of view to use for defining the sociological causes for poor health produced by the health care system and its insensitivity to new thought and personal wants and needs. One major reason fo rthe failure of the new systems being developed in health insurance will be linked to the inability of these companies to have the intellect and understanding needed to encourage more involvement of these non-allopathic options. There is a cost benefit that can be achieved by engaging in such a task, but more than likely the insurers will remain far behind when it comes to understanding the medicine wished for and needed by the poor and underpriviledged, as well as the regularly employed middle class citizen with an open mind. Health care insurers that lack the dexterity needed to understand and allow the philosophies of Chinese medicine, unaniism, indigenous philosophy and quantum physics to be a part of the philosophy of someone’s search for health, will most likely fail to meet the needs of the percentage of their members/patients in need of such care. Such a mindset by the health insurance company represents a lack of compassion for its members, at least when interpreted from the side of the insured–namely the medicaid, medicare and low and middle class income people in need of these more human forms of health care.
With the alternative approach to interpreting disease patterns and behaviors, one can change the sourse of the disease and its chronicity and longevity. For example, in some forms of alternative medical psychology traditions, we are taught that it is not the foodways and nutrition stores that give us Type II diabetes, rather, it is the behaviors that we engage in, the reason why we engage in these behaviors, the mindset we are in that leads us to participate in them, and the way that we decide to deal with the related problems or conditions, such as physically, cognitively, emotionally, metaphysically (spiritually), or in terms of prevention, maintenance and long term self-imposed/decided care management mechanisms (i.e. allopathy and/or not?). There is this “outside the box” approach (or in the minds of Pete Seeger and Woody Guthrie ‘outside the little boxes/houses’) to socially and culturally defining people we respond to changes in their health status that makes up the other forms of health care out there. It is often the fact that cases of special need exist due to other underlying features like poverty, a poor living environment, poor sanitation, malnutrition. Asthma, for example, is not just environmentally induced. There are the daily stresses of life to contend with in combination with the kind of environment one is living in that can help induce asthma related illnesses. Poor inadequate housing within turn of the century homes for example, make for unhealthy environments where children breath in dust, dander and asbestos from nearly a century ago, along with the typical pollutants and pollen found in low income neighborhoods. Together, these lead to conditions like allergies and asthma, COPD and bronchiolitis, allergic bronchitis and upper respiratory infections.
Likewise, the common sharing of Chlamydia during the young adult years is in part a consequence of poor health behavior choices, but also a consequence of poor housing arrangements, unhealthy street life being initiated and promoted by others, and the form of promiscuity that develop in these settings to ward off depression and thoughts of suicide. These social and physical “diseases” develop in part due to the mindset of the victims, but equally so if not more due to a lack of concern on behalf of the general public about putting more money into supporting new public health programs. In the Bill Moyers series on cancer in women from more than a decade ago, the art therapy worked on the patients he interviewed, due to a mindset and a change in life’s behaviors and practices. Why are the health insurance agencies so much against such improvements? Why does who has some sort of Chronic Disease only have one choice to make, which is to conform, get old and usually become sicker but maintain a decent quality of life?

Back in 1990, while on a Trimet bus traveling west along Burnside, I can remember a very well dressed businessman wearing a top of the line suit talking with his business partner about a meeting they were going to. After passing by the lines of people leaning against the walls at both ends of the Burnside bridge, he took a break from his logic to comment about the line of people standing all along the bridge, claiming it to be an eyesore and then suggesting these people and their services be moved to a place outside the downtown area. This way all of their services could be merged into a single program, and provide everything needed by the homeless and unemployed in one place.
Immediately following his comment you could tell by the expressions on peoples’ faces that his comments weren’t well received. This behavior is an indicator of the insensitivity the rich continue to be have towards the poor. The truth was many of the people on this bus resided in low income neighborhoods, and it was their main means of transportation to the downtown area for work, or street life. The businessman simply assumed that all homeless people do not work, or try to find work, and that those in need of charities or additional financial assistance were an eyesore to him and his colleagues. This issue of inequality has prevailed for decades within urban settings, and takes place whenever the poor and underprivileged are adjacent to the middle and upper class as part of their day to day life experience, but yet the two by habit rarely interact.
In reality, it appears there is little we can do to better the health of a community besides provide the facilities needed along with the resources and money needed to better the health of the poorest people for any given area. But even this is rarely accomplished, and designing plans that are meant mostly to work from the top down to accomplish this task just doesn’t work. In other words, spending a lot of money to develop a large or centralized service agency doesn’t offer much in terms of true help. In reality, back on board that Burnside bus, the person who made this statement deep down probably knew this, and/or just didn’t care.
In 1992, with the recent opening of a Conference center in Portland came an ADA conference that was being duplicated around the country. ADA was then very new and this was an attempt to display to the general public it’s first accomplishments. This convention was open to the public, and when the public attended and went to the special sessions, some of these sessions resulted mostly in vocalizations of dissatisfaction, not just with the system in general, but with the apparent insensitivity presenters were displaying to the public at large. One session for example was run by a fairly elite npo that offered its services to people on Long Island, a place where travel other than local is almost impossible for anyone with a disability. Their service didn’t seem to meet any unique needs according to some and since their office wasn’t open to the public, and their services primarily devoted to the information found on a pamphlet that could be mailed, this process seemed highly reiterative of the various other services already out there. This irritated the disabled attending this session to no end. The three presenting appeared well-dressed and were very out of touch with the lower class. As a result people began walking out about half way through this session. If one were to look up the income of this npo at a later date, we might find that very little of the money earned by this one-million plus per year agency went to the people, except in writing by mail. The message presented here to many of us was that these agencies exist as sources of employment for the middle class, funded by taxpayer dollars, and not at all for helping to employ the “disabled” lower class.

As a victim and survivor of both ends of this chain separating the rich and the poor, I find that some features of human behavior are present in all urban settings, where rich and poor communities are commonplace. Others have their unique qualities and effects on the overall regional population health. This is due to culture, ethnicity, race, breed, color, language, philosophical and intellectual differences. Such behaviors are also capable of turning any problem experienced within this setting into a social disease that is endemic in places where the poor ultimately influence the rich, and vice versa.
The way these two social groups collide is indirectly and through financial and monetary imbalance, funneled in due to health and disease imbalance. When the poor become sick, the rich unknowingly also suffer, first through infrastructure requirements and taxes, then through the sickness afflicting members of their family. For example, AIDs came to be when I was attending my first year of medical school. The local news about this disease was that it was unique to just one culture (not homosexual), one ethnic group. This condition still had no name when it was presented by the chief pathologist of my school teaching the pathology course. Unknowingly, my mentor at the time, who was also a legal spokesperson for the school, was being asked to lay the blame on this particular ethnic group, potentially resulting in the same being shared with the news. He refused, and quite soonafter retired from his position in early 1986 (all of this is told in an autobiographical article he wrote and had published in Milbank Quarterly, 1989/1990).
Healthy communities require just healthy people, not some healthy people supporting the health care needs of the unhealthy. What makes the Pacific Northwest so different is how and where the members of their community make their way into this setting. Each region of the United States has its own particular sets of people, cultures, medical beliefs, traditions and disease. These influence the quality of life a given region has, and the necessities required for maintaining a healthy state if and when it exists. The economic differences between the rich and the poor result in lifestyles that are led along different paths by these two groups. this means that there probably has to be separate methods and logic attached to how these two groups are managed and treated. A standard set of rules have to be developed that allow culture to play it due role in making people healthier, even if this means producing a new form of integrative medicine.
.
PART II
History
Before I went into the study of public health, I was a part of the low income community health scene in Portland, Oregon. I spent hours a day “observing the local urban environment” we like to call it, wandering local parks, sitting on park benches, watching the walkers and joggers pass by, conversing with other homeless people, socializing with members from various other homeless social scenes. One of these scenes consisted of a group of people devoted to “alternative medicine”. It included believers in everything from the most basic forms of herbalism and astrology, to the most archaic, rarely discussed forms of wicca and garden fairies, physiognomy and spiritual counseling, meditating and connecting with past lives. On occasion I was active in the pop culture and npo scenes for some of these groups, but for the most part by the late 1980s I was satisfied working as a researcher of plant chemistry at the local university, where I also served as a contracted lecturer specializing in plant taxonomy, medicine and pharmacology.
Throughout all of this, aside from receiving some income for teaching, I lived as a part time recipient of one of the largest state and federal programs out there for the low income, disabled population–the local State Welfare program and the related Supplemental Security Income program. This change in life for me was due to a worsening form of epilepsy I was experiencing since my early teen years (TLE or CPS). By the end of 1986, at the age of 29, I was dismissed from my position as a student of a regular medical school in New York due to this medical history. ADA did not exist then and the professors, deans and administrators had various opinions about whether the disabled could learn all the skills needed to be a physician. Until a medical school was willing to allow a blind student to learn and practice medicine (i.e. a friend of mine who suffered the same prejudice), even though only some parts of the field could be engaged in by him/her, these same insecurities were going to allow medical school administrators to claim that law and patient’s ethics had to rule over any disabled student’s rights for any student with epilepsy learning to be a doctor.
A half year or so later, after being given a year’s leave from the MD program, I became a patient in one of the largest health care programs out there in this country–the Oregon Medicaid program. I had a choice to make–I could spend my year off in Oregon getting better care for my seizures, only to have to return to New York once my year off from school was finished, or I could stay in Portland, Oregon to get the kind of care that I needed. I therefore resigned from medical school in January 1986, after three plus years in the program, in order to get a new form of care for epilepsy offered in only a handful of places around the country. My hope was to make it through this regimen and re-enter medical school much later once my seizure problem was tended to.
From 1986 to 1995, due to the Federal guidelines for Medicaid recipients, I was pretty much resolved to teaching classes on a per contract basis at a local university. This meant I had to report to the local SSI office all activities I was engaged in that generated income coming in from the State University teaching setting. I spent most of my working time at this university in a lab provided to me for work as a plant chemist and researcher of plant medicine. My areas of focus were developed due to more than 9 years of pre-med and medical school experience back east, and my interest in perscription drugs derived from plants ever since my pre-med freshman year in 1976, and this course I took from Adrien Albert with a topic in it called selective toxicity (toxin vs. medicine). During my Portland years beginning in 1986, I carried this knowledge further by studying the chemistry of plants in the lab as it related to their uses in medicine and anthropology and plant taxonomy. This enabled me to develop a book and course focused on the evolution of natural products (plant chemicals) by 1990, filled with valuable information on the related studies of medical botany and ethnobotany.
As a part of my class I also reviewed topics being taught locally at two of the non-allopathic schools. I taught my students that Portland, Oregon was/is the only urban setting in this country with licensed, accredited physicians for the following four distinct forms: allopathic, chiropractic, naturopathic, and traditional chinese medicine/acupuncture. To understand why this is the case, I spent the next twenty years researching and teaching the history of alternative medicine and medical licensure and accreditation.

source: my blog at Naturopathy Chronology
The truth is Portland is the only place in this country where naturopathy has been kept alive as a profession since the late 1950s, the period which immediately followed a series of attacks made on alternative medicine in general. Once the remaining licensed and accredited Eclectic and Homeopathy physicians had retired medicine, their professions began to fizzle out enabling naturopathy to serve as their replacement. These 1950s events also marked the end of a period when the last homeopathic institutions and hospitals (also in Portland) were finally closed down, after more than a century of successful but repeatedly unstable periods of operation.
Aside from the politics of medicine, there was also the growth of new medical industries getting in the way of the growth of alternatives like naturopathy. This was a time when soldiers returning from war (the Korean War) had a variety of medical sciences to consider for future careers. Such opportunities led many of soldiers to apply for the federal assistance offered to cover educational costs related. The alternative medical curriculums also took the opportunity to mention these offers, although very few of those who served in the military opted to take on an profession outside the allopathic realm. In the general sense of things, to the soldier this form of medicine made limited use of the new technologies, and therefore seemed too immasculine one might say.
“All naturopathic students recognized by the Veterans Administration for training under P.L. 550 will be granted $90 a year scholarship.”
“Beginning this Autumn 1959, the College offers for the first time a course specially designed for Christian Missionaries. The training period is nine moths, two semesters of four and one half months, totaling 1116 class hours to a Certificate of Technician of Naturopathic Missionary Medicine.”
It was the closure of these naturopathic schools in California, New Mexico, Texas, and other states during this time that led to the recirculation of old library holdings from these alternative schools to new locations for continued use. The Naturopathy school in Portland is where these documents ended up. As this Portland School became the seat of the original writings of numerous practices and philosophies, elsewhere these teachings were never heard about again. Included in this collection was a scarce document detailing the results of two Utah state-sponsored studies, a preliminary and subsequent complete review (type ‘Utah’ for entry onto this summary page) on naturopathy and other forms of alternative medicine between 1955 and 1958, which provided us some of the most important clues to the period of transition that took place between 1945 and the late 1950s in this period of medical history. With this document we can better understand why medicine in the Pacific Northwest is what it is today–a profession primarily allopathic but with some of the most unique social and sociocultural medical settings and offerings in the nation.

source: my blog at Naturopathy Chronology
As medicine became “drugless” during the early to mid-1900s, chiropractors took to nutritional/dietary products for treating their patients, and the rest, the naturopaths, turned mostly to nutrition and diet, exercise and sports, and the use of herbal remedies (see enrollment data extracted from Utah study at Utah Naturopathic Physicians Survey, 1957) Naturopathy students were taught numerous philosophies related to health and disease, including physiotherapy, nutrition therapy, massage therapy, herbalism, and a variety of historical alternative health related beliefs related to Thomsonianism, eclectic medicine, physiomedicine, hydrotherapy, homeopathy, acupuncture, traditional chinese herbal medicine and meditation [note: some comparative course listings for the ND programs, still in need of clean up, are at my blog pages entitled Draft of First Catalogue, Program Comparisons and one on the John Bastyr College, the result of a 1970s political division in the sect internally by the branch of NCNM operating in Seattle (enter with ‘Bastyr’)].
During the late 1940s/early 1950s, government and allopathic offices and groups approached the “drugless” or “mixed” chiropractic-drugless (naturopathic) school in Portland and threatened loss of accreditation due to a dispensing of “medications” by the non-chiropractors. (Until the mid 1960s, some medicines like digitalis could only be dispensed in herbal form, causing a problem with the idea of a drugless medicine being practiced when strongly toxic herbs were involved, but there were other reasons as well pertaining to classification of immunizations as a ‘drug’ that cannot be administered by ‘drugless’ doctors.) As a result, the mixed medical school stopped providing classes to naturopathic students. forcing them to turn to private schooling in small lecture hall and home settings throughout the remaining 1940s and part of the 1950s (I have a communication on this from this period in Naturopathic history, still to be posted.) In 1957, the National College of Naturopathic Medicine was opened, which has since become the most important school in this profession’s history. All other schools operating during the time of the Utah study in 1955/6 were subsequently closed.
On and off since the 1960s, the reputations these schools have had have been controversial and highly opinionated. There was a tremendous amount of biasness in fact used to evaluate these programs. These evaluations came from MD graduates and especially leaders of the MD profession, most of whom had no opportunities and spent no time attending these ND programs. When they did, there was a certain amount of prejudice already present when they attended such classes or public lectures made available on the profession of Naturopathy. In addition, there were those events that were borderline in terms of professionalism, to put it bluntly. The presenters did at time lack the knowledge base seen with their MD counterparts in certain argumentative situations, due mainly to the program itself and the nature of their profession. But the same could be argued for MDs, who had little to absolutely no understanding of some of the practices engaged in by the alternative clinicians, able to recognize, understand and regurgitate an endorphin or interferon theory for the way acupuncture works but turn to a century old out-of-date response utilizing the term “quackery” to argue situations for which they had no training or clinical background. (Such blindness, at both ends, is often the case in this ongoing argument.)
Within this same school, “drugless medicine” had numerous teachers trying to preach that immunizations were bad for you, that chemical medicines were bad and herbal medicines and homeopathic formulas healthy, that the old adage of puke, purge and sweat was as true now as ever before, that poor diet made you weak and gave you cancer everywhere in your body, or that bad health was rarely if at all due to microorganisms, in particular such a thing as the bacteria.

Understanding the local history of NCNM, the local Chiropractic College, and OCOM provides some insights into the practice of medicine as a regionally defined cultural attribute, but this still doesn’t tell us much about how and why these events happen and why they become so successful. This information comes by researching the past, and in many ways it ends up, the Willamette Valley and Portland is much like the Hudson Valley region in New York. There are a number of physiographic, demographic, cultural and medical/historical events that helped form these new healing faiths in both of these well populated valley settings. Distance from the leaders of the field at large was important, but only a part of this picture as to what enabled the non-allopaths to become so successful in such a region.
A better understanding of how and why people in general turn to non-allopaths came to me when I began my studies of Oregon Trail medicine in 1993. I had finally completed the Dr. Osborn research and was searching for a new topic, when I came upon a similar recipe book penned by Illinois-Oregon trail-Oregon State physician John Kennedy Bristow. That led me to researching the various alternative forms of medicine of the early 19th century, eventually leading me back east to determine why and where many of these beliefs were born.

How and Why these CAM practices, as a collective, are mostly a Western Phenomenon. The above is perhaps a fairly simplified map of the migration of complementary/alternative medicine [CAM] across the U.S. The earliest, primary routes of medicine philosophy in general follow any and all of the above trails indicated, with regular medicine, trapper medicine and perhaps “Indian Root Doctoring” philosophy travelling these routes as well. The migration of the sanative philosophy of Thomsonian is most important. It was accompanied by the trancendentalists like Oregon’s early physician John McLoughlin, and was followed by physicians of a distinctly new and different philosophy known as homeopathy (also sanative), some of whom no less were Swedenborgians. Physiomedicine is a unique derivative of Thomsonianism, its beliefs are more sanative and are mostly born out of Bible Belt traditions. This practice was spread to Oregon in 1852 due to John Kennedy Bristow and his teacher, Reverend Edmund G. Browning from Adams County, IL a year after the devastating cholera epidemic struck again. (Also related to this is the history of this sect along the Mississippi as per Bristow’s Uncle Michael Gabbert who was a physician and published historian out of Memphis, TN). Eclectic medicine, being derived from all of the faiths, followed all of these routes of migration after 1850. The hydropaths (water cure, nutrition and sanitation medicine practiced by ladies) and spirit rappers made their way westward during this time as well. There was also a tremendous amount of California-Pacific Northwest interaction ensuing from the 1850s into the early 1900s (red arrows). Much of contemporary non-allopathic medicine during the early 20th century survived in the Pacific Southwest region (but esp. CA, CO and NM), making it from the west coast and southward perhaps from Kansas between 1900 and 1930, filling parts of the US between Texas and Illinois, and Texas and California. Relatively speaking, the Seattle Naturopathic school is a very late addition to all of this history (dark red line); prior to its current independent ownership, it was initiated along with Portland NCNM ca. 1956 (due to Vancouver, BC influence), finally becoming its own institution during the late 1970s.
My first important discovery was made when I realized that many of the local pioneers learned the medicine of the Hudson Valley and/or upstate New York (“the burned over district”), either directly from New York or as Midwesterners of first and second generation descent from New York families and healers. This meant that the non-allopathic medical beliefs of the east coast had followed the trails leading from various parts of the Valley up to Troy, NY, and from there to Ohio and then Indiana and Illinois, and then directly across the country by overland routes leading to the western shores of California, Oregon and Washington. Likewise, the books written on these medical fields or faiths made their way along similar routes, many ending up in city library collections as donations or as part of the boxes of books being disposed of through local bookstores by individuals who descended from these pioneers of six or seven generations before. (Interestingly, a significant number of these books came specifically from one publisher, Orson Fowler of New York City, someone famous for his work in phrenology and whose estate I later found out I grew up upon.)
Ironically, I was also on my own quest for knowledge about my health during this time. Due to my income status, I often found myself having to rely upon such things as Baloney Joe’s and other local soup kitchens for meals, and the Medicaid health care program for my health needs. (There are a number of agencies/npos familiar with, and articles written about, my foraging for food in the parks as well.) All of this personal history had attached to it a medical history of epilepsy. This greatly impacted by progress as a student in the school of medicine back east due to prejudices and uncertainties existing on behalf of the academic administrators. It was 1982 to 1984, and ADA had yet to be born. This left open the many options administrators and professors had to select from when dealing with my seizure history. One former classmate in this school of medicine (now my own personal MD) very recently told me the problem I had was like being branded with “a Scarlet letter.” My requests for how to deal with a seizure history and the medical schools’ administrators’ methods of managing my care were completely different. In the end that led me to search elsewhere for more advanced therapies for my seizure problem, not offered by my medical school. The much needed treatment unexpectedly came my way in just a few months, and was quite a success three years later.
Now living in the Pacific Northwest, I followed up my study of medicine back east with the continuation of my lab and teaching position, several attempts to return to medical school which were unsuccessful, and finally my studies of medical geography and public health in my northwest university setting. With more than 15 years of Social Services-Welfare-Medicaid-Section 8 experience, I decided my focus would be on specific topics related to my own experiences, ‘five or ten years from now, once I can return to college’ I used to tell myself. My population health studies now focus on social inequality, poverty, infectious diseases and other moral issues related to people’s physical, emotional, psychological, metaphysical and sociocultural health, my goal was to produce/find the best sets of data or statistics pertaining to the hardest diseases and diagnoses available for analysis and review.
My readings of the philosophies of physicians from the 17th to early 19th century during those years made me aware of the ways in which we interpret health, medicine, disease, and “cures”, and the notion of being “healthy” versus being “ill.” For this reason, there are several approaches I learned to take when reviewing regional health, keeping in mind the ways in which these disease get treated or result in refusals of care and signs of public discontent are defined by the unique sociocultural history of Pacific Northwest medical practices and beliefs:
The first is to look at the disease patterns and how they are distributed between regions.
The second is how age-gender-culture differences differ between regions and how these features impact how diseases erupt in some regions more than others.
The third is how these two features together define the niduses or centers for diseases locally, be these diseases physical in nature, genetic and therefore pretty much inevitable in terms of cause and form, or psychological in nature, mental health related, income and socially based, and/or related to local sociocultural circumstances, each of these making them behavioral, emotional and even neodarwinian in terms of origins and development.
Based mostly upon the above experiences at the receiving end of health care, followed by a period of intense public health focused educational activities, I have come to the conclusion that a number of important features of the Pacific Northwest influenced the way public health evolved in this region and how these health care changes are now continuing to occur and either improving or lessening the benefits of typical health care programs in the Pacific Northwest for the next decade or two. Some of these features were included in a Healthy People 2010 project engaged in several years ago. Many of these goals are offshoots of previous concepts that already exist and relate strongly to the Pacific Northwest.
However, there are several unique features about the Pacific Northwest and Northwestern lifestyles in general that impact the ways in which medicine is practiced and how certain diseases or medical conditions are treated and “cured” in the Pacific Northwest. In related reviews of medicine in Portland I engaged in, my focus was not only on disease ecology and the environment but also turned to trying to understand how the Northwest came to develop these unique healing faiths and practices. In particular I was interested in the locally licensed and accredited practices of Naturopathy (esp. herbalism) and Traditional Chinese Medicine (TCM). Both were being incorporated into some local heath care insurance programs, along with already accepted and accredited practices such as “sports medicine”, physical therapy (an alternative until the 1960s), podiatry (renamed as such from chiropody thereby allowing for licensure and accreditation in the early 1960s), and osteopathy (DO practitioners of which have most of the same clinical and surgical privileges as an MD).

Photographer Doug Beghtel/The Oregonian. Article’s author: Andy Dworkin. ”New Clinic Opens at Portland College of Natural Medicine.” Published: Wednesday, September 30, 2009. Subtext for photo: “Students Tim Rudowsky (left) and Matt Elliott weigh and mix kun bu, or medicinal kelp, and other Chinese healing herbs in the medicinary of the new clinic at Portland’s National College of Natural Medicine.” Accessed on 3-25-2011 at http://www.oregonlive.com/health/index.ssf/2009/09/new_clinic_opens_at.html.
Due to the tendency for non-allopathic practices and beliefs to greatly influence patients on Medicare, Medicaid and CHIP programs, these behaviors have the potential for meeting the demands in medical care by special needs populations. In some cases, their implementation can have the effect of reducing the overall costs for care, and/or improving the long term outcomes and quality of life for patients. For this reason, I took a closer look at what kinds of social and behavior-related problems impact the Pacific Northwest specifically in relation to the local alternative or complementary medicine culture. Now more than ten years into this project, my review has led me to draw the following conclusions, suppositions and/or findings:
- The Pacific Northwest is located a fair distance from “the status quo” on the East Coast, and even southern California or the Midwest. This enables different mindsets to evolve and different personal, family and cultural traditions to form in the Pacific Northwest, beliefs that don’t exist as much in other parts of the country.
- The Pacific Northwest offers its own environmental setting, to which certain natural philosophies are attached. The environment of the Pacific Northwest is in general “more rugged”, and involves a younger, less inhabited post-colonial region. It subsequently has more traditions that are still active in society, many of which relate to indigenous and pre-settlement history.
- The Pacific Northwest is a part of the Pacific Rim, and has domestic (family-based), social, cultural, legal, economic and political attachments to other parts of the world. This enables international and intercultural relationships to develop and persist, relationships that don’t normally exist to such an extent in other parts of the country, save perhaps for some parts of the southern Pacific Coastline.
- The Pacific Northwest differs from the Pacific Southwest mainly in terms of climate and culture, with the warmer California region placed quite close to Middle America and especially Mexico having unique impacts on the Southwest that slowly migrate northerly and exert delayed although sometimes considerable impacts on the Pacific Northwest.
- The Pacific Northwest has its most direct connections to the people and the colder climate settings of Western Canada (Vancouver and British Columbia) and the Alaska-eastern Russia border. This provides it with cultural and physical opportunities not seen in the Southwest, much less elsewhere in the United States. According to the past president of the Oregon Naturopathic licensure organization, this is also the major reason naturopathy remained alive as an accredited, licensed medical profession in the Pacific Northwest during the 1960s and 1970s.
- The Pacific Northwest has connections to overseas cultures and countries that facilitate in-migration of knowledge, lifestyle and unfortunately disease. Many of these may be absent from other parts of the country for geographic and transportation related reasons. This international cultural and commercial connectivity allows for the transoceanic migration of everything from new medical discoveries, to changes in therapy, modifications in lifestyle and disease patterns, and whatever decisions have to be made in terms of defining the needs of the Pacific Northwest when it comes to meeting the regional medical needs and the being equipped and ready for managing the right kinds of changes in local regional public health and disease patterns.
- The Pacific Northwest, due to reduced east coast “status quo” influences, increased Pacific Rim international and cross cultural influences, increased Canadian, Russian, and to a lesser extent Mexican and other Pacific Rim influences, allows for different foodways and alternative, complementary, or in the best of circumstances, integrative medical practices to develop and evolve in this setting. We see this in the different forms of medicine being practiced in this region, over time as well as presently, and by researching the history of these changes, have the potential of knowing and predicting just how much these practices will be engaged in by the public in the future.
- The Pacific Northwest has a history that remains alive and active, thereby enabling the influences of past traditions to emerge and re-emerge repeatedly throughout future generations. These influences have the potential of making some chronic diseases more prevalent, more treatable, more manageable, and more curable, either in substance or in terms of quality of life. The two chief ways that these influences take place is through the popular culture circuit with such quarterly trade magazines as Reflections offering information on the various healers and programs out there, and through the non-allopathic schools that exist in this regions, which aside from MD, DC, ND, and L.Ac./TCM include LMT and most of the traditional nursing and missionary school options.
I base these statements on a variety of personal and professional experiences due to residing in the Portland area setting, both on the street and off. The following are examples of studies I was engaged in while developing my skills in medical geography and public health once I returned to college as a student rather than a lecturer in 1996.
.
PART III
Examples

http://www.pdx.edu/prc/mapping accessed 9-1-2012
Mapping Social Inequality. The primary theme for most public health programs is social inequality. Even when schools are focused on inequality secondary to a major topic such as health education, policy, epidemiology, geriatrics, urban development, or environmental sciences, the difference that exists between the rich and poor always becomes a major theme in a well balanced health education program. Social inequality is the primary reason many studies exist in today’s academic world. Social inequality is also a topic that has been around since the beginning of the first handwritten iconographs and words.
If we take a look at the Portland Urban setting we can try to draw relationships between poverty and exposure to toxic waste and carcinogens. The common theme such work begins with states that the lower income people are more likely to be exposed to hazardous living environments due to their inability to afford more highly appreciated, untouched virgin properties, places where few if any businesses have effectively diminished the natural, ecological value of the living space. The idea that due to poverty, the living areas for the poor become unhealthy, and in turn due to poverty poor, unsanitary lifestyles begin to dominate within these community settings, and due to poverty and its impact on cultural and personal strengths people in turn do less to improve upon these now highly unhealthy living spaces, resulting in criminal activity and further perpetuation of poverty promoting lifestyles and living practices, is the single most common theme found for most studies engaged in trying to relate income and poverty to overall regional or neighborhood health.

Poverty stricken areas based on the map available at http://www.pdx.edu/prc/mapping , thanks to the Portland Population Research Center (http://www.pdx.edu/prc/home); areas with >20% Poverty were redrawn from the 2009 estimates and overlain in light yellow.
Portland has its North and Northeast sectors for example where the poverty prevails. Both of these regions are typically associated with non-caucasian residents who have middle to low income employment and/or unemployment histories. The Northwesternmost portion of the Northern Portland Area also has the largest amount of chemical waste produced and released or spilled for this metropolitan area, including accidental releases by some of the most unhealthiest of chemical industry settings. When when we review the distribution of cases within the urban setting, we don’t see a link between the forms of cancer evaluated for this work and the low income areas according to the 2009 population estimates posted by the Population Research Center. This theme continues with more specific spatial studies of chemical release and potential exposure.

A more highly detailed study I performed of this urban setting demonstrated better evidence for a possible association between poverty and the onset of cancer for the types evaluated when a small area grid mapping technique was applied (covered extensively elsewhere on this site). In the following images, the blue points (dots) are cases, the grid cell colors are red for the most toxic areas, and the pink areas are the regions defined as having greater than 20% poverty in 2009. (A numerically based nearest neighbor statistical evaluation of this relationship has yet to be performed.)

Hexagonal grid maps demonstrating the relationship between grid areas, numbers of cases, and chemical complexity of that area related to the state’s toxic release inventory data. The top row of 3 maps has polygons for the very poor shaded in pink; the lower rendering is identical except it lacks the filled pattern.
.

Mapping Regional Health Care Access. Access to health care has a number of geographic features that help to decide the ways for communities to receive the most appropriate care. The state of Oregon in general has several major topographic features restricting the means by which people can travel to where ever their care is being provided. In my study of cancer cases in relation to chemical release, the above divisions in property were chosen to serve as research areas. They were defined based on the distribution of cases, with boundaries selected based on a combination of population density features, major topographic features, and work/care-related travel options such as time and distance between the centroids or closest economic center of major regions. Government-defined county, township, census, and voting region boundaries were evaluated for this work as well, but its was zip code tracts that offered the most reliable, static data sets.
Later reviews of these research areas demonstrated significant cultural differences between neighboring regions as well in many cases. The most important and significant difference between these research areas is found when we compare Willamette Valley with Jackson-Josephine. Situated at opposite ends of the river valley, the northernmost urban setting has many of the features expected for urban settings with regard to public health related issues. Substantial funding exists for the Willamette Valley research area, versus the very limited funding and services that exist within the southernmost, warmer climate rural settings that produce most of the Jackson-Josephine research area. Both of these research areas have considerable populations, but according to many individual familiar with the Naturopathy profession and its politics, within the Josephine-Jackson area we find a considerable amount of interplay between physicians who practice as alternative, complementary or integrative medicine physicians, which contrasts with the social scenes engaged in by regular MDs who work in this area. (There were a few MD-ND’s down here as well!) In general, this area is where the “personality differences” between these two types of doctors are accentuated as well, with the non-MDs tending to serve mostly low income rural communities, but residing just across the border in California, versus the MDs residing within the state of Oregon and serving a mixed population of low to moderate income patients.
The “alternative medical culture” also prevails in the two research areas north of Jackson-Josephine–Roseburg and Eugene. These possess much of the same lifestyle and culture of inhabitants residing further south, allowing complementary-alternative medicine (CAM) to be an important part of their medical philosophy. As noted elsewhere on this page, these former borderlands to the large urban setting developing in and around Portland also played very important roles in the history of this state in general when it comes to medical practice, belief and licensure. Non-allopathic regions had their political centers in the Salem area (the lower Willamette Valley research area) during the late 19th century, whilst allopathy maintained political control of the larger town/city of Portland. Some of this fascination with the value of Salem in state politics continues today with CAM and ND programs, not just because this is where most of the legal decisions were and are made for medicine in general, but also due to its location between the northern and southern halves of the state.
For a very short time, the National College of Naturopathic Medicine (NCNM) in Portland tried opening a sister school–the American College of Naturopathic Medicine (ACNM) in Salem. It ran from 1979 to 1981 and was managed by two NCNM graduates, who had earlier removed to this state via the Kansas-Oregon Cohort program then operating for Pre-naturopathy/Naturopathy college students. ACNM opened at a small circular office building in Salem (see map earlier on this page and related notes within my other history of naturopathy pages), but its program was short lived. (Due mostly to financial problems according to one discussion I had with the higher ups in this profession; one individual was then still active in the region, sometimes visiting and teaching at NCNM in the late 1990s).

As an aside I should note that another very different “natural medicine” school was opened in Eastern Oregon during the late 1950s and early 1960s. This “school” was run by a lady masseuse and alternative medicine “healer”. The needs for care in Eastern Oregon were at the time possibly being poorly met by the current systems underway. The Eastern Oregon versus Western Oregon experience in both regular and alternative/CAM medicine had a number of effects upon these professions in the state as a whole. Licensure and accreditation were the standard philosophies of all schools in the country during this time, but the definition of the Naturopathic profession was still up for grabs to some extent. It was primarily the needs of the low income families and communities that made it possible for these non-allopathic practices to find their way into the local health care system. There is this common feature for the stories we have pertaining to the successful development of non-allopathic professions in general. Poor services, lack of services, inaffordability, and lack of respect for the education and the profession are major reasons that people turn to the “irregulars”, “eclectics”, naturopaths, and other non-allopathy forms of medical or health practice.
When we review the state map again for its research areas, we find that the coastal communities are pretty much isolated from each other and the inland, although it is possible for these coastal areas to form links or economic bonds with the nearest neighbor inland. People in and around Florence have Eugene to go to for special care and unique medical needs. Many of the Eastern Oregon areas lack these direct links, and even though this is mostly because the populations are so very low, this ultimately does have an impact on the quality of care that people in these Eastern Oregon settings receive. In a later topic of review, for example, pertaining to breast cancer screening, this impact has an effect on the potential survivability of cancer victims due to late diagnoses. This could also be impacted by affordability of care, quality of care, and numerous other public health issues related to management. Fortunately, the various maps of Oregon state’s health status, at the per county level, do not really demonstrate any sub-state areal behaviors aside from those ecologically, environmentally, demographically and historically expected.
.
.

Mapping Homelessness. In the course of my geographic reviews of the most eventful diseases impacting low-income settings during the past 25 years, I cannot help but notice a number of common themes always developing in my findings. When mapping the spatial distribution of homeless camps in Portland, Oregon in the summer of 1997 for example, I found that there were certain strategies to where the homeless reside that were exceptionally commonplace. The homeless did not pick a place to reside due to privacy needs, or the ability to form small encampments for socializing, or proximity to local food and beverage stores. The most important facts for selecting your camping area seemed to be its proximity to major highways for use in traveling to other towns and cities, and most importantly, proximity to the various agencies that provide you with services, like the local downtown soup kitchens and the non-denominational, informal church settings.
Within these settings, one of the most interesting things about homelessness is that human behavior is the same whereever you go. People have this natural tendency to segregate themselves into groups when they gather at soup kitchens. With homelessness, one of these sets of contrasting groups is the ‘haves’ versus ‘have nots’. The ‘haves’ are those who do something to earn a little money on the side, be it panhandling or cashing in on the deposits from cans and bottles. This gave them a bit of an edge at the soup kitchen. Those who have a quarter or two bits could make their way into the serving area first. Those who don’t have to wait. As if this were not enough, those with multiple quarters could also afford a cup of jo with dinner at a cost of two bits, and for another two bits you could take a shower and shave before setting up your bed for the night.
This slight edge you had on the others had two benefits. The first benefit was that you were guaranteed something to eat, by reducing the likelihood that they might run out of things by the time you are served. The second benefit was that if you were employed, you could get in and get out of the facility as quickly as possible, which a number of people who drive up in cars wearing work-related clothing often did.
So there was also this way of separating oneselves in this setting into the employed, but barely compensated for your time versus the unemployed. Other ways the homeless population tends to segregate itself into groups are obvious. Back in the late 1980s there were the skinheads versus the others, the religious converts versus the non-converts, the domesticated street people with kids and sometimes a spouse versus the others, the teen gothics versus teen non-gothics, the drug and alcohol free community versus the “losers.”

These lifestyles also influenced where and how they resided in the downtown area. Teens tended to stay in the concrete downtown setting, staying in halfway houses funded by numerous grants most of the time. The older members tended to stay in the parks and at park edges, or make their way back to some more isolated periurban setting, located just across any of several bridges within the downtown region. In the 1990s, as the numbers of hispanics from Mexico and further south arrived in the Portland region, these people tended to develop a community of their own in the larger park areas filled with plenty of shrubs and trees. On several occasions I recall walking along a trail through a certain portion of the largest park in the city, and by looking up on the hills to each side could see small candles and fires ablazing. Normally one would feel threatened as if walking down an alley in New York City, but this was not the case in this vicinity, at least during the time I was there. This was where the Mexicans were staying and socializing–out of sight, out of mind.
In other much smaller parks it was not unusual to see single, double and triple sleeping areas beneath the rhododendrons and evergreens. In another large park, there were a number of fairly well concealed ‘fortresses’ build so to speak, with small trees serving as part of the cover, along with a ground cloth, blanket and even a small pack of supplies sometimes sitting there untouched. In yet another park setting there was this place where an old cottage sat from the 1930s. This cottage was where someone I became well familiar with over the years–a 6 and a half foot redheaded man with a 15 inch scraggley red-haired beard who called himself ‘Luke”, probably in reference to the Bible Saint Luke. Luke told me he was from the special Green Beret team from the Vietnam War, an occupation which he claimed he never recovered from completely. A person this large rarely had much to be concerned with regarding physical threats and the like while residing on the streets. He made good use of his survival skills with the old gardener’s place he found to stay, back in the woods of an old mansion estate. He had a root cellar he made use of and a latrine, two necessities of street life he told me, in terms of “squatting in luxury” and homelessness he felt this made him one of the most fortunate individuals to frequent the downtown parks and streets for food, clothing and other necessities. He rarely made use of the deposit money industry to earn his money, but instead chose to help people set up booths at the Portland Saturday Markets where I occasionally worked, as well as work for farmers on the side loading and unloading their crops, and dumpster diving in certain places for some of the best foods a street person could find.
Singularly and most importantly I learned by conversing with Luke and others that the most important aspect of health in the Northwest for the least healthy of people wasn’t just the issues regarding lack of adequate facilities or insensitivity on behalf of the corporate world, the main problem was a combination of the way the homeless view themselves and their values to health and life, keeping a clear point of view of things, avoiding the schizophrenic kinds of thinking that can set in if one is not careful, making the best use of the resources that are available to you. Luke claimed that these resources do not come from the status quo, but rather from your self, the choices you make and the avenues you take whenever new opportunities are on the horizon. One could walk 5 to 10 miles along the same street, a dozen or more times a month, but on that one occasion pass by lost, dust-coated five dollar stuck in some roadside weeds due to the seasonal winds, and either see it or not. Such was the case for the highways that the homeless liked to camp next to. For those living in the urban core, at special halfway houses designed to assist the mothers-to-be, the families, the teens, and the special needs victims, this survival behavior so important to park-residing homeless populations was not so much a factor necessary for recovery while depending on the halfway houses. Again, it is the inner mind set that determines one’s fate in such situations, and making good use of the resources and support services you have at hand. None of these unfortunately have much of a relationship to the growth of the programs in Public Health services provided for many urban settings.
.
Mapping a Cancer Screening program. In my study of breast cancer screening programs by county, and the relationship between dependency on mobile screening vans and late diagnoses, I determined that the two worst counties in terms of late diagnosis for the time were eastern and rural in nature, not a surprise when cost of renting the van and traveling is a concern. Oregon state is primarily populated along the Willamette River Valley and its western coastline, both contained mostly within the western half of the state. The presence of natural and man made barriers to the far eastern parts of the state made it easier for opportunities to diagnose early to be missed. In the mind of the epidemiologist, this was a consequence of lack of funding combined with questionable management. In the mind of the accountant or businessman this was a consequence of a normal cost-benefits analyses equation.
.
Mapping Chemical Release. In my study of chemical releases from an Aluminum manufactory, specific wind patterns made certain regions highly susceptible to exposure to industrial plumes and therefore more likely to develop certain forms of cancer or leukemia in theory. This fear of cancer was generated by a set of families living in a paper manufacturing town just across the river. Six of them had kids with childhood leukemia. What they didn’t know was that the leukemia cases had different histologies, and so even though they shared a similar diagnostic terminology, they were probably not really related in terms of the statistics related to their cause. Nevertheless, the work resulted in a poster board proposing a way to monitor the region based on topography and climate patterns. This and my first GIS epidemiology project.
This led to a much more extensive study about three years later, covered by grants, when I began an analysis of chemical release sites on the state’s environmental health. For this project, the chemical information provided for each confirmed chemical release site was evaluated, reclassified and compared with the distribution of leukemia and myeloma case distributions. Also, each business was recoded and regrouped based on its Standard Industrial Classification identifier, allowing for oil companies of different types to be merged and compared with cancer cases, followed by a similar process for electronics manufacturing industries, automobile industries, ship manufacturing, lumber products, etc. Finally, several new methods were developed for testing these spatial distributions, the most important of which being the creation of a hexagonal grid algorithm. This data and methodology was then applied to the total toxic release sites inventory and the confirmed sites profiles for chemical release applied to any other sites lacking data on chemical release, with their SIC used to define the types of releases they were expected to demonstrate. This resulted in my controversial maps on the distributions of cancer types based on specific chemical behavior or SIC-defined “profiles” for each business. This then led to my development of the hexagonal grid algorithm, one of the most valuable tools I ever invented in disease mapping.

Mapping Water Quality. Water quality and the availability of potable water is a major concern for nearly all states and watershed monitoring programs in the United States. The Willamette Valley has a long history of engaging in agricultural activities in its rural and suburban regions, and a long history of industry in the suburban to periurban settings. In addition to farming and industry, commerce requires that ample petroleum product and chemical resource storage be available within the Willamette Valley region, making it necessary for railway and highway travels be engaged in by providers and suppliers of these resources. In the most rural of settings, lumber has been a primary natural resource industry in the Pacific Northwest ever since its first settlement by immigrants during the 19th century. During the past century, the lumber industry has led to the development of paper industries and wood products manufactories, all industrial settings where water is a necessity for industrial and human consumption purposes.
The other regional effects of water related land quality and land use features relate to population health and disaster management issues in the most heavily populated areas. The western edge of downtown Portland demonstrates susceptibility to earthquake, landslide and creep related problems as these relate to urban and industrial buildings stability, but especially individual household stability. Sections of land along the Pacific Coastline have natural disaster concerns related to tsunamis and earthquakes. Inland regions have drought and extremes in climate to contend with. In a DEM study of a local watershed I was engaged in, my research on the region’s susceptibility to flooding also had applications to such public health issues as the spread of microorganism-based diseases and potentially carcinogenic waterborn chemical pollutants.
As detailed in a later study, this issue chemical release is an important public health issue due to the sharing of these local watersheds. The contamination of the Multnomah watershed and its definition as a Superfund site around 2000 represents a milestone in how environmental health related issues become a regional issue instead of a very localized issue with one or two industries or companies laid to blame. Similar concerns exist for a number of other locations in the Pacific Northwest, all with heavily populated Urban centers, ranging from the Coos Bay and Port Orford areas to various settings in and around Seattle.
.
Mapping regional outbreaks and behavior related health risks. Regional outbreaks has been a primary topic of public concern since the migration of AIDs into Oregon during the mid to late 1980s. This STD had an unusual history due to one or two local male carriers of this disease who managed to successfully transmit it heterosexually to a number of other future victims. (These were not necessarily the first cases locally, but they were the most controversial because of the news media). The local transexual and homosexual scenes only added to these public health concerns already impacting the Pacific Northwest by 1988/1989.
In addition to the regional outbreak of infectious diseases were a number of human behaviors and conditions that had a tremendous impact on the local sociological health of the community, with some of these unusual behaviors and at times criminal public health-linked behaviors extending well to the north and into Seattle. Sociologically, the most noticeable and ‘newsworthy’ outbreaks in human behavior between 1980 and 2000 pertained to homelessness, street drug abuse, child sexual abuse, unhealthy practices engaged in during periods of pregnancy on behalf of youths, local support for herbal medicine and OTC supplement use by patients, the public need for engagement in various forms of physical and metaphysical healing faiths, and the growing public support for medical cannabis use.

During the late 1990s, after nearly 15 years of studying the history of alternative medicine and Oregon Trail medicine, it became clear to me that several reasons possibly existed for the increases in public interst in these other forms of healing. These social behaviors have since been observed as well for the histories of the numerous yellow fever and cholera epidemics taking place between 1797 and 1855, leading me to add this particular topic to the courses I regularly taught on the history of plant use in medicine.
The failure of allopathy or regular medicine to produce a cure is why the public tends to turn towards non-allopathic or ‘irregular’, alternative and complementary medical practices.
Throughout the 1800s, the failure of bleeding and mineral remedies to work any better on the sick than the alternatives convinced people in masses. The large numbers of deaths brought on by allopaths versus homeopaths in a New York setting during the 1849-1853 Cholera epidemic demonstrated the ill-fated nature of going to a regular hospital when taken ill. The same was true for the much earlier yellow fever epidemic tragedies of the early 1800s. One of the more important combination therapy physicians for his time (an allopath with training in homeopathy as well), produced a review of the deaths in New York Allopathic versus Homeopathic hospitals during the mid-19th century cholera epidemics, and tried to show that allopathy was the more fatal place of care of these two. (A few years later, as chief editor of the national journal on homeopathy ca. 1856-7, he converted totally to allopathy due to the refusal of either side to allow for hybridization of their philosophies and practices, but mostly his disappointment with the homeopaths to support some of the allopathic beliefs in disease, population and climate. His subsequent mapping of disease is covered on a separate page.)
Much of this history concerning the failure of allopaths was forgotten by the 1900s, due primarily to the maturation of the germ theory into the bacterial theory with its very strong evidentiary background and history. Some of these steps leadin gto the failur of allopathy were repeated beginning in the late 1980s and 1990s, when regular medicine failed to find the cure for the new epidemic disease – AIDs. Similar dissatisfactions ongoing about “the cancer cure” furthered this social movement, leading to the development of integrative medical practices offered and performed by special facilities around the U.S. These programs offered spirituality, art therapy and mindbody healing processes as a part of their traditional allopathic regimens, practices that continue to this day. Other chronic diseases adding to this public dissatisfaction with allopathy have since then included the develop of drug-resistant diseases like Hepatitis (all types), the iatrogenic Clostridium in-house epidemics, the re-emergence of a drug-resistance tuberculosis, and the evolution of new strains of native (E. coli and Hanta) and foreign born diseases entering this country (for the Pacific Northwest, the Pacific Rim effect).
In the Pacific Northwest, we see even more unique effects of regionalism on this part of the health maintenance/disease prevention market. The natural foods market for example led to the development or publication of cases involving several serious E. coli strains via unprocessed milk and cases of herbal medicine intoxication due to overadministration (glycyrrhizinate-induced Na-K+ imbalance, at first misdiagnosed as Addison’s disease), and facilitated public health issues like the complications that can arise from combined OTC plant drug-prescription drug use by chronic disease patients and the lack of integrative medical care programs presenting as alternative case management activities remaining undocumented in the regular medicine case management medical records.
.

Dr. John McLoughlin, before and after
Mapping New Medicine in the Pacific Northwest. The numerous alternatives to the status quo have some of their strongest followings in the Pacific Northwest. The reasons for these unusual movements and behaviors once again have something to do with the location of this part of the country relative to other sources for impact and influence. relative to the East Coast and Washington, D.C., the Pacific Northwest is one of the most distant settings of this country, if we exclude Alaska, Hawaii and the various island settings the US lays claim to for the moment. For most of the history of the Pacific Northwest this had provided those residing in this region with the opportunities to be “different”, to state it mildly.
The history of this region’s medicine provides numerous examples of this unique aspect of this hinterland setting, when compared with much more settled communities residing east of the Rocky Mountains. These hinterland settings had a number of effects on United States medicine that helped give rise to every one of its major alternatives existing during the nineteenth century. The 1830s fort settings, established for the purposes of fur trade, allowed trappers and Native American medicines to become a part of the American medical culture, mimicking much the same activities and beliefs learned and born near the Great Lakes and back east a century before. The first physician to run and perform practice in this fort, Dr. John McLoughlin (portraits above), was his own unique self–a transcendentalist constantly turning to the use of the newly discovered skills of hypnotism, orbs and Quimbyism to heal his patients.
The settlement of the Pacific Northwest region over the next ten to twenty years provided distant communities for the east coast and midwestern forms of non-allopathic medicine to migrate to and reestablish their strong local followings. It is no coincidence for example that the first forms of medicine outside the fort and military settings in this region were the alternatives so popular elsewhere in the United States. The very first journal to be circulated regularly to masses of settlers in Oregon Territory-now-State was the Physiomedical Recorder out of Cincinnati, Ohio by Simeon D. Earle in 1852; this journal reviewed the practice of Thomsonian medicine as it was taught in the midwestern states. The first medical journal published in Oregon came from Salem and was devoted to the same strongly religious-based physiomedical philosophy. Allopathy had yet to make its claim through the printing press.
The opening of regular medical schools in the Willamette Valley of Oregon did not help these political matters any. There were two regular medical schools started about the same time by the 1850s, one in the central Willamette Valley near the Salem area (first called ‘Wallamett’) and a second in the Portland downtown setting. This presence of two schools naturally led to two points of view at times about medical philosophies and faiths, which during the late 19th century often led to a clash between professors at these institutions regarding the validity and usefulness of the new forms of electric cure being developed. Such behaviors continued over the next decades, until it was decided that these two schools could merge to form the one and only medical school, still operating in the State of Oregon to this day.
But during this period of merging and the political strengthening of the field of allopathy in Oregon, some time between the 1880s and the early 1900s, other philosophies were being heavily promoted in the nearby communities and the local doctors devoted to homeopathy, eclectic medicine, a few remaining followers of the sanative (religion focused) practice of physiomedicine, followers of the new chiropractic movement, local chiropeds (now taking on mostly by a few old time trappers and “Wild Bills” clad in frilly buffalo jackets), chinese medicine-promoting traditional chinese medicine practitioners, and the “New Eclectics” naturopathy practitioners. A homeopathic institution and hospital was also established in the Portland area during this time (a few blocks up from Pioneer Square), and a sanitarium run by a regular MD from the Good Samaritan facility opened in the Mount Tabor area (and the cottages are still there). Its primary purpose was to treat prostitutes addicted to opiate products, becalm women suffering from nervoses, and treat whatever working class gentlemen suffering from various forms of work related stress was willing to admit to such a need.
The urban setting in which these events took place was small in size for its cultural diversity, and was a fairly heavily populated setting for being a part of the Far West. This naturally enabled some ‘unique’ practices and followings to develop that had impacts on the local public health. One of the most interesting buildings in downtown Portland was the Oddfellows building with its newly installed electric lighting contraptions. This building housed most of the palm readers, fortune tellers, soothsayers, phrenologists, early psychologists and occupation therapists, many with very descriptive room numbers revealing their beliefs–the lucky number 8 as a very common theme at this time.
Bicycling and exercise were also strongly promoted by the 1890s during this time, and a main theme at the upcoming Lewis and Clark Centennial. Homeopathy had developed into a practice that was now strongly promoted and supported by women more than men. Since 1855, local plant medicines had become a major source for revenue in the national drug market in the Portland area, resulting in trade relationships set up between the Pacific Northwest and distant international trade cities and ports, with the Oregon natural resources now most important to the field as a whole, such plants as Oregon grape, yerba mansa, yerba buena, and yerba santa, all marketed by regular and alternative pharmacy companies.
By the 1920s, these features enabled the Pacific Northwest to develop into its own “social organism” so to speak, replete with individuals engaged in new medical thinking, new forms of natural philosophy and new forms of plant drug-related commerce. The local foxglove industry was most important to the allopathic profession during the early 1900s. The local sphagnum moss industry gave the Red Cross the ample amounts of materials needed to make sterile wound packs for the two World Wars. The largest wooden planes ever built and flown for the second World War II came from local Sitka Spruce logs. Mint oil, celery powder and tonics, cascara sagrada laxative products, assorted herbal medicines all gave the Pacific Northwest the boost in economy it needed, in spite of the presence of increasing numbers of chinese physicians, eclectic physicians working side-by-side with them, and the various new questionably licensed physicians making their way into this region from the Midwestern states, practicing medicine based on certificates from unaccredited schools and programs in and around Chicago.
The distance between the Northwest and the heart of American medicine legal authorities, Washington, D.C., in combination with the effects of this distance upon transportation between the two coastlines, made it possible for the Portland and Seattle cities to establish themselves as unique entities in the United States allopathic and non-allopathic industries. Everything ranging from patent medicines and tonics by Parke and Co. (later Parke-Davis), to 6 foot mahogany static electric cure generating wheels, to the first X-ray machines to sit in front of (without protection) riddled the regular medicine marketplace. The alternative profession was equally unique in what it had to offer patients, such items as acupuncture needles and moxibustion sticks, Traditional Chinese Medicine recipes and an exotic aphrodisiac, to the expected west coast produced herbal medicine and homeopathic products making their way up the shoreline from California, serving the entire west coast medical market from lower California to Seattle, Washington.
When the AMA began to send representatives to the Pacific Northwest during this time, much of the foundation for facilitating alternative medical viewpoints and practices were well established. Perhaps the strongest evidence for this very well planned development of a local social movement favoring the non-allopathic professions is found in the New Eclectic 1895/6/7 annual meeting documents. In 1895, Portland, Oregon, was defined as the most important political center in this country, and so attempts were made to keep this form of medicine alive by selecting Portland as the site to carry out the next and last successful annual meeting of physicians now calling themselves “New Eclectics.” The bacterial theory was the cause for this split in the this particular non-allopathic profession during the late 1800s. As the last generation of allopathy trained medical climatologists and medical topographers were dieing off, so too were many of the non-allopathic professions who were unwilling to accept the new findings and teachings related to the bacterial theory for disease.
This Portland New Eclectic movement resulted in a very successful meeting the following year (covered at this site). But this success was followed by a lull in the school based teachings of major alternative medical professions. The actual practice of these skills by local hospitals and medical groups remained intact, but no more new schools devoted to these practices were being built, leaving the Pacific Northwest without a means to provide such an education. Very quickly, this change led to a rapid increase in Christian Science practitioners and other metaphysicians in the Portland area. Were it not for a change in the legal system, this continued growth would have remained successful. But this increase in numbers resulted in exceptionally long listings of “religious healers” in the local business directory, outnumbering the lists of regular MD and alternatives at times. The same was true for other states as well. In the Latter Day Saints state of Utah, the fact that the Governor was so supporting of the non-allopathic healers made many on the state committees there unhappy with the state of medicine in Utah. The alternative MDs (Eclectic), DOs and DCs were then receiving as much notoriety, respect and popularity, if not more, than the regular MDs. This set the stage for the events that led to the famed Utah study of non-allopaths in the mid to late 1950s, accompanied by the opening of the country’s first Naturopathic School in Portland, Oregon around 1957.

Mapping CAM Specialties. This unique tendency for complementary/alternative medicine (CAM) to develop a large following was immediately clear to me from the day I removed from the Long Island, New York area to Portland, Oregon in summer of 1985. The reasons for this move included my own need for another opinion about how best to treat a seizure problem, since the medical school I was a student for was very much behind the times in new techniques, in particular the works of the Neurological Research centers like those in NYC at Columbia and in Portland, OR at the Good Samaritan Hospital. Another reason I opted to move west pertained to my work outside the medical school–I was a regular in the newspapers and on TV due to my outdoor classes on edible and medicinal wild plants. This publicity came to a peak one year when a short quip about my work was published in a local news column in a newspaper with the largest local circulation in the country, serving all of Long Island and parts of the New York City region.
Due to this publicity and a video about one of my outdoor classes that aired on the local cable stations, I was handed an offer to attend the school in Portland, Oregon on naturopathy. At the time, as part of my investigation of the alternative/herbal medicine field, I was regularly attending classes and such in other programs offering “degrees” that were non-acredited (an “MH” or Master of Herbology program for example); this offer to attend the Pacific Northwest school classes once I graduated from MD seemed enticing. Six months later I decided I had to remove to Oregon for better care for a year; two months later I was residing in Portland by August of 1985.

Results of my counts of the directories. The left graph is counts for each healing type; the right graph depicts the same as counts displayed on the same bar.
The other schools of medicine in this city were a constant interest of mine. As I researched their history I incorporated a lot of my findings for this work into the courses I taught at the University. One of the more important projects I engaged in was in the winter of 1991/2, when I reviewed all of the local business directories and phone books and compiled counts of the various forms of alternative healers who resided in the immediate urban setting.

The directories I reviewed went back to 1876, were not for every year, and in some years, certain fields of medicine were not included in these directories. Nevertheless, this enabled me to produce the graphs for this section, which have a lot to reveal about the history of medicine in the United States, much less Portland, Oregon and vicinity.

The most important findings from these analyses are the following peak periods in Oregon CAM history: 1893/4, 1907-9, 1930-1935, 1957/8, and 1986 to present. These either demonstrate peak CAM influence in terms of numbers of health care providers, or in terms of the overall history of this profession in general and its multiple offerings. Physical and mechanical forms of healing evolved following the body building movement effectively popularized by Bernarr McFadden around the turn of the century. During the late 1930s, Christian Scientists stopped listing each and every practitioner in the local business directories. By 1957, the local school devoted to the current form of licensed, accredited program in “naturopathy” began (and for a while its applicants were eligible for federally funded loans due to the Korean War).

Mapping Native American Plant and Cultural Heritage. A natural offshoot of herbal medicine is of course Native American medicine, and the Pacific Northwest like any part of this country has its Native American philosophies and beliefs when it comes to traditional medicine. When I began my taxonomy and plant chemistry projects at Portland State University in the winter of 1986/7, turning to the local traditions wasn’t my first direction as a researcher. I was focused on a theory I developed about cancer drugs evolving as selective medicines developed for a variety of reasons other than to heal cancer. It seemed more natural for a toxin that worked somewhere else in nature to become anthropomorphized into a certain type of medicine, not the kind that nature had in mind but instead the kind that mankind needed.
But during the coures of my reviews of all the cancer drugs and their similars like the antiviral medicines and autoimmune reactive plants seemed to demonstrate anything other than that these toxins were usually very complex, highly evolved chemicals, that were for the most part unpredictable. Multiple paths could produce cancer drugs. The only thing they seemed to have in common was that the most effective cancer drugs were usually produced in the later stages of the evolution and application of a given series of syntheses, like the end stage of a sesquiterpene lactone path, the end stage of any of several benzylisoquinoline paths, the end stage of a quinone or terpene alkaloid path. The main thing these all had in common was selective toxicity after completing several stages of chemical evolution. Because I couldn’t explain why cancer drugs evolved, based largely on my findings for the Pacific Northwest flora, I decided to put aside this philosophy for a while. (Meanwhile writing a lot of it up on some other pages at this blog.)
It was during my first year or two of this work that my name managed to circulate quite a bit due to my research on alkaloids. Most students equate alkaloids to the nicotine and opiates. I was researching the types of alkaloids closely related to opiates, but few realized how complex the alkaloids are in the plant kingdom and how diverse they can be chemically and pharmacologically. One day, this led to a a student from the local Reed College calling me out of the blue to ask me if I would help her with evaluating a local Native American encampment site. Her goal was to document the local flora, determine what uses might have existed for these plants, and see if there were any signs of these various forms of utilization based on the layout of the region and the site’s archeological remains. This work was being done of a tribe native to the Columbia River valley known as the Klamath Indians; it was completed sometime in the winter of 1991/2.

Later that year, during the fall of 1992, I had the fortune of meeting Chief Lelooska or Don Smith (1933-1996) for the first time. Born as Yana the Bear by a Cherokee mother and artist Shona Ha or Gray Dove, he was the grandson of a full blooded Cherokee who went by the name ‘He-Kill’. He-Kill was good with a carving knife, as any grandfather should be, and it was this heritage and persona that had such an impression on Yana the Bear that decades later, by the time he was a young adult, Yana became the highly productive individual that decades later I came to know as Lelooska.
Unfortunately, the family’s Cherokee descent did not offer the family much in terms of any additional benefits during their early years of residency in Oklahoma followed by California where Don Smith was born. The family moved to Oregon in 1936 and ran a gift shop for tourists. As he got older, Yana or Don’s skills as an artisan improved. In 1959, he carved a 50-foot totem pole for the Oregon centennial Celebration. This pole was then sent to the Deep Freeze Research Station at the South Pole. Years later, its was removed back to the Washington Park Zoo.
In 1961, with adzes and knives at hand, he removed to Ariel, Washington. A traditional longhouse was built as well as a log museum and art gallery. It is here that he began his work as a dancer, singer and storyteller retelling the legends and myths of the Kwakiutl Indians while donning their masks in a dark, firelit room. Seven years later, in 1968, he attended a potlatch offered by British Columbian Kwakiutl Chief James Sewid. Appreciative of his work and his goal in preserving a part of his personal heritage and this region’s local heritage, Chief Sewid adopted Don Smith into his family.
Ever since, Don Smith has been known as the great Carver known as Lelooska, meaning “To Cut Against Wood with a Knife.” He set up what has since come to be known as a living education center in Ariel, Washington, where he regularly engaged in carving his various wood relics during his remaining life, favoring exceptionally large objects like totem poles and early versions of Kwakiutl masks. On the side this facility offered classes on his methods of carving, hiring high school students during his later years to do some of the basic carving of the larger logs needed to make the totems and large masks, to each of which he added his final touch. (It still offers these, see http://www.lelooska.org/)
Over the years, Lelooska produced a number of ceremonial events or evenings in his plank house or longhouse. For the ones that I attended (one in 25,000 such people per year in the 1990s), he would sit at the end of a large room, with drums beating by his side as he retold the stories and legends of the Pacific Northwest Indians and in particular the Kwakiutl. For each character he had a mask that he carved, the most impressive of which were nearly than 3 feet long and could be opened to display the face of another character from his stories (his transformation masks). These masks were also of the Raven, Wolf, a Northwestern style Eagle, a grumpy Old Man, an old Indian lady with wrinkly skin, and a transformation mask bearing the pure white face of a very young child-like character within symbolizing winter, all examples of characters he produced for his stories, from masks hand-carved from western cedar logs.

For more of Lelooska, go to http://www.lelooska.org/
When I first went to one of these nighttime ceremonies, I was fairly well engaged in the study of Pacific Northwest ethnobotany, and had already developed a number of classes focused on this material for my regular plant medicine classes at the university, the main reason for my visit. By 1992 I had produced an extensive series of tables documenting plants by different cultures in relation to their chemical make up. These tables were in fact my most valuable possession at the time, and students who first saw them and learned to make use of them saw the value in pulling all of the minutia of the plant use knowledge into a single document. These graphs complemented a book I developed a couple of years earlier for teaching the taxonomy of plant chemicals, named Plantae: the evolution of Natural Products (still noted today on some book buy searches).
From 1990 on, this book was my primary claim to fame locally until the tables came about. In particular, these latter publications with the tables became very popular. I know this because more than twice as many people bought my book at the local copy center during those years than numbers of students taking my course. Due to my work on the evolutionary process and how it relates to the plant chemical synthesis pathways, this book still can be found today at times on the web.
When I returned to the classroom as a graduate student in 1996, and began my classes in Community/Public Health, I turned first to studies of people and how they focus on personal health practices. Many of these classes were required for the program, one course, “Exceptional Human Experience”, focused on the unique experiences people have when experiencing what many consider to be everything from “exceptional achievements” to “small miracles”, like breaking the 4-minute mile for the first time or undergoing an incredible recovery from a chronic or lifelong disease. This philosophy interlinks the mindbody way of conceptualizing diseases and cures with the alternative philosophies and traditions being vocalized out there by the more eccentric believers in unique medical philosophies–an atypical topic for a program of public health for the time.
Back in the Native American world, I found applications of this philosophy to other issues as well. At the time, I was devoting a number of my research projects to Native American issues. The first such project dealt with circumpolar groups like the Inuit and Saami, their unique philosophies, their ways of life, and their legal and moral rights. One of my more interesting studies came about when I began work on the urbanization of Native Americans and the impacts this change in lifestyle had on their health and hygiene. During this time I began to review population health in general, the migration of diseases like Hanta, the development of athlete’s heart by some individuals in Arizona due to a life of poverty and constant foot travel, the effects of assimilation on the Inuit Tribe due to Hudson’s Bay company interactions in Alaska and parts of Canada, and the local indigenous rights regarding intellectual property issues and The Rights of the Shaman, a term paper I wrote that got a lot of resistance from my professor and as a result was never graded due to differences in opinion.
I was most interested in the onset of diabetes by Inuits during the late 1880s. This was due to their subsistence on military food supplies provided by the local fort operated by Hudson’s Bay Company. Researching how and why these changes in health and longevity occur following cultural change, my attention was then drawn to epidemiological transition theory. Thus began my studies on the temporal mapping of cultural disease patterns, a topic which has applications to the study of Pacific Northwest Cultural medicine history, philosophy and theory.
During the late 1990s, I spent a year lecturing on this topic and gave a talk on it at the Northwest regional meeting for the American Indian Science and Engineering Society meeting, and a Pacific Northwest Native American students group. During this time I reviewed the urban asthma issue experienced by Natives and/or low income groups and underwent a detailed metaanalysis of the literature on the “New World Syndrome” then being promoted in medical anthropology journals. (This syndrome is now considered a metabolic syndrome and is assigned that ICD in the medical records.) I then produced a very lengthy treatise on this topic including my detailed diet and nutrition studies, and my review of a number of related topics dealing with Native American medical philosophy, and the possible incorporation of some of these practices into Pacific Northwest health care programs.
As a consequence of the specialties that evolved related to psychosomatic medicine during the 1950s, an important part of medical and clinical psychology training came to be the study of human behavioral medicine and medical psychology/psychiatry. To many people, Native American beliefs and traditions played a major role in our lives, even more so in the Pacific Northwest due to its unique heritage and diverse beliefs. This philosophy was especially true for those people devoted to the use of alternatives and complementary therapeutic practices. About this same time, a book was published detailing a Canadian program that had developed a way to incorporate traditional native philosophies into Western medical traditions. This method of practice was engaged in by the major medical centers in the country, and was found to facilitate one’s transition into have to live with a recently diagnosed chronic disease. Because these diseases were handled in a new way, with alternative goals and philosophies in mind, some of the older fears and other unfortunate thoughts about these conditions diminished. In this way, the pibloktoq common to certain Inuit settings no longer received the improper diagnosis of some psychiatric condition and new cases of epilepsy became representative of stages in live one has to go through while growing up.
I liken this manner of successful treatment and improvement of quality of life in these patients to the Health Belief Model taught in most public health programs. To make this model better fit the alternative Native American strategy for providing improved care, I proposed that the underlying philosophy be allowed to be updated or changed in order to better fit the needs of the individual going through his or her chronic disease crisis. I terms this method the Modified Health Belief Model.
There are a number of culturally-bound syndromes that can be treated this way, and some problems considered to be biological in nature like epilepsy. In fact, my study of cross-cultural behaviors relative to one’s experience and persona history with epilepsy shows that culture and beliefs taught by parents, family, friends and health care providers play an important role in the long term changes and outcomes people with these kinds of conditions experience.
These psychosomatic effects, defined as such during the 1970s, in fact evolved from the previous endocrine theory out there (ca. 1930s), and the age old “sympathetic nerve theory”, a philosophy defined around 1660 by a religious leader who blaming the power of sympathy on the body, instigated by nerves that run sympathetic with or parallel to the spine. In the 1980s, my medical school years, the autonomic nervous system theory and gate theory related explanations for some of these effects were replaced by the endorphin/enkephalin theory ca. 1980/2, followed by the interferon/autoimmune theory, and then psychoneuroimmunological and psychoneuroendocrine theories. the most alternative thinkers and writers in this field today even label this philosophy the quantum energy theory for otherwise inexplicable cures, referred to by many as “miracle cures” and by others as shamanic cures. These Native American philosophies and traditions also link up with my ‘transformation of common belief’ teachings, providing us us with a little more insight into why some alternative medicines work just as well as allopathic remedies. This is not necessarily the case for all treatment plans, but it does help to explain those cases with hard to predict results and outcomes, and others with hard to explain cures.
.

Mapping New Cultures in the Pacific Northwest. Even before it was a State, Oregon Territory had its multiculturalism. Aside from the two major sets of Native American groups residing in this region–the island community groups from the first migration and the more inland groups from the second and third migrations–there were the people from the Russian trawlers making their way across the Bering Straits and Aleutian Islands, settling in upper Alaska and certain harbor settings as far south as central Oregon. Then there were the numerous Pacific Rim groups and communities that made their way into this region as early as 1845 (some like to say the Hawaiians had their feet on west coast soil as well, many generations earlier, although Pacific Northwest evidence for this is for the most part scanty or lacking, ignoring for a moment the Columbia River’s Kennewick Man that was unearthed). In the very early annual reports made of inhabitants of Oregon Territory, we see Danish boarding houses being constructed for carpenters and brick layers to reside in, and several foreign orphanages. Commerce had already brought in ships from all directions, with most of the ships coming from Central and South America, and in particular from Chile with food and clothing. There were also ships from the Sandwich Islands, one of the fastest ways to send the military, international products, and disease from one part of the world to the next.

18th C Russian Boats and Maps
Trappers, Explorers and Oregon Trail immigrants added to this cultural complexity in the region, as lifestyles and beliefs from the various parts of the densely packed east coast and midwest managed to be transferred to this region as well. Small communes were also the norm, and like the Swedish utopians residing adjacent to Mormons just outside of Nauvoo during the years 1845-1849, so too were there religious and non-religiously minded utopian groups residing in Oregon territory, some devoted to the early 19th century socialist movements but most to any of a variety of British, French and German movements then developing the goal of occupying the Pacific Northwest. The Aurora Colony, trappers and mountainmen, Indian scouts and agents, self-proclaimed explorers, and argonauts all took advantage of this fairly unsettled part of the United States, its last virgin soil, forest, and water. A review of the census data for Oregon just before 1850 demonstated the two largest clusters of people outside a fort setting to be a Danish-run male orphanage with about two dozen young, working age boys, and a boarding house filled with several dozen carpenters of all ages, upbringings and nationalities.
.
All of these unique and very individualistic philosophies formed the basis for the first “modern society” for Oregon once it became a State in 1850. Into this new State came a number of important cultural groups, most remaining active and present to this day. Following them during the past half century or two were a number of more “new thinkers.” A century later, by the 1950s and 1960s, these old and new cultures were well known, and a new series of changes were about to take place.
.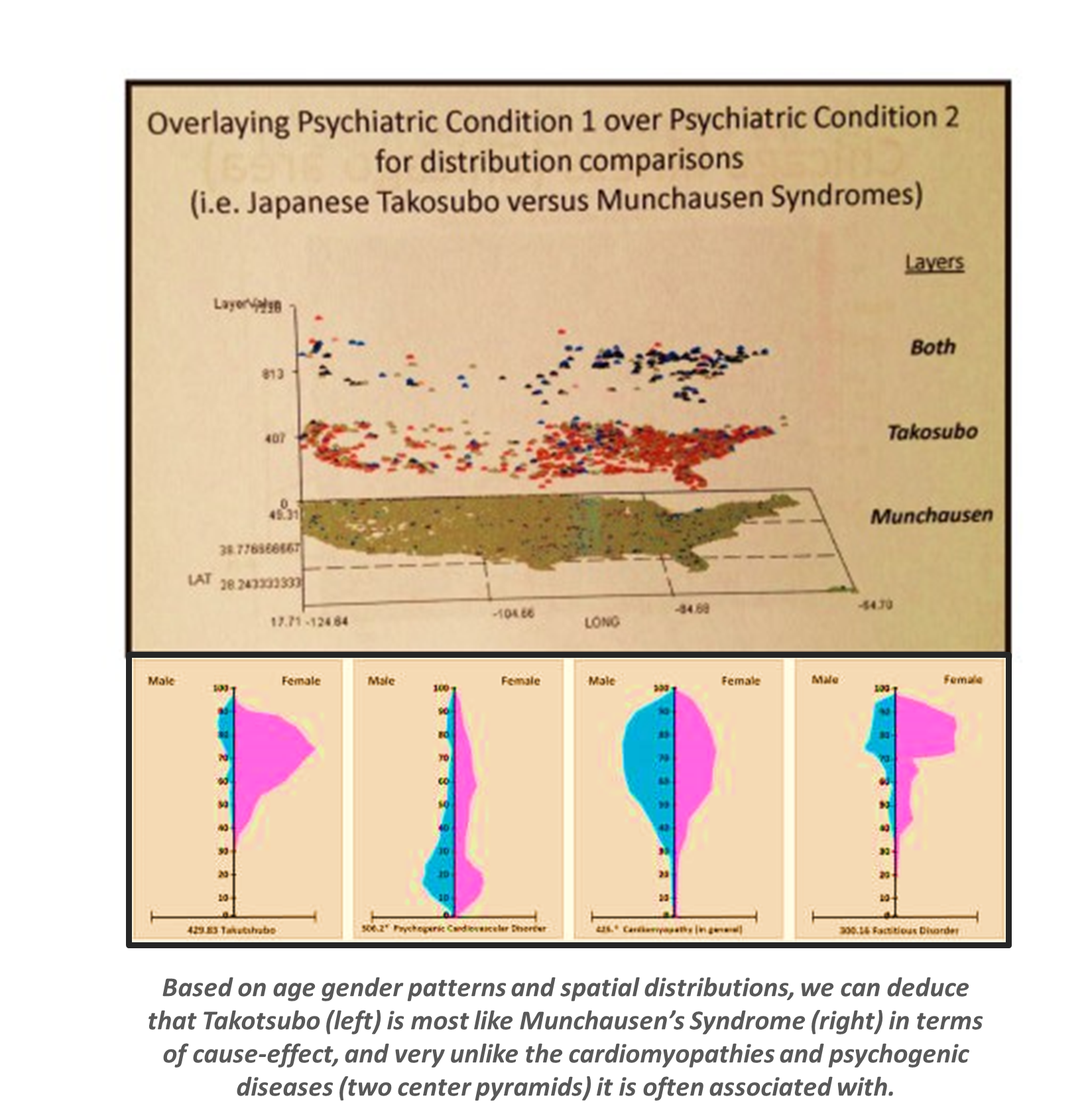
The Japanese culturally-linked diagnosis Takotsubo is very similar to the common American diagnosis Munchausens’s syndrome, both in terms of spatial distribution and in terms of primary age of onset and diagnosis.
Mapping Southeast Asian Culture and Health. One of the more important groups to come to Oregon for the first time during the state’s recent history was during the 1970s. This is when the Laotian lu Mien, Cambodian and Vietnamese families made their way to the United States due to the war (start here for more). In addition, there were Chinese descendants known as Hmong, an indigenous group from China that migrated into North Vietnam, who had also been driven off those parts of Southeast Asia they occupied for generations. All of these people and cultures had members who made their way to the Pacific Northwest. The Hmong developed a strong following in and around Seattle. The indigenous and non-indigenous Vietnamese, Cambodians, and Laotians made their way to the Pacific Northwest. For the most part these latter groups settled deep within the Willamette Valley.
Beginning in the late 1970s, these Southeast Asian in-migrations produced a significant strain on the local public health system (link to US Census Bureau review of this topic). Some of these problems continue to this day. During the earliest years, tuberculosis was the primary infectious disease concern, but in the years that followed, the psychological and social impacts of this move helped define the common medical problems this special class of people would have to face. Suicide and its similars for example were not unusual in young adults. Grandparents demonstrated psychosomatically-related diseases like the Sudden Unexplained Nocturnal Death Syndrome (SUNDS). Middle-aged adults demonstrated signs of stress and psychological/psychiatric changes, probably due to career changes, but often interpreted as genetically-related conditions as well. Teens and twenty plus year olds were experiencing a psychiatric state called “Amok” (i.e. the clinical condition “running amok” is envisioned as one running down a hall and jumping through a window); this is now more of a cross cultural syndrome than during its earliest years.
During my several months of activity with one of these groups I saw possible signs of schizophrenia and various stages of bipolar disease according to United States diagnostic guidelines, conditions viewed by the family as basic behavioral and emotional problems in need of counseling and family support more than western medicines. One could also see how the Southeast Asian children and children’s children experienced more of the effects of adaptation and dietary change on their health than on their parents, and on their parents more than on their grandparents. As both the child and family begin to develop ‘western diseases” like diabetes due to these changes in lifestyle, the forms of medicine they had to practice became more integrative, often with loyalty geared mostly towards the country’s traditional medicine and diet, not the western forms of therapy. Similar situations were found to exist as well for asthma in urban settings and various forms of ICD identifiable psychological or psychiatric states related to anxiety disorders, and some culturally-bound sexual health dysfunctions. (Reviewed later on this page in the mapping are a number of physiological-mental health ICDs and culturally bound syndromes linked to local Southeast Asian communities. I also have a page devoted to ICD 9/10 notes on these–Socioculturalism and Health).
Traditional risks also play a role in how these new cultures impact the health of this region. One of the most controversial issues during the 1990s and early 2000s pertained to the birth statistics of Hmong mothers, who demonstrated the greatest birthrates in this country at one point during the course of my research. (See News item , NIH study and California review (p. 11) for more.)
.
Mapping Cultural Medicine in the Pacific Northwest: Native American Medicine (including shamanism), Unaniism, Siddha, TCM, and Kampo. The Native American medical philosophy has partial acceptance by regular medical practitioners, more so by those engaged in complementary practices alongside regular allopathic MD therapeutics. At the local medical school in Portland (OHSU), there are experts in the utilization of shamanic curing methods. These professionals also practice and teach via the complementary school, the National College of Naturopathic Medicine (NCNM). For the most part many of the Native American medical practices engaged in over the years have been devoted mostly to Native American herbalism, consisting of herbal medicine practices based upon varous philosophies, ages and forms, most of these non-traditional, partially to completely westernized, and usually based on contemporary philosophy and modern scientific beliefs. (See my essays on Traditional Indian or Native American medicine, Indian Root Doctoring, its modified, Americanized form, ‘Transformation of Common Belief’ writings (see next) and my study of the phenomenology of plant medicines, to name a few.)
Unaniism is a form of medicine from the Middle East, in particular Iran, Iraq and India. Siddha is the Ancient Indian or Ayurvedic form of medicine practiced in India. According to wikipedia,”Kampo medicine . . . is the Japanese study and adaptation of traditional chinese medicine.”
Unaniism consists of the philosophy of ancient Greek medical practitioners merged together with certain Middle Eastern traditions and practices. Practitioners of these two philosophies believe in the humoural theory for nature and their practices involve the classical four elements theory. In recent decades, some Unani practitioners have likened their methods for treating mental health problems to practices akin to homeopathy. Others focus on the alchemy of this methodology, as it was described by Rhazes and Avicenna (Ibn-sina).
The practice of Ayurvedics has a much larger following and by the 1980s became a standard part of the “alternative medicine” world in Oregon, although classes were not taught at the local NCNM.
Kampo books appeared in the Oregon College of Oriental Medicine (OCOM) library as early as 1992/3, but it is possible this philosophy has been taught, although informally, as long as there were teachers for Traditional Chinese Medicine (TCM) at NCNM (TCM started about 1982/3/4, acupuncture was reviewed and taught and NCNM and its “sister college” for the time, the Seattle School (today John Bastyr), since the mid-1970s).
Like the chinese practice of acupuncture, these forms of therapy along with TCM may in the distant future become integrated with regular medicine. Some contemporary health insurance programs do allow some of these non-allopathic practices to be covered. In addition, there are ways in which the local non-allopathic physicians, serving as partners in a profession run by a regular M.D., do manage to provide certain services that are covered by typical health insurance programs. These are few and far between, but do provide us with case evidence suggesting that such coverage is possible in the distant future. The advantages of these practices of course are reduced cost and reduced stress upon the regular M.D. run health care system. The first of these advantages is lost if these new additional services are not provided as substitutions for more costly allopathic services, much like acupuncture is used to less the cost for managing drug abuse or chiropractics the costly need for pain management medications targeting cases of lower back pain.

Mapping Therapeutic Prayer and Religion. Therapeutic prayer is what the term implies. It is the use of praying as a part of the healing tradition. Prayer becomes a part of Public Health in numerous ways, but one of the most important ways in recent years and decades has been in reference to its use for curing or improving the lives of other people, usually in the form of prayer, but also by way of engaging in meditation, group chanting accompanied by prayer, or various forms of thought related practices and behaviors such as visualization processes, blessing a person’s home, providing some unique form of aromatherapy to a place, or engaging in some form of metaphysical cleansing activity, to name a few. Self-imposed practices are also methods for trying to induce betterment or a cure, by way of engaging in activities related somehow to the mindbody experience so often associated with the ability of such practices to make an individual better. The Pacific Northwest, due to its long history of engaging in traditional and non-traditional, religious and non-religious, sectarian and non-sectarian methods of healing, has a very strong cultural heritage that is unlikely to be dismissed from the local population’s health and medical practices any time soon.
During the early 20th century, Christian Science formed the longest list of alternative healers in the early Portland business directories. These directories bore numerous unique “healers” but none so popular as Christian Scientists whose offices were placed conspicuously in close proximity to the Good Samaritan Hospital in the Northwest district of Portland. At the time, the administrators of Good Samaritan even had some affiliations with these healers, and as thoughts were passed back and forth between Good Samitaritan nuns and nurses and the local spiritualists, the doctors, mostly men, were engaged in their own escapades trying to promote and encourge growth of their facilities. By now, endocrinology and other tissue and organ related medical specialties had emerged. Cancer was still very misunderstood and mistreated. But the germ theory had finally won over most of the members of the profession. Only a few “stubborn” non-allopaths remained to promote their opposition against the germ theory, with most of these still adhering to homeopathic beliefs. By the end of the 1950s, this listing of names of Christian Scientists was dropped from the directory, perhaps for a variety of reasons, but in part due to their development of Christian Science facilities like libraries for practitioners to use and the curious to turn to in times of need. On and off, science continued to reduce the numbers of followers, anti-evolutionists, and drugless medical practitioners. The practice of praying for cures went back to its traditional Biblical history and use, and even then regular doctors tried to assign scientific cause to diseases “cured” by Jesus and others, providing diagnosese for diseases that were very much unlikely, and then modern diagnoses were given to diseases that should have been very rare for the time.
The largest revival in prayer-based healing came at the turn of this century, lasting through most of the first decade of the 21st century. As a part of this revival in prayer as a means for cure came a revival in other practices as well devoted to quantum physics or energy philosophy, touch healing, and metaphysically based healing practices (see my history and review of this for starters). One of the more influential groups in the immediate Portland area of the Northwest, but rarely discussed for its relationship to health, is the Sufi movement. The most popular Sufi movement in Portland is devoted to the famous dance/meditation practice and exercises in music, prose and poetry. The most medically applicable sufi movement and group in Portland is devoted to the teaching of Sufi Pir (akin to Prophet) Murshid Hazrat Inayat Kahn and his successor/youngest son Pir Vilayat Inayat Khan. (The current successor whom I’ve met is Pir Inayat Kahn.)
All of these had philosophies with strong resemblances to those behind religiously minded prayer based healing practices. Accompanying this revival in spirituality based medical thinking were more programs and classes devoted to such allied events, experiences and practices as distant prayer, sufi medical practices performed by small groups, and undergoing the “exceptional human experience” (Rita White’s philosophy). The notion of “Divine Intervention” was no longer the only explanation given for these events when they happened, and as is often the case, such Miracles have their ways of developing new followers and new faiths.
The metaphysically-minded faiths and their ceremonial places or churches have been more frequented and heavily attended in recent years, such as the local Quaker, Christian Science and Unity churches (a 3+ year qualitative-quantitative study I did from 1997-2000) and a number of popular Buddhist outdoor retreats. These revivals influence the Pacific Northwest more so than other places at times due to their complete and total impacts on society as a collective, a movement that takes places along various avenues. Unlike other places with important and often very strong and highly respected religious beliefs and faith, and unlike the hamlets of the Shakers, Mormons, Amish, and Hassidics in the Eastern United States, or the 7th day Adventists, Hutterites, spirit rappers, and numerous utopian groups residing in rural settings of the Far West, the various urban sections of the Pacific Northwest are quite diverse and eclectic in nature, more so than these local congregations as well as much of the rest of this country. This makes it very likely that nearly every patient in the Pacific Northwest, even atheists and agnostics, will have some sort of metaphysical mindset or perhaps spiritualist approach to maintaining their health and attempting to resolve a health related dilemma. Be these actions taken personally or through friends and family, whenever health care is involved, some sort of metaphysically based and even mindbody based methodology is available for use to any and every patient in this region. Just how these faiths become a part of the regular medical practice is a major topic with need for further evaluation as part of any future Healthy People set of activities.
.
Mapping Medical Traditions and Philosophies. The physiography of the Pacific Northwest gave rise to a number of additional ways of treating illness that to date are never really appreciated in designing health plans. The most controversial of these is herbal medicine, which has a long history of allopathy-driven controversies and disagreements. The other alternatives with similar criticisms but less arguments pertains to the simple practices of homeopathy, aromatherapy, color therapy, art therapy, and numerous other practices which make use of concepts and theory instead of the controversial intake of chemicals. Then there are those chemically driven alternatives like the promotion of Cannabis use for improving the quality of life, the engagement in outdoor recreational activities to improve physical, mental and emotional health, the notion of buying more organic goods from local farms that make no use of chemical fertilizers or genetically modified products, or one’s involvement with very controversial treatments like weekly coffee ground enemas, prolonged periods of fasting, or self-imposed addictions to certain herbal products like licorice root (a source for endocrine-like problems) or the highly controversial comfrey and western coltsfoot herbal formulas (both sources of liver problems, especially when taken with certain prescription drugs).
In 1987, the medical botany officials at the local naturopathic group approached me as a toxicology expert and we designed a method for evaluating herbal medicines as potentially toxic agents. This was to avoid seeing any arguments arise due to interactions between naturopathic and allopathic medications, or patients overall health and use of the more chemically rich herbal medications. I relied upon the association between plant taxonomy, phytochemical pathways, and types of patient needs to design a ‘toxic syndrome’ or ‘toxidrom’ database. This data was then used to produce the database IBIS, produced and marketed by AMRTA.
In Oregon, the most important medicinal herb in the Pacific Northwest with regional connotations is probably Oregon grape at a cultural level, cascara at an economic level, yew tree at an economic and modern ecology level, and devil’s club at some post-modernist, alternative medicine level. But there are others that were highly influential on local health that have since been forgotten. Each of these were carved into the glass at the Light Rail station west of Downtown Portland at the Tuality stop (artist Jane Kies’s work entitled “Quilt of Traditional Remedies”). Back in 1991, I was asked to identify the most important plants in local medical history for the area. This was also the time I began to view plants as having a cultural significance, the knowledge of which was in serious need of preservation. The most important plants were then defined as including an umbel family member. Two years earlier, I also identified Thalictrum as being very important due to its cancer treatment potentials (thalictrine/thalicarpine analogs), as well as incense cedar (Calocedrus) with its testicular cancer drug desoxy-etoposide. In between, I identified 50 species of plants that were presented at a meeting in Salem for the Pacific Northwest Natural Products Industry association then forming, resulting in the development of a permit program limiting the harvesting of these resources in Old Growth forest settings from 1992 on (beginning with the taxol industry).
Herbal medicine is a mass marketing industry that has the greatest impact on economy and ecology in the Pacific Northwest, and more than likely nationwide as well. Such a large field of practice is barely reviewed, managed or covered by traditiona health insurance programs and agencies. This lack of involvement represents a turning of corporate heads in the wrong direction when it comes to providing adequate health care services. There is adequate documentation of this part of a patient’s medical history but inadequate utilization of this information for improving upon preventive care related services and reducing overall costs for services. Such an ability exists and the better trained professionals available for these services found practicing and being trained to be an ND in the Pacific Northwest, yet such an intergration fails to exist in most Pacific Northwest health care programs. Since the bulk of those people covered by health care engage in these activities, they are not provided with the best possible health insurance out there. Since large numbers of the uncovered population make use of these ‘alternatives’ there are equal costs to the long term care system being accrued as they continue to receive less than optimum forms of health care.
This integration of knowledge produced by the alternative practitioners and researchers lacks any unbiased work performed by the allopaths. In general there has been this tendency for allopathic professions to focus on the minutia of what makes a plant bad, with total disregard for the same problems related to prescription drugs. In 1989, a potentially hepatotoxic herb could be sacrificed for example, at the risk of turning one’s head and allowing for maintained use of a highly toxic halogenic derivative of ibuprofen. Bacterial end-products derived from wood pulp (microcellulose) were recommended over the more common psyllium products and lactobacillus cultures recommended by naturopaths and nutripaths.
.
Mapping Healthy Outdoor Places. When I first moved to the Pacific Northwest, two geographic features stood out as being health-related for the region. The first was the commonness of springs of various forms, but mostly the hot spring of places like Bagby formed by the volcanic nature of this region and the nearby sulphur springs facilities at Carson, Washington. My second observation was the nature of the Pacific Northwest shoreline topography and its landforms. Besides a line of volcanoes found well inland there was the coastal range, and the large cliffs and rock-formations lining significant portions of this state’s western shoreline. On a perfect day this meant that you could climb a pair of mountains (Twin Sisters), visit the beach to plunge into cold water (Long Island Beach, WA or Astoria), and then spend the evening engaged in an hour long hot tub soak and towel wrap before staying the night in a rustic cabin with minimal heating facilities.
Prior to this more modern, pseudo-utopian concept of health and the outdoors, there were the trappers I mentioned earlier and their interpretation of the wilderness as a means to clear the mind of all your emotional problems and, in the case of consumption, cleanse your body of whatever ailed you. To the earliest post-Grahamite followers, the early vegans and water curers, besides Graham bread there were local herbs to stock up on in case a cleansing of the blood or bowels of its “toxins” was needed (or so was believed). When water cureés made their way into this region in full form between the late 1840s and early 1850s (see my pages on this), the appearance of a place had everything to do with health and how these new settlers chose to live. To the Finns and Swedes, Astoria was the place to be, located close to the ocean’s shores and local equivalents for fjords formed along the Columbia River. This was the place for hot dry saunas to be built and a large dance floor and eating place set up for the weekly dances. To post-trapper period generation Northwesterners, Carson Hot Springs in Carson, Washington was the place to go, with its lumberjack like appearance and strongly sulphur-smelling vapor-filled white-tile hot rooms and white enameled tubs.
.
The utopian point of view of the Oregon coast was not just a trait of early 18th century French and Metis trappers or the occasional early 20th century travelers and Scandinavian immigrants. Throughout the mid-1900s there were various vacation places built, along with summer retreats full of cottages. In the 1980s, these cottages rapidly became permanent places of stay for the locals, especially those disabled and/or retired. By the mid-1980s, these same retreats became the first home-care facilities in the nation, a traditional open-house behavior transformed to meet the needs of the AIDs victims facing just a few months of life left to live.
.

Mapping Subcultures. The subculture way of life is rarely noted in medical records, yet this is perhaps one of the best pieces of information one can document about a patient. The standard clinical office environment with regular medicine prevents the nuances about patients from ever being adequately documented. This lack of information between doctor and patient increases when the overall amount of time per year that the primary care provider shares with a patient amounts to less than 60 minutes or one hour. This number pertains to the actual amount of time spent in face-to-face conversation with a fair amount of information sharing.
In one job I held I had to evaluate the services of a suburban clinic engaged in provided medicaid/medicare services as part of its Family Medicine program. This office had a patient that requested services for only urgent and emergent care. For each of the two years that I reviewed this clinic’s operations, this patient had no visits, but had a year long supply of refills offered for each service year, and one blood test per year. This patient was a white man over 65 years of age. The data for this man’s social life, diet, way of preventing or treating diseases represents about the same amounts of personal, social and non-medical related knowledge physicians have for most of their patients.
The subculture we place this person in varies from one judge of personality to the next, and the medical status this decision may in turn result in may vary substantially from one office worker to the next. In most situations, office workers have conversed with by phone or even seen this individual and so have a fairly accurate opinion about this patient’s social and mental health status. Such is not the case for insurance companies. For this reason there are only a few limited ways that insurers can actually know the subcultures of their membership or patientloads. It is the subculture that impact life related behaviors and conditions like BMI, blood pressure, regular use of street drugs and medicines, sleep behavior, and recreational activities. Without knowledge of each patient’s physique, behaviors, work and play activities and overall persona, a company has a difficult time categorizing the health of a patient, yet this is exactly the way these companies carry out such practices.

Mapping Mixed Medicine. There are two distinct points of view of the health of the poor and disabled in the Pacific Northwest. There is the point of view experienced by those who must live this life, and there is the point of view held by those not enrolled these programs, including the practitioners and many workers of the health care field as a whole. This duality stands out even more the Pacific Northwest than in other ports of the country due to the unique nature of Pacific Northwest alternatives. Few of those in the regular health care field have a complete understanding and experience regarding what it means to be poor, in need of care, making use of such non-allopathic techniques as the chiropractor, the naturopath, the homeopath, the chinese physician, the hydropath, the nutripath, or as Rev. John Bovee Dods put it during the late 1830s and early 1840s, the aeropath and terrapath. Yet these philosophies do exist in the Medicaid and Medicare communities, on behalf of individuals who rarely share this sacred piece of knowledge about the inner psyche and persona with their regular doctor.
Whereas earlier in Pacific Northwest history, mixed medicine was when the chiropractors and naturopaths both learned to become “drugless physicians”, a time when these two groups were forced to split into two separately administered non-allopathic health professions between 1945 and 1955, in modern medicine, this use of “mixed medicine” here has a much more complex meaning–and is something slightly short of integrative medicine. It can refer to the differences between regulars and irregulars, farmworkers versus non-farmworkers, hispanic versus non-hispanic, the healthy versus sick, the chronically diseased versus acutely ill but otherwise very healthy patients, the educated versus uneducated, and once again, the rich versus the poor. It also represents the traditional practices of two forms of medicine by patients with important needs. These patients see their regular doctor, but rarely share much of their experience with the other healers with that MD. Vice versa, it is not so much the case.
During the late 1990s, for a short while as a part of Portland’s Health Care Medicaid program, a fairly large complementary medicine care facility was opened, with many non-MD doctors (esp. NDs and DCs) and PAs trained as well the non-allopathic fields. This MD-managed health care program approximated the integrative care concept, but lacked the completeness and originality needed for it the become a prototype for other health care clinics and the like for the region. Such a dual purpose health care program never developed.
There is even more to this duality at the Pacific Coast/Pacific Northwest versus non-Pacific Coast/Northwest level naturopathy profession when we look at everything west of the Rocky Mountains. Naturopathy is known to be a licensed accredited medical profession along the West Coast. East of the Rockies, even as far west as Denver, this field of study is still publically interpreted as alternative, unaccredited form of medicine. This is due to the other form of schooling in this profession that exists back east. This misunderstanding of the meaning of this medical specialty–naturopathy–exists due to the existence of non-licensed naturopaths trained and qualified to preach and practice by way of mail order techniques. Adding to this problem is the use of the abbreviation ND used by naturopaths, which in theory is equivalent to the MD pretty much in terms of accreditation requirements for the west coast schools, but not the case for all other methods of training in this country.
As if this were not enough, there is also a division between east and west in terms of overall knowledge of the field. Even amongst non-physicians, such as university professors, an east coast “expert in herbal medicine” at the academic level typically has a superficial understanding of the plant medicine as part of a profession, unless he/she has taken the courses these accredited schools provide. Additional evidence for thisclaim is found quite easily through conversations–if you were to ask such a professor the difference between New York naturopaths and West Coast naturopaths, chances are they would not be familiar with the west coast schools, or the certification and accreditation histories of each, and would certainly not know the differences in their curricula.

Mapping Sequential Occupancy. Understanding the traditional sequent occupancy theory for regional development is applicable to the Pacific Northwest in terms of understanding population health research for the region. As noted in my ca. 2000 thesis, the sequent occupancy way of interpreting a place, its development and related changes over time has a valuable application to public health mapping. Each of the stages a region goes through has specific health risks attached to that place and time due to the natural and human ecological events taking place.
In the most basic of settings, natural diseases are a consequence of the environment, human behavioral patterns, and human activity. Older more traditional settings lack the problems experienced as a farming occupation develops, and zoonotic diseases become more possible and prevalent as the domestication of animals become more than just a family activity. As hamlets, villages towns and cities develop it becomes easier to spread certain contagious diseases within these setting, from one person to the next and one household or neighborhood to the next. Places which develop further and become more manufactory and technologically based in turn develop another set of diseases. In addition, this development has attached to it economic and human behavioral change, resulting in disease onset linked to a more available supply of drugs and alcohol, more exposure to chemical waste and pollution, more exposure within the occupational setting to specific toxins, teratogens, carcinogens and pathogens, increased risks for specific kinds of injuries and accident induced problems via the work place. As a post-modern living setting comes to be, human behavior again changes, diet becomes different, and life span is now substantially increased. As a result, older age diseases and medical problems are now setting in, like diabetes due to sedentary life styles and dietary change, and increased asthma problems due to exposure to the environment and asthmagens at an earlier age, more often in many regions linked to rapid urbanization.
Each of these new risks have addition costs attached to them. Whereas during the childhood years, costs are high due to initial diagnoses and preventive measures being taken, this high cost for services temporarily decreases as most people live through a relatively uneventful older childhood, and very healthy young to middle-age period of adult life (10 to 35 years old approximately). It is during these 25 years that we are most productive but limited in experience. So quite often little is done in terms of long term prevention. Those with chronic disease onsets initiating in their late 20s and early 30s typically engage in no preventive practices during the decade prior. Those with chronic disease onset in their 40s may often have some clues to their impending health problems, but also due to their energy and vitality tend to engage in various high risk behaviors.
![]()
Pacific Northwest Population Pyramids, Theoretical (for later discussion), based on Quarter Century Increments for the period of ca. early 1800 to present.
.
Mapping Epidemiological Transition. Epidemiological transition is a term used to define the changes in population health over time due to the major transformation of that population from one age-gender distribution typically associated with underdeveloped countries, to a population with age-gender distributions typical of a developed country with considerable economic success. This origins of this concept relate to a study in which the health and welfare of a developing country was related to the United States.
This study of the Pacific Northwest clearly demonstrates the kinds of changes in population health and regional health practices that have also been documented numerous times here and there in small pieces by other researchers. For this reason, I decided to apply the epidemiological transition model to my regional study, beginning with the assumption that regardless of the period of time during which certain events take place, there are communities like those of developing or underdeveloped countries and those like developed countries representing their various stages of development.
Epidemiological transition theory usually has a spatial component that remains constant, and it is time that has changed the region, which is then compared with all others. For a variety of reasons the official boundaries of some countries may change for political reasons. For the most part however, this way of understanding a population and its general health status makes this theory a valuable tool or point of view for researchers to trying to understand the health of a large region or given large number of people within the same country or political, governmental boundaries.
For such an approach to the use of this model, several different side routes of analysis may be taken, and applied differently to the different population groups at hand to better understand their health status and its relationship with the age of the group or nationality evaluated with regard to time. This already done in some ways when we look at the health of the lower class versus the health of the upper class, and the health of blue collar workers versus the health of farmworkers and the health of white collared workers.
Epidemiological transition begins with the standard population health modeling data used by the World Health Association. Metrics like average age, counts of people by age ranges, age of marriage, age of death, fecundity, etc., all managed on a per gender, per defined area basis. To this series of classic metrics I added my own focus on one-year age ranges, and then applied this to specific disease types as defined by their ICD 9 identifiers.
The following pyramid illustrates a theoretical relationship that exists between cost and age-gender counts. This model is defined as theoretical for the purposes of this discussion, but in many ways it does present a fairly accurate demonstration of the relationship that exists between cost and age when it comes to health in general. The one thing to keep in mind with this illustation is that the cost relations for each gender in relation to each other are probably more theoretical than actual; my intention was to underestimate these relationships I speak about.
The relationships are accurate for each gender cost relative to each population age count for the same gender, but between genders, we know that this equal cost relationship probably doesn’t exist. There are certain age groups for women for example when specific services cost much higher than comparable costs for men, for example a woman seeing per primary care provider, often a gynecologist rather than a family pracitioner or internal medicine physician, for her annual visit, versus a man engaging in the same but not visiting a specialist. Similarly certain visit costs and the related treatment can be higher for men than women due to a variety of features, ranging from the likelihood of males receiving a much poor diagnosis and prognosis, to the long term impact refusal to undergo periodic screenings and visits will have on costs once the initial diagnosis is finally made, for example for hypertension, diabetes, asthma, or even cancer.
.

Cost versus Age and Risk (F=pink, M=blue)
It also helps to define what is meant by the above graph by the work “Cost”. Cost is not just a monetary value that is being assessed here. In fact, it is more accurate to view the cost curve as a measure of claims filed, when these graphs are used to evaluate the numbers of people being evaluated for the particular health condition these graphs are usually produced for. Cost is not identical between cases because the methods of charging a patient and an insurance agency are complex and involve formulas that are never identical between programs and coverage types. With claims however, a claim is almost always the same thing. (Although claims are now being linked together with other claims for various cost saving reasons, making this part of the analysis more difficult to make sense of at times.) Claims usually refer to either someone diagnosed with a condition, or being evaluated for possibly have that condition. The majority of claims for a single ICD are usually for confirmed or nearly confirmed diagnoses (‘nearly confirmed’ means one or two entries or visits away from confirmation; for example when a condition is now awaiting completion of the next involving a ‘reconfirm diagnosis’ step).
If we assume that even though costs vary between health care programs and coverage types, that these claims always have the same cost or pricing attached to them each and every time for a particular person, not for all people, just for the same person, emaning they do not change that much in costs from one month to the next.
Based on this last supposition, we can see there are two major periods of rising cost in people, in general (not for any particular ICD). There is a childhood related rule-out/confirm diagnosis and initial diagnosis cost, and a cost that exponentially increases at a certain point near the end of life, due to comorbidities now having impacts on each other and the costs for the long term effects of these diseases now resulting in either an increase in need for care and amount and type of service, and/or an increase in catastrophic events taking place such as heart failure, onset of uncontrollable dysrhythmias, serious disabilities, more serious seizures or hyperglycemic events, etc.
The primary lessons based on the shape of this graph are as follows:
- There are typical childhood risks that result in increased cost and at times result in diagnoses that can be linked to other medical events later in life that in turn result in high costs.
- The 12 to 25 year old age range is the lowest risk age group. Diagnoses and needs for care lessen during that time, thereby reducing costs even further.
- The 25 to 35/40 year old range is the preventive period, during which engaging in the appropriate dietary and lifestyle habits have the greatest long term effects upon your costs. The activities one chooses to engage in during these years, and those to stay away from, determines the cost and medical related outcomes of the years that follow, and in the long run, the quality of life once one reaches retirement age.
- Forty five years of age, plus or minus a few years each way, is often that period of transition. Some diseases do have later onsets, like degenerative diseases due to other forms of chronic disease, or diseases that have obvious age related links such as a diagnosis of recurring atrial fibrillation, multiple sclerosis, and recurring uncontrollable convulsive disorders.
- Reductions in total numbers of people and total numbers of people with specific diagnoses take place after the age of 45. Whereas during the decade or two prior to this peak age, opportunities for prevention and improvements in quality of life further down the road should be of primary concern, the decade or two after 45 is that period when prevention and maintenance must be engaged in rather aggressively. Each year such preventive practices do not take place can have the potential of increasing not only the number of serious events later in life, but possibly also increase the likelihood for a catastrophic event taking place between the ages of 55 and 64.
- The ages of 55 to 64 represent a time when high amounts of attention need to paid to providing preventive-maintenance care, for obvious reasons. The less this is engage in, the worse off health becomes in the period that follows.
- People living at the ages of 65 to 74 are typically in a maintenance-prevention mode (the order of priorities have switched). Maintenance serves to maintain the healthy state one is in, assuming he/she has already reached that state of mind and body. Prevention activities serve to reduce other complications and negative outcomes of comorbidities. This means that prescription drug adherence is essential, and all chances for complications due to prescription drugs or treatments should be avoided.
- 75+ needs no explanation; one is either in that quality of life mode suffereing from numerous medical problems, or has benefitted from whatever preventive practices they engaged in earlier in life, to the best extent possible.
What we learn about cost can be evaluated in an excel file or statistical analyst tool, but for here the simple dot matrix way of evaluating areas on a map is used. The assumption here is that the area beneath these curves (between the zero y-axis and the ‘n’ value line) will demonstrate total cost relationships, for comparison between each of the different stages in regional health status and need for services. With this assumption, three periods were chosen for review, and then evaluated for costs accured up to the peak cost line, after which die-off occurs quickly and costs for care rapidly disintegrate.

The above details are from population pyramid graphs 1, 5 and 7. Maximum costs are assumed to increase about 50k units (along the x-axis) ,as per above the 3 figures. Note: this cost-claim curve is correct based upon a much larger study I performed as well. [F=pink, M=blue]
These demonstrate a theoretical cost relationship to age, allowing for childcare prevention and treatment costs to decrease over time and technological advancements, and oldest age groups costs to increase due to expected increases in chronic disease as the average patients’ ages for mortality increase. The yellow part of the area is what is evaluated, using a point grid mapping technique, resulting in the following point counts and therefore an estimated amount for costs with increases in costs for all age groups thereby evaluated. As the numbers of older people increase, costs goes up precipitously, perhaps doubling with every 50 years of change in population pyramid form based on the above 8 graph series.

The math for all of his will be provided later.
Repeating this for the rest of the 8 pyramids and then graphing the results produced the following:

According to the above, the changes in a population over time through economic development and modernization results in an increase in costs for health care due to an increase in size of the older population, when the older population is assumed to require an increasing amount of care and therefore increase in cost as the population get older. This conclusion is common sense of course, but illustrates the reason population pyramid exactness in shape and form can be helpful in assisting us with defining new ways to assess or predict changes in future health care costs.
This same theoretical method still has to be applied to more detailed assessment of Pacific Northwest population history. In addition, we learn more by applying this to the individual ICD graphs developed (see reviews beginning on another page).
.

Description of Figure: Population pyramid (left), with HEDIS/NCQA Study Groups defined by age-gender (brackets); the upper right table depicts age ranges for these studies (top chart, with age/years on x-axis, and each HEDIS/NCQA on y-axis), and the bottom right, a count of studies (y-axis) covering a given age range (x-axis). [Note: F=pink, M=blue; F=red, M=blue for third chart beneath the second]
Mapping Population Health Transformation. Population Health Transformation is the process engaging in the prior two tasks to review a given region’s stage in social development based on the sequent occupancy theory, combined with an epidemiological assessment of the population at hand, and its various subregions, niches, or nuances both socially and culturally. In regions like the Pacific Northwest, where individuality is sometimes the primary rule for survival within this setting, these differences people and small groups of people have from the west is very important to understanding where the population is going at a public health, epidemiological perspective.
People’s attitude, beliefs and behaviors define what they do whenever they are searching for a cure for whatever ails them at the time. These are personality features that simply are not shared with the physicians, and most importantly the regular or allopathic doctor. This lack of communications exists for a number of reasons. The amount of time spents by a patient with a doctor is a part of that picture resulting in the disconnect, but more importantly, the amount of quality time a patient spends with his or her doctor, on a yearly basis, is probably the chief deciding factor in determining if the doctor truly knows what medical issues are going through a patient’s mind and how he/she is engaging in healthy or unhealthy activities relative to that medical status or condition.
If one looks at the levels of people who provide us with health care, from the office worker on up to the allied health and alternative health professions, and then upwards further to the primary care provider and even our specialists, we find the latter two know the least about our personality and often the most about our physiology and anatomy. Our decision to drink ginseng tea may be shared with them and even entered into the medical records, but this information has no way to be adequately used without the right levels of expertise engaged in this part of the overall health care plan. This is where the role of the alternatives, turned complementary and perhaps even integrative physicians fits into the scheme of things with regard to providing high quality health care.
A psychologist or neurologist can try to help us manage our insomnia problems, and then send us to a sleep pathologist for some tests, and from there to a provider of a sleep apnea device to see if this improves our daily wakefulness and ability to perform. On the side, some of these patients may be even engaging in the classic herbal medicine plan for assisting them with their sleep, using the very classic herbs, but quite often to no avail. At the provider level, it is hit or miss as to whether the patient has been recommended a viable means for using herbal preparations to help one get to sleep. If you send that patient to a specialist who determines the reasons for insomnia are more complex and involve specific stages of the sleep cycle, he/she may not be able to correlate this with the herbal medicine being taken, and whether there are alkaloids, sesquiterpene lactones, flavonoids or valepotriates being taken that could in addition to causing unrest and GI complaints, also result in some liver related stress due to the interactions your regular medications are having with this change in therapy.
A complete alternative health assessment of the same person may be different, and may depend on the specialist in alternative, complementary medicine engaging in this evaluation. For example, a person train in acupuncture and TCM would have a very different philosophical take on your condition and its causes when compared with a homeopath’s assessment or an eclectic herbalist’s assessment. A water cure physician/massage therapist might offer some recommendation you hadn’t really thought about since they seemed too “old-fashioned”, like soaking your feet in the tub to reduce pain and begin to relax. A chiropractor might have a theory regarding your history of lumbago as a cause. A naturopath might take into consideration all of the above, and more, and recommend dietary changes (reduced coffee/soda/herbal medicine caffeine intake), meditation while lying in bed, aromatherapy and sound therapy. A psychologist (or even psychiatrist) might consider this an emotional, behavioral, neurochemical or even past life generated neurosis condition (you never know with the Pacific Northwest). All of these are techniques used to eliminate the possible problems, signs and symptoms related to the pre-insomniac period. A very similar methodology is used to eliminate one of the most common problems faced by Pacific Northwest patients–insomnia due to Sleep Cycle Dysarrhythmia–the problem one faces due to the biological clock not working due to work schedules in combination with reduced daytime solar activity exposure. Any and all of the above have equally meaningful theories and methods for treating the condition.
Population Health Transformation is simply allowing all of these possible methods of care to be made available and supported for each individual to make the fullest use of as they wish.
The current plan for assessing population health is to evaluate patients based on electronic medical records data, without taking these various other means for care into account. With electronic medical data, we have the option of either having more information and knowledge to assess regardless of how much of it is valid and how much is gibberish. In remote sensing, there is this way to analyze the surface of the earth based simply of color patterns for various wavelengths of reflection and absorption. The nonsupervised method is done by allowing the system to learn the differences and try to classify parts of the earth’s surface by assigning relationships between each one and its neighbor (the cell next door and its wavelength pattern), and others like it next foor or afar, with still more neighbors to take into account. Supervised methods of evaluating the same data require that we add a human touch to this methodology by overseeing how some of these initial building blocks are put together for the rest of the program to run. Supervised methods require knowledge and experience to be correct.
The up and coming way to analyze people health involves features from both of these methods. The big question is, can the new method differentiate personalities based on the clinical data. By engaging actual people in such a progam as focus groups, one can learn to find ways to define these individual differences, the differences between the punk rocker living on the street engaging in frequent cannabis use, and the gothic princess doing tricks every now and then and making use of vodka rather than coke.
To put Population Health Transformation into perspective with all of this, suffice it to say that individuals with experience at the street (“alternative”) and clinical (“traditional” or “allopathic”) levels for these outliers are needed for the best analyses to be performed. Their expertise adds more credence and more value to whatever methods are used to try to map out population health at the small area level, for reasons of developing very specific prediction modeling tools. Currently the idea is there, but the knowledge base needed to fully engage in such a task is not really there, that is unless the people employed to make these predictions are experienced homeopaths, with experience as well in dealing with the gall bladder meridan and that added knowledge needed to know the differences between when it is gu chi causing the gall bladder to have a problem due to some food the patient ate or more seriously a result of a diminished wen chi implicating some underlying chronic disease problem.
Population Health Transformation is making full use of your resources.

.
Mapping and Defining regions–the HEDIS and NCQA Regions. Before reviewing the detailed outcomes of Pacific Northwest health, it helps to look at the “regions” that have defined for understanding and testing population health that are presently being used. The U.S. has been divided into regions in several ways for statistical analyses. The Census has a method for defining areas of the country, and since this is a health study of the U.S. we can compare this with the standard way of evaluating national medical programs for this country–the HEDIS/NCQA methods.
There are two sets of studies out there that tend to portray their results with some relationship to regions of the United States. HEDIS studies are a standard for most large programs, and due to the national presence of HEDIS related activities, we have the opportunities to observe national health statistics in a large area or regional manner as well.
More illustrative of this potential means for evaluating regional health patterns is the work of NCQA. NCQA has pre-defined its regions, but unfortunately has left us with some fairly large regions in the western United States. The manner in which regions are defined relative to health always has an aspect that is related to cost for services and how it applied to the assignment of value process. The common perspective is that one region costs more than another for the same sort of service, for various reasons.
If this cost and consumer behavior related reasoning is ignored, then we can break the larger NCQA regions down into smaller regions or subregions, and then neighboring states in distinctly different parts of the US can be evaluated and compared. In this way, we can compare health care in the Pacific Northwest with healthcare in the Northern Rocky Mountain States and with health care in the Southern Pacific region or Southwestern US, an evaluation that can’t be managed using the NCQA method of comparing different regional health care delivery systems.
A simple view of the Census versus HEDIS/NCQA reveals significant differences between regions. One has to wonder which method is better, a method which focuses mostly on people and their primary age, gender and ethnicity attributes. or the other method which tries to define regional health behaviors and related disease patterns. Logically, we want to demonstrate favoritism towards the latter, and in the case of broadscale disease mapping, employing this method is not so much a problem in terms of reviewing large numbers of people.
A primary problem with population health monitoring is the ‘numbers’ issue. Too small a group and you have to wonder about the validity of the study results when using them to define some primary public health characteristics of a region. Too large a group and there is no problem with accepting the validity of the statistics, but then you have to wonder if you missed out on any important differences between sub-regions. This is especially the case when the area you have lumped into a single group is suspected to have significant differences in its content between the two opposing ends of that region.
Such is the case for the HEDIS/NCQA definition for regions. Population density and targeting numbers of people lead these studies to compartmentalize people’s health based upon mostly numbers of people in each group regardless of cultural backgrounds and regional differences. this problem is not so much the case for the east coast region of the U.S. as it is a problem with evaluating west coast populations. In the west coast, there are important latitude defined differenecs in health along the large regions defined and used for evaluating population health in the Rocky Mountain States between Canada and Mexico. Likewise, the west coast states are not only different from those of the Rockies due to population features, but also due to climatic and physiographic features, each of which play very important roles in better understanding disease ecology features.
But the problem with defining a west coast region as a unique entity pertains to its north-south differences culturally and climatically. The same differences between the Rocky Mountain and the Pacific Coast states exist as well in the Northwestern versus Southwestern states, as my disease ecology maps display later on this page illustrate.
The standard HEDIS/NCQA manner of reviewing the western most states also has its problems due to the artificial regionalization seen when the states of Alaska and Hawaii are both added to this region. For population sake, the low counts of people in these five states helps make a study of this region more credible due to higher numbers, but even for diseases strongly of a behavioral nature cannot easily be reviewed in terms of cause and effect once cultural background is taken into account. For example, with asthma and diabetes, two of the most prevalent chronic diseases in this country, one can hardly state comfortably and with much certainty that any findings made about diet and diabetes in Oregon can effectively be translated over to the same for California, Alaska or Hawaii. Likewise, the increase in asthma related problems complicated by allergy histories have no relationships that will match between any two states in this artificially assigned region. Therefore, better regions have to be established for cost effective intervention programs to be developed for these diseases in this part of the United States.
This also means that the HEDIS/NCQA method for evaluating disease patterns has limited functionality in terms of clinical effectiveness for some parts of this country. Yet, this same problem extends further when we review the regions evaluated for the Eastern and Midwestern states as well. In my study oif distributions for these regions, breaking them down into sub-regions and then comparing the sets of sub-regions to each other, the Southeast, Mid-Atlantic, New England, Upper Midwest and Lower Midwest portions all benefit by further segmenting these populations in order to improve our sociocultural methods for analyzing regional health patterns. This problem with large regionalization is accentuated by the differences between the Pacific Northwest and elsewhere in this country. Even within the Pacific Northwest, Alaska and Hawaii have to be removed from any standard study, at least in the beginning, since each does have an impact on the Pacific Northwest in general due to commercial and migrational habits. The only statements that can be made about an inter-regional association for Pacific Northwest states are that: a) Portland and Oregon are similar to each other, and too dissimilar with the southern populated settings of California, b) California, at least in its southern half, is more like the states to the east than the states to the north in terms of disease ecology history and spatial relationships, c) the area between Oregon and California has some overlap and in some cases can even be treated separately for certain disease analyses, like the study of recreational patterns and health or lyme disease and health.
[Insert Regional Study Maps]
Once upon a time I developed this way of redefining regions in the United States for population health research. By applying the above NCQA and HEDIS methods for defining regions, taking the Census Bureau method into account briefly, and then thinking back about my own experiences living in different parts of this country, I decided I had to break down the given standardized regions into subsets or newer regions. For the Pacific Northwest, California was to be excluded for the most part once detailed project management work came to be for regional public health, but for now I decided to map the three Pacific Rim Coastline states as a single entity to see what I could come up with.
Next, I applied some new formulas I developed to evaluate each of these regions of the United States and display this data on a single map. These maps were developed for about 300 ICDs, 50 or 60 of which were exceptionally good and told us a lot about diseases and their occurance in different parts of this country. These maps unknowing also provided me with my first highly detailed insights into regional health patterns that in turn led me to perform a more precise and complete mapping of similar data. That project resulted in the 3D images I produced and review later on this page.
The regional maps I produced for this country only review age-gender distributions in one year increments for the most important disease states or diagnosis. Many types of disease groups that I developed a classification system for were not included in this earlier project since I had not as of yet developed that taxonomic or nosological way of categorizing mappable diseases.
This work results resulted in the following broad area conclusions that relate to the large multistate portions of the United States analyzed during this phase of my research. Again, the focus was on developing a way to more accurately capture the regionlization concept for HEDIS/NCQA like disease mapping projects. The following methodology was used:
a) none of the studies in this step took ethnicity and culture into account;
b) all of these studies were performed by dividing the population into categories defined in 1-year increments for male and female age groups separately from each other, and
c) these were then displayed and tested using a population pyramid statistical analysis technique that I developed for comparing any two sets of outcomes (male versus female, region1 vs. region2, disease1 vs. disease2, etc.).
The following conclusion were then drawn immediately from this work; more detailed findings, along with the map illustrations, are reviewed in the next section:
- Florida and neighboring states have the oldest population in the country and will experience the first financial stresses induced by the needs of care by the old.
- The New England-New York area is demonstrating health care utilization behaviors that mimic those seen for Florida region for many of the same diseases. The older employee population age group demonstrates a statistically significant greater percentage of people under the age of 65 experiencing the same health problems as the Florida are residents. No other large multistate part of the country demonstrates similar findings.
- Several regions demonstrate significantly larger percentages of the population beaing a high percentage of mothers and children. This mother-child relationship is highest in the upper midwest near and around the Great Lakes and along the lower Eastern Atlantic Seaboard, with some evidence for a similar population health pattern existing to the north into Washington D.C. area as well, and perhaps another in around Texas.
- The Pacific Northwest population health states based on age-gender distributions portrays a region which is much healthier, with lesser problems that the rest of the country pertaining to the well known chronic diseases.
- Much of the rest of the country lacks specific outstanding age-gender risks indicated by large numbers of patients peaking or demonstrating statistical significance when its comes to having significantly more or significantly less for the specific age-gender groups that were tested.
East Coast-West Coast Regions. It helps to compare the Willamette Valley medical history with that of the Hudson Valley. These two regions bear similar human geographic features in that with the 18th and early 19th century study of New York, New York City was compared with those parts of New York extending from the Fishkill area northward along the Hudson River Valley. This approach is similar to how we can review the state of Oregon during the mid to late 1800s or even the early 1900s, for comparison with the country as a whole. This is because both of these regions were considered somewhere between borderlands and hinterlands in nature, places where the status quo suffered from serious competition and significantly different culturally bound philosophies and traditions.
[NEED MAPS!!!]
A Brewing Controversy
With regard to the Oregon experience in the late 1800s and early 1900s, it was the impacts of decisions made by the AMA on the East Coast that impacted west coast medical practices the most after 1900. Even with regular medical schools present on the west coast by the 1890s, many of the physicians trained in 19th century traditions and whom were highly respected by their communities lost their licenses due to these legal changes. The impacts of this on local politics and families are found in the meeting minutes and related articles posted in the state’s medical journal published during the late 19th century by the State Medical Society. In 1882, the younger doctors expressed concerns about their older relatives losing their rights to practice medicine.

Gordonskene. Healthcare’s Endless Saga – The Argument In 1949. March 25, 2011. http://newstalgia.crooksandliars.com/gordonskene/healthcares-endless-saga-argument-1949
More than fifty years later, from the 1940s on, one major force against the non-allopaths–Morris Fishbein, was busy giving his talks and making his rounds around the US trying to turn families away from the other forms of health care in use like homeopathy and eclectic medicine and back towards believing in allopaths and the hygienic movement underway. Results and recounts from these events were in turn were shared with the nation at large by way of a popular culture journal devoted to healthy living practices known as Hygeia. This family magazine was published monthly and had regular sections in it devoted to infant and child care and feeding, child-rearing recommendations, household cleaning and sanitation practices, news about common diseases and medical conditions, signs and symptoms to watch out for, how to behave when seeing your doctor, and the latest news on “quackery.”
By the 1960s, Hygeia managed to help allopathy secure a stronger place in its profession. However, this success was due more to legislative changes and public interest than any combined marketing successes. It was the end of the first half of the Cold War once the 1950s had passed, and technology was now beginning to take hold of the many professions and career avenues available out there. As the medical profession in the Pacific Northwest underwent substantial change from 1957 to 2000, the alternative medical professions in this state also became more secure financially and publicly. During the 1960s and 1970s, these schools (one Naturopathic School in Portland, the other in Seattle) remained active and managed to stay alive in spite of the progress regular medicine made when it came to discovering the gene, better understanding cancer, and coming up with new remedies for previously untreatable diseases. During the 1980s, there was this mild period of growth in the alternatives for indeterminable reasons, followed by another spike in growth in these professions during the late 1990s for reasons discussed elsewhere (the millenium movement so to speak).
Throughout this time, the Pacific Northwest population grew in size and complexity. Along with more people came more cultural diversity, forming regions with greater population densities. Larger urban centers and increased surveillance activities, formally and informally, led to more complex diagnosis and the definition of the disease patterns, many of which were evaluated for this project. These diagnoses related to poverty, poor living conditions, human activities and behaviors, mental health conditions, personal psychology related syndromes, and increases in the in-migration of people and foreign disease patterns. (This next section details these socially born and physiographically born or developed diseases linked to the growth of the population in the Pacific Northwest.)

Section Summary
When we view the medical geography/disease ecology (human and natural ecology) of health in the Pacific Northwest, a number of major themes pop out. Not all problems related to poverty occur together, nor are the expected problems related to climate, weather, socioculturalism, and other features by seemingly the same people found to be recurring in a region. Some very obvious outstanding social diseases associated with regions like the Pacific Northwest do stand out as such, and the moral messages these have attached to them are obvious. However, there are also conditions, behaviors and diseases that over time we have often felt are true Pacific Northwest problems, like the various diseases related to the lumber industry or the allergic bronchitis caused by mushroom growing industries.
There are also conditions that we expect to be primarily of a Pacific Northwest nature, like the onset of insomnia or sleep cycle irregularities due to the number of cloudy days, or increases in depression and suicide cases for a similar reason. Then there are these peaks in Northwestern disease patterns that come as a true surprise to disease cartographers, and it was the expectations that these conditions probably exist that led to my initiation of this project. The most common diseases such as diabetes, asthma, etc. are not reviewed here, due to their tendency to be well dispersed across all living spaces. Regional differences may exist for many of these, and the reasons for these regional differences fairly well understood and/or hypothesized, these are not covered due to the purpose of this project.
The purpose of this project is to determine if specific behaviors exist across time and space for specific disease types, and to evaluate those diseases most linked to either area, or people. The environmental diseases are mapped to see how place plays a role in their distributions. The human behavior and sociological/cultural linked diseases, conditions and behaviors are reviewed for medical sociological research reasons. A number of other unique forms of disease with social and moral implications are reviewed as well, including diseases or diagnoses associated with the criminal mind, and ICDs that have some sort of linkage to some form of human behavior (i.e. pyromania or pedophilia).
The findings presented on the maps that follow are not conclusive, nor are they valid for all time when it comes to Pacific Northwest medical history, They are valid for a time during the past ten years, and are indicators of how people behaved statistically in terms of the types of behaviors, medical conditions and diseases they manifested during the past generation or two.
It is also important to note that these national and regional findings pertain to the least usual medical conditions or behaviors, and are those types of diagnoses that often go undocumented or entered into hard copy and/or electronic medical records. There are also some general behavioral features of diagnosis that exist involving the doctor and the patient. In some cases, certain disease types are overcounted due to the use of a disease-indicating ICD code as part of the rule-out process in health care. This problem exists primarily in children and young adults between the ages of 10 and 25, male and female.
This next section reviews the maps in general. It is then followed by a section that focuses on Pacific Northwest issues.
.
.
To be continued . . .
LINKS TO NEXT SECTIONS . . .
Part IV – the 3D Mapping LINK
Part V – Pacific Northwest Maps LINK
.

Leave a comment