November 2014
Monthly Archive
November 27, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Map: Turkey density in the United States
The government actually keeps track of this.
Source: www.vox.com
Turkey Farms are actually all around the Country. A few years back I had the opportunity to photograph and evaluate a 200 year old farm that specialized in this poult industry, just before it was leveled for the building of new houses.
With GMOs such a hot topic in the press, and a major topic of concern due to the unknown impacts of genetically engineered foodstuffs on the human body, this has become one of my most frequently visited sites . . . .
“The James Way” of Raising Turkeys" at
https://brianaltonenmph.com/historical-buildings-and-sites/the-james-way-for-hens-and-turkeys/
Turkey farms and public health have a shared history that is totally forgotten. During the Sanitation Period in US history (lat 19th-early 20th C), turkey farms and many other livestock business settings were a major concern to epidemiologists. Tuberculosis was a major concern, and the crowding of chicks led to large numbers of deaths at times. This is when a major university in New York helped perfect the livestock veterinarian business, and produced a medicine that was administered to every new hatchling– Sulfaquinoxalamin. Evidence for this was found as inspectors’ tags hung on walls throughout the facility — these tags as "an aid in preventing outbreaks of coccidiosis due to Eimeria melengrimitis and E. adenoides.”
What was once a religious based tradition in just a small secular part of the colonies of North America had evolved into family business by 1900, and large businesses by the 1970s. The continued evolution of this cultural practice into megaindustries has changed it from a single culture behavioral pattern into an omnicorporeal cultural system, leading to the re-marketing of these teachings in the U.S. to further satisfy the needs for all cultures, be they Native American, Christian, Jewish, Muslim . . . ad libitum.
At my personal blog site, I provide a unique perspective of the history of this industry and how it evolved from small private farms to large factory settings in the Dutch cultural settings of Hudson Valley, New York. The interpretation of the Turkey farming industry takes a very unique sequent occupancy approach to demonstrate its impact on the various periods of US-American cultural and economic growth.
This is one of my most common sites for elementary to high school teachers, especially this time of the year.
See on Scoop.it – Medical GIS Guide
November 26, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Bouttenouse Fever – YouTube
https://www.youtube.com/v/n5uECNUBRgw?fs=1&hl=fr_FR
http://youtu.be/n5uECNUBRgw BouttenouseFever 7 0803 0%
Source: www.youtube.com
I mapped some of the rarest diseases associated with in-migration of infected people, animals, hosts or vectors a number of years ago, soonafter successfully mapping the in-migration pattern of west nile and using this to employ GIS in identifying the location of a positive testing nidus based on a grouping of host and human cases within a 5 square mile area.
This collection of my 3D videos includes coverage of the following fairly rare forms of geozoonotic diagnoses:
Bouttenouse Fever – 0:22 |
North Asian Tick Fever – Asia-Russia – 0:21 |
Queensland Tick Typhus – 0:23 |
Creutzfeld Jacob, IP – 0:29 |
Crimean or Congo Fever – Asia – Russia – 0:41 |
Guama Fever – 0:29 |
Yakatopox- 0:28 |
Omsk Fever – 0:27 |
Guinea Worm -0:25 |
Ratbite fever, ip – 0:36 |
Foreign zoonotic diseases (aggregrated, depicting in-migration routes)
See on Scoop.it – National Population Health Grid
November 25, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on 4 – Sociocultural Disease Clusters
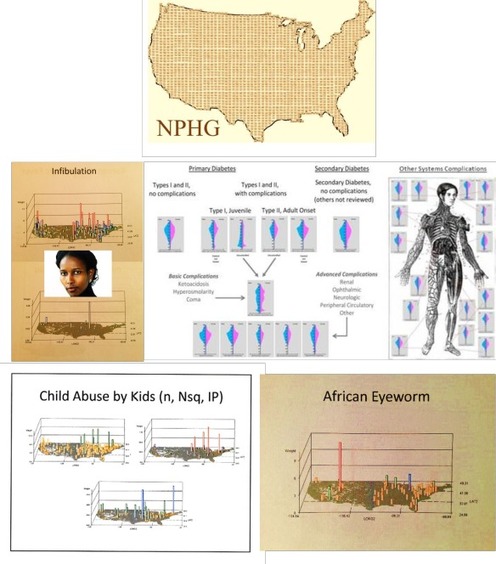
The woman in the poster board like collage is Ayaan Hirsi Ali. She wrote a book detailing her infibulation experiences which helped to improve the social awareness about this controversial traditional African Muslim practice.
Source: nationalpopulationhealthgrid.wordpress.com
This is one of several applications for GIS to medicine which I promote with regard to my NPHG approach to analyzing population health.
Investigating sociocultural disease patterns is one of the most valuable uses for spatial epidemiology within the managed care setting. It may also soon become the most controversial as we begin to point the finger at certain racial, ethnic or cultural causes for certain disease patterns.
Four classes of "foreign diseases" are defined on this page.
We are most familiar with just one or two of these classes, and spend little if any time investigating the remaining sociocultural issues in public health.
See on Scoop.it – Global Health Care
November 25, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on In the medical response to Ebola, Cuba is punching far above its weight

165 health professionals from the country arrived in Sierra Leone on Thursday.
A related question to ask is
‘could Cuba in turn be impacted by the return of a physician who does not know he/she is infected?’
Source: www.washingtonpost.com
Cuba has an excellent healthcare system, and has taken steps that outshine many of the other country’s attempts to deal with Ebola.
This has certainly been a feather in the cap so to speak. But the next questions we all have to ask, the same that all other countries sending help need to ask as well, is how might this put ‘Us’ at risk back home?
The point here is not to stop any international aid that is taking place due to Ebola. The purpose of this posting is to more strongly state the criticisms out there about how borderline the success of preventing the international, intercontinental spread of Ebola has become.
Cuba’s problem, were Ebola to enter the region, according to my opinion (based on studies, but still an opinion), is that Cuba has that additional factor to contend with regarding possible Ebola migration and penetration. Cuba has some high risk community settings due to low income related living conditions. The rural neighborhoods in particular that are low income have additional risk factors to consider, such as the natural climate and topography settings that helped Ebola travel its paths over the decades in Africa, through both southern and northern hemispheres. But there are also the vegetation settings and animal spatial ecology patterns to consider. The potential hosts, carriers and the like are there in the Cuban setting. There is enough rural territory, with rolling terrain and highly varied microclimate settings, to make it possible for a parallel to the African tropical nidus to be discovered in a part of Cuba. That is the heart of the matter in terms of Ebola and its potential for migration to Cuba.
Cuba is an isolated region, like Iceland was for the various Measles epidemics that have been researched there over the decades. One of the last things Cuba needs is for Ebola to reach its homeland.
The Cuban economy and healthcare system are generous in what its people are are doing right now, participating in the Ebola epidemic response programs. So, it is up to WHO and CDC to develop a more effective, prevention-minded program in order to prevent an accidental transportation of the disease to other places.
The Cuban healthcare workers are no doubt more alert to this problem of possibly travelling with Ebola by accident than even the international and governmental groups seem to be. But the repeated migration of isolated cases, from one area to the next for other countries (including the US), isn’t comforting when a disease highly epidemic due to its natural ecology becomes a passenger finding its way to a new nidus or "hot spot". The climate, topography, zoology, ecology and latitude and longitude for Cuba are right, making it possible for ebolavirus to become ecologically stable within this new setting.
See on Scoop.it – Episurveillance
November 23, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Introducing Unani Medicine to the United States
http://docs.google.com/viewer?url=http%3A%2F%2Ftodayspractitioner.com%2Fwp-content%2Fuploads%2F2013%2F11%2FUnani-medicine-pt-1IMCJ113_Golabadi_24_30.pdf&embedded=true
Source: todayspractitioner.com
Since 1985, there has been an active attempt by just a few of us researchers to better understand Unani medicine.
Unani medicine is now ready to expand the popularity of its practice in the United States (see links below), much like the practices of Caribbean African-American did about 20 years ago, in parts of the Southeastern and Southwestern United States (i.e. African herbalism, divining, spirituality, voodoo, hoodoo, etc.).
Unani medicine has two cultural links–India and the Middle East (mostly Iran and Iraq).
The social settings with the longest history of Unani practice are probably in the New York-New Jersey region, where they first developed storefronts and clinics devoted to this healing faith.
There are a number of features of Unaniism that make it attractive to western medical patients. Unaniism has a unique philosophy on personal, culture and mental health, attractive to some in much the same way that homeopathy, aromatherapy, shamanism, traditional chinese medicine and drumming have become popular culture complementary-alternative medicine (CAM) ways to treat certain patients.
The following are additional sources on Unani practice:
I focus extensively on Unaniism at my Pinterest page devoted to International Health at
http://www.pinterest.com/altonenb/international-health/
and use it to demonstrate mixed research methods (combined qualitative/quantitative for PIPS and QIAs) at:
https://brianaltonenmph.com/biostatistics/grounded-theory/combined-qualitative-quantitative-methods/
Benchmarks for Training in Unani Medicine (WHO) — http://apps.who.int/medicinedocs/documents/s17558en/s17558en.pdf
Links to Unani Medicine Sites — http://www.globinmed.com/index.php?option=com_content&view=article&id=99862:links-to-unani-system-of-medicine-and-related-websites&Itemid=186
WHO and Unani growth and development — http://www.unani.com/who%20&%20unani.htm
See on Scoop.it – Global∑os® (GlobalEOS)
November 20, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on 2014 Ebola Outbreak in West Africa – Cumulative Reported Cases Graphs | Ebola Hemorrhagic Fever | CDC
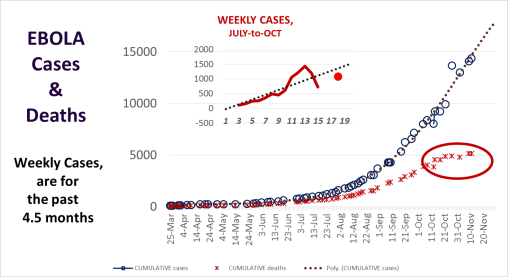
The rates of cases are certainly plateauing. This CDC site — 2014 Ebola Outbreak in West Africa – Cumulative Reported Cases Graphs — has a review of the cases as they behaved in different countries over the past several months.
Source: www.cdc.gov
I posted a statement claiming that plateauing had commenced about a week ago, with the numbers evidence for my claim (although early, after just 2.5-3 weeks of leveled numbers in a row). A number of months ago, my model stated this would happen in mid-October, which I correct the the end of October a month later as more weekly values could be evaluated. My model suggests complete reductions due to a saturation of the population, resulting in an impact of the most susceptible followed by a loss in diffusion potentials. This assumed there is no new population impacted, located in a very different part of the world like Europe or the United States.
The model I use is a very basic deterministic model, which accounts for systems behavior, not innovative diffusion patterns like the more stochastic/probabilistic models like to depend upon. Since Ebola is in its first pre-pandemic period, this is very much like the first years and diffusion of the earliest Cholera pandemic year–1832 about. Models of that disease pattern published in the 1960s and 1970s demonstrated that a non-hierarchical behavior prevailed in the way the disease impacted the rest of the region infected.
The second time through however in 1849/50 demonstrated a hierarchical diffusion pattern, in which the disease traveled great distances and impacted newer, uninfected populations far away from the source. The future of these hierarchical diffusion processes are predetermined by certain human and natural ecological features, a product of the pathogen’s evolution and ecological history, in combination with climatic and seasonal weather patterns (in the extreme sense, El Nino and global warming impacts, latitude-linked isothermal lines, and the like). Human migration helps the disease to spread, but its potential for become endemic to a region or naturalized is almost completely environmentally based, and heavily dependent upon zoonotic features (for both Cholera and Ebola).
See Gerald F. Pyle’s Applied Medical Geography (Scripta Technica, 1979) for more detailed applications of this method for analyzing spatial disease patterns.
See on Scoop.it – Medical GIS Guide
November 19, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
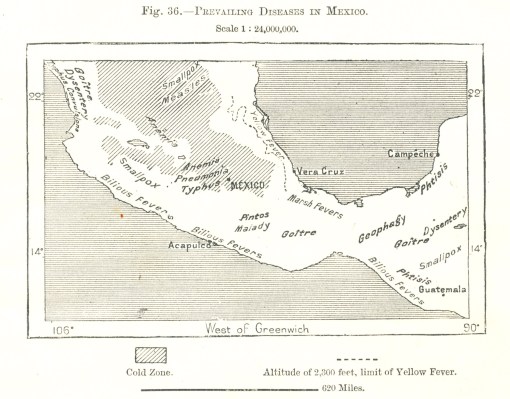
Comments Off on My Most Popular Site: “Central Mexico Disease Geography (ca. 1880)”
Why is my site with a map devoted the health in Mexico the most popular?
How much will the rise in Hispanic culture medical needs impact U.S. healthcare system over the next decade or two?
What does a 125 year old map of the health in Mexico tell us?
This map is from my most heavily visited page to date on my blog devoted to historical medical geography, spatial epidemiology, cultural medicine, and the history of medicine. (My site surpassed the rate of 100,000 hits per year, or 65,000 people/year, a month or two ago).
Source: brianaltonenmph.com
This above map is found on p. 91 of THE EARTH AND ITS INHABITANTS NORTH AMERICA, Vol. 2, by the famous French Geographer Élisée Reclus (1830-1905).
From 1875 to 1894 Reclus published one of the best known series on global populations, a 19 volumes series on "Universal Geography" entitled La Nouvelle Géographie universelle, la terre et les hommes.
This version of the map however comes from another book by Reclus (probably in Universal Geography as well)–THE EARTH and ITS INHABITANTS. NORTH AMERICA (New York by D Appleton & Co., 1891).
According to a population density map contained in this volume (Fig. 71, p. 171, The Density of the Population in Mexico"), the densest population at the time was the darker (cooler) region where anemia, pneumonia, and typhus are mentioned, just north and northwest of the label "MEXICO."
I produced a fairly complete explanation of this map years ago, accessible at my personal blog site (https://brianaltonenmph.com/gis/historical-disease-maps/centralmexico/ ).
The popularity of this map suggests my site is heavily visited by US students and professionals interested in Mexican/Hispanic culture and how this impacts local medical geography, our current health care needs, the history of health related needs amongst Hispanics and their communities.
The popularity of this page also sends an interesting message to the medical profession.
It popularity may also be because members of the Hispanic communities in the United States have a growing interest in their own heritage, or because non-Hispanic people want to learn more, or because meeting the needs of the Hispanic patient is perhaps one of the most important cultural health issues to date in the US healthcare system.
Whatever the reason, we also know that the history and geography of Mexico and Central America are popular topics for classes taught in schools and colleges across this country. One of the least discussed parts of this aspect of American history (all 3 or more Americas) is the long term impact of a rapidly growing Hispanic culture on the United States healthcare system.
Like the American Indian public health dilemma, there are a bunch of popular impressions taught about Europeans, Hispanics and the Indigenous that are not completely true.
These two cultures had impact on each other, in such a way that this topic cannot be taught effectively in any single college level program, except as a discipline.
In terms of medical history, the history of New Spain health is more than just a story of how Europeans wiped out so indigenous groups through the communication of small pox and measles. There is also the tale of how certain venereal diseases were brought back to Europe by sailors venturing deep into the woods of the New World, a New World blessing for the social elite back home. (Diseases do travel both ways, from culture to culture.)
Reclus covers but a small part of this history, mostly superficially, but most importantly, with a focus on Native Mexican-American Hispanic cultural diseases, not on the other diseases that strike this area due to in-migrating African-Americans for nearly two centuries.
Small pox and measles prevail where large numbers of indigenous people reside. Most of the fevers are close to the shorelines, a product of local vectors and ships bearing the contagion in the form of mosquitoes from Jamaica, Cuba, afar. Poor nutrition due to foodways are prevalent in those regions where Goiter is noted. Geophagy (Clay-eaters) is a unique culturally-linked, or culturally-bound behavior (in Jamaica as well). Pintos Malady (today, Pinta), is an ecologically-defined variety of falciparum diseases, characterized by large dark patches and skin mottling.
Most important to note here is the need for a more extensive program devoted to a more comprehensive approach to monitoring cultural health within the US healthcare system. Medicine is not just the practice of health care using solely western philosophy and health paradigms. The basic Western European motif for defining the healthcare is not always clinically perfect for these other cultural groups.
With a rise in the size of the Hispanic population in the U.S. (see the 2020 census predictions), and a matching rise in African/African-American, Caribbean, Asian, Indigenous, Muslim, and other cultural healthcare demands, ad infinitum, the "traditional medicine" everyone is currently encouraged to practice will have to be supplemented by programs devoted to understanding the culturally-bound syndromes (geophagy, the Mexican interpretation of seizures), culturally-linked diagnoses (pinta, chiclero’s ear) and the ongoing culturally-related risks for the most common maladies (i.e. asthma, diabetes, certain heart diseases, blood dyscrasias, through genetics, foodways, etc.)
I review culturally-bound, linked and related diagnoses and disease states at a number of places (start with https://brianaltonenmph.com/gis/populations-and-managed-care/disease-patterns-linked-to-culturally-defined-health-regions/ ). My coverage focuses on how to improve a healthcare program by defining how to improve upon its cultural knowledgebase, awareness and sensitivity, and develop a more efficient, culturally targeted interventions program.
[For more on Reclus, see http://en.wikipedia.org/wiki/%C3%89lis%C3%A9e_Reclus; the book with this map is at http://books.google.com/books?id=dxj3Qr2RIWYC 😉
See on Scoop.it – Medical GIS Guide
November 18, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on The Diagnosis of James River Ringworm – an example of Historical Disease Mapping & Predictive Modeling
In 1982 I purchased a copy of Benjamin Smith Barton ’s writing Collections for an Essay towards a Materia Medica of the United States (3vols, Philadelphia, 1804). In this book he made a statement about a geographical disease referred to as James River Ringworm which first appeared in slave populations residing on lands owned by Thomas Jefferson’s family.
This led me to pose a series of research questions, which 30 years later I was finally able to answer. These questions were . . .
1) What exactly was the James Fever Ringworm?
2) Was it truly an endemic or epidemic disease like Barton suggested, or short lived?
Source: brianaltonenmph.com
The cause for James River Ringworm was important to because I decided it was either a result of the living conditions that slaves had to endure, or it was due to the transport of this disease from Africa. In a lengthy, very drawn out review of this "epidemic" for the VIrginias, I learned that it was also related to a disease that appeared along the shores of other nearby rivers according to French writer Louis Valentin, ca. 1796-1805. It also appeared to be very much wilderness related, could it have also been zoonotic in nature?
By a simple probabilities map of the region, using spatial concepts to define the different ways this disease may have evolved, I came up with several theories as to how it made its way to the region.
By reviewing basic transportation routes for the time, population densities for the slave camps, the places where it existed and their natural ecology, I was able to determine where the disease prevailed the most, and more importantly what it’s probable cause was based on physical geographic and climate-weather features.
Several times a year I am contacted about my study of this epidemic history. Currently, historical microbial pathology specialists are frequently turning to past research and writings to determine if the fungal diseases noted today as new to a region are in fact simple a rediscovery of these past regional disease patterns.
In particular, the complications of post surgical patients healing and recovery processes due to local fungal and bacterial contamination of slow healing organ transplant and ulcer injuries seem to be linked to, of all things, soil chemistry and the way soil plays such an important role in spore production and infection of open sores and wounds. Of all places, this is a primary research endeavor by a colleague of mine at a Long Island teaching hospital dedicated to high technology research in the medical sciences.
When I began this research in 1982, I had no reason to pursue it much, until the realization that there was certainly a topography and climatology reason for this purportedly regional epidemic pattern. The diagnosis I came up with for James River Ringworm was very amusing once it became clear which one of the four species most likely responsible for it was the probable cause. We missed this obvious clue to a cause for this epidemic impacting Jefferson’s slaves due to our modern interpretation of this disease. Jock Itch or Athlete’s fungus took on a very different appearance when it first appeared as an epidemic during the early years of Virginia Colony and United States medical history.
See on Scoop.it – Medical GIS Guide
November 15, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
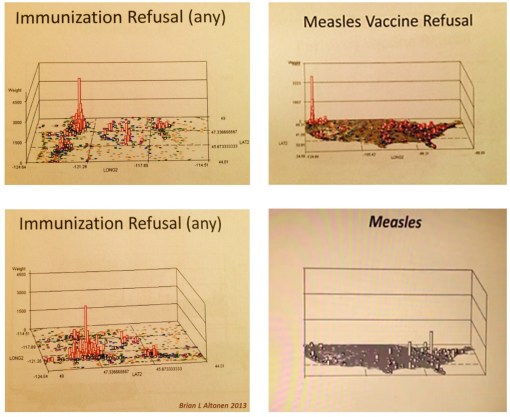
Comments Off on Why is measles making a comeback?
FROM THIS ARTICLE:
“There are two reasons for this year’s measles resurgence in the US, according to a recent paper in the New England Journal of Medicine.
The first is that the virus is still rampant in other countries, where it remains a leading cause of death in children. Globally, more than 20 million people still get measles each year, and about145,700 of those infected died in 2013 — an alarming increase from the previous year. Americans who travel can’t completely avoid contact with measles in many countries, but with high vaccination rates and effective infection control procedures in place, the disease can be kept at bay in the US.
That’s why the second reason for the resurgence is so troubling. “An increasing number of parents in this country are hesitant to have their children vaccinated,” the authors, from the Emory University School of Medicine, explain. “Such hesitancy has resulted in an accumulation of unvaccinated populations who can become infected and maintain transmission.”
There will always be a small number of unvaccinated people, namely babies who are too young for the vaccine and people whose immune systems are too compromised for a vaccine to be effective. Under the best circumstances, those people are protected by herd immunity: when the vast majority of a population is vaccinated, the virus cannot spread and will fail to reach the vulnerable few. But the “accumulation” the Emory researchers refer to is “non-medical exemptions” — parents who cite religious or philosophical objections to vaccination, artificially increasing the ranks of this vulnerable group and putting those who can’t make a choice, like infants, at unnecessary risk.
Source: forumblog.org
I think it’s going on three years that I have been posting this piece of public health news.
My review of the national population health statistics for "refusal to immunize children under 5" received a considerable amount of resistance from the medical profession. My matching posting on examples of diseases that are immunized and where they are noted as part of a patients medical history in this country, drew the criticisms of leaders in some of the grander leadership positions in the epidemiological field. But facts entered into EMRs don’t lie (some are rule outs, some are history, some are mistakes), and millions of accidental entries seems very much impossible.
This observation of avoiding the childhood immunization program I first made in 1986 when I was a researcher of taxol and several novel cancer drugs, in Portland State University’s chemistry department. At the time, I was also teaching classes on health and medical chemistry. My chemical specialty was and still is alkaloids and toxicology.
Friends in my age range in the late 1980s had kids who they refused to immunize. This was very much a by-product of the natural health movement going on around this time, but soon escalated into the vaccinations are unsafe ideology, due to the published claim that autism could be linked to certain vaccines.
(At one point in time, the mercury in the measles vaccine was claimed to be linked to autism, a claim since reversed and the supportive findings retracted by the researcher who performed this study; it was subsequently denounced in the medical journals and literature, but is still believed in by many people today).
Ten years later, when I had the opportunity to begin researching the health of the population using GIS and spatial data, this is one of the first topics I evaluated–the distribution of immunizable diseases in young children, and the EMR claims that included V-codes indicating a refusal to immunize you child.
Each of the immunizations that is refused has its own V-code. A single immunization can be in combination form, but there is an independent v-code for each line of combos or single vaccination products that is refused. A mother that refused to let her child be given an MMR for example was of course counted for each of the 3 vaccines refused. This allowed me to differentiate refusals by type of immunization, to determine if measles was the primary disease being avoided for its vaccine products.
When I first produced these maps, I was completely surprised about how universal these refusal patterns were, with parents preventing immunization of their children across all immunization products, both single and combination products, not just involving the individual measles vaccine or the MMR.
This behavior continues to day, and over the years the videos I produced of the maps of these behavioral pattern have remain unchanged in their spatial findings–the Pacific Northwest has the greatest numbers and density of children lacking the complete immunization profile by the age of 5, and the lower Hudson Valley into New York City has the greatest population density of children lacking a full immunization history.
This was also the first evidence I then publicized, for arguing that my very fast program for mapping national disease (nationalpopulationhealthgrid project – NPHG) is in need of further use and experimentation in a real life big data world. (Which I am still searching for, for my PhD dissertation project).
needless to say, there is a tremendous amount of resistance against my national population health mapping technique. I admit, it is not as standard and cut and paste as the other GIS systems everyone is heading towards. However, this is the only effective way to produce 15 to 20 thousand maps per day, or dozens to hundreds complex 3D maps, enough maps to quantify the health of the entire nature for hundreds of metrics per program run.
*************************************************
Should the reader wish to explore my unique innovation, the child immunization presentations are at the following:
http://nationalpopulationhealthgrid.com/applications/01-childhoodimmunization/
https://brianaltonenmph.com/gis/population-health-surveillance/production-examples/childhood-immunization-refusals/
Immunizations and other childcare health issues demonstrated using the NPHG program are presented at this YouTube page: https://www.youtube.com/playlist?list=PLWrApErk5byaJjbbjS6TEAAChZ7apmbzg
My Pacific Northwest Regional Health research report (1987-2006) also details this aspect of regional health, and more, at https://brianaltonenmph.com/gis/population-health-surveillance/production-examples/regions-and-health/
My criticism on much of the public health profession and managed care industry about its slow adoption of GIS in healthcare administration and management is reviewed–pointedly and in its entirety–at https://brianaltonenmph.com/about/surveillance-3d-modeling/
*********************************************
IMMUNIZABLE DISEASES VIDEO(S)
For those with just a few minutes to check out this issue, I recommend my 3.5 minute video on where the diseases are noted in the medical records, and a series of videos on the refusal for each vaccine type. These videos very succinctly makes my point – – THE HERDING EFFECT IS AN OUTDATED IDEOLOGY OR PARADIGM that has to be put away when dealing the healthcare of a modern/post-modern society. See this at
https://www.youtube.com/watch?v=W1d8fBxz5V4&feature=youtu.be
Or via (for the written text introduction page),
https://brianaltonenmph.com/gis/population-health-surveillance/production-examples/the-childhood-immunization-problem/part-i-immunizable-disease-rates/
*****************************************
My general review from years ago of immunization refusals has the following YouTube index (links to an old YoutTube site, inactive, but most videos are still running):
IMMUNIZATION REFUSALS (CHILD AND A COUPLE ADULT)
Refusal of Childhood Immunizations (all combined) — http://youtu.be/WZoaIn1ujm0
Immunizations for Diseases — http://youtu.be/W1d8fBxz5V4
Refused Variola — http://youtu.be/kAWJ35Qeu0A
Refused Measles — http://youtu.be/8Z963mMhfkU
Refused Mumps — http://youtu.be/o2E6Lj4E4_A, http://youtu.be/c61BB-WNMT4
Refused Rubella — http://youtu.be/i8hT7ubPBNM
Refused Diphtheria — http://youtu.be/AAwPKPrUgMA
Refused Tetanus — http://youtu.be/OnygXBtdkH8
Refused Pertussis — http://youtu.be/E1ZB0GMt8U0
Refused Polio — http://youtu.be/lZlEM5_AIBU
Refused Viral Hepatitis — http://youtu.be/9YS3BeY764Q
Refused Typhoid — http://youtu.be/ro-pa4Qevpc
Refused Tuberculosis — http://youtu.be/Pl77KaOW7Ag
*******************************************
Other related pages/presentations/poster sessions/etc.:
https://brianaltonenmph.com/2014/02/14/population-density-immunization-refusal-potential-outbreak/
http://altonenb.tumblr.com/post/93111801851/the-immigration-problem-were-not-talking-about
A third party information page supporting my postings: http://www.directrss.co.il/TextPage_EN.aspx?ID=6660655
ScoopIt! on the new mapping algorithm I developed–NPHG: http://www.scoop.it/t/national-population-health-grid
A NLM article on the pacific NW problem, particularly in Seattle – – http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1919709/
****************************************************
“Great spirits have always encountered violent opposition from mediocrity.”
Albert Einstein, 1940
"All truth passes through three stages. First, it is ridiculed. Second, it is violently opposed. Third, it is accepted as being self-evident."
Arthur Schopenhauer
See on Scoop.it – Medical GIS Guide
November 12, 2014
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on First Ebola, now Dengue hemorrhagic fever has arrived in the U.S.

The immigration policies of the Obama administration and the democrats in Congress have opened the door to another disease, Dengue hemorrhagic fever that is now
Source: www.examiner.com
Dengue is literally one of dozens of foreign born diseases that make their way into the United States on an irregular basis.
The fact that we hear about this now surprises me, since this has been a public health issue since the large migrations into this country from the south began. Dengue is mosquito borne. So once the winter kicks in its travel to new places will be significantly hampered.
Dengue, like most fevers, is distinguishable from other conditions brought on by mosquitoes. It has not penetrate the northern latitudes of the U.S. as much as west nile. Its common vector is Aedes aegytptii. There are other Aedes species of mosquitoes in the United States however.
Some of my first disease ecology mapping engaged in out in the field involved the studies of west nile. My documentation of Aedes in a county in NY by trapping is illustrated in one of these early ArcView GIS maps I produced back around 2002/3 . The page covering species distributions is https://brianaltonenmph.com/west-nile/vectors/
This work I did on West Nile between 1999 and 2006 was actually quite extensive. The innovation I demonstrated was the role of canopies and sunlight behavior/exposure on vector species distributions, by species and risk for a given region for west nile. These pages are frequently reviewed by students learning the disease ecology approach to surveillance. For the best of the pages, perhaps go to my work on the use of light sensor measures around trap sites: https://brianaltonenmph.com/west-nile/west-nile-surveillance-2/
Remote sensing and NLCD/Satellite imagery were two other avenues I explored for West Nile surveillance. (https://brianaltonenmph.com/west-nile/nlcd-grid-mapping-and-west-nile/ and https://brianaltonenmph.com/west-nile/6-remote-sensing/ 😉
In 2002/3, I demonstrated the value of GIS when the team I was working with used it to find the hot spot for positive testing crows (https://brianaltonenmph.com/west-nile/case-related-surveillance/ ); this was followed by the discovery of an ecological setting where west nile virus overwintered.
Back to Dengue – – – the following is a link to a 3D Videomap map of this ICD’s past behaviors: https://www.youtube.com/watch?v=eHyehbfOwFo.
Interstingly, the disease, also known as Breakbone fever, has a local NY plant known as Boneset that was a diaphoretic used to break the fever in these cases during the late 1700s/very early 1800s. The presence of Boneset (Eupatorium perforatum) and this legend on its use is a strong indicator on the local history of Dengue Fever in the upper-Mid-Atlantic states as well (A native American remedy purportedly, but with laboratory testing demonstrated in the medical school setting as early as the late 1790s). Therefore, it was not restricted to the warmest climate settings in U.S. medical history. (My 20+ years of research on this topic as well, is partially initiated at https://brianaltonenmph.com/6-history-of-medicine-and-pharmacy/trapper-and-explorer-medicine-ca-1790-1840/ — it has dozens of pages).
See on Scoop.it – Medical GIS Guide
Next Page »
