Introduction
Any mention of public health and the Hudson River often brings up the same few concerns about people’s health and the environment. The quality of water first comes to mind due to the now famous history of this water due to its more than two centuries of use in various unhealthy ways. Second, the impacts of crowded urban settings on the health of the environment in general come to mind, issues related to such things as viability and survivability in relation to the land-, water- and air-born forms of wildlife that frequent this region. Finally, there is the issue of people’s health and the impacts densely crowded settlement patterns have on population health in general. The populations of this setting have a tremendous potential for becoming the next starting point for some widespread Asiatic influenza epidemic or the place where a new foreign-born disease can enter this country.
Such has been the case in fact in recent years as well as a century ago or longer. Lyme disease made its way to this country from Sweden, infected several small community settings nearby in Connecticut, and then rapidly made its way to the more inhabitable and supporting vegetation-host-vector ecological make up required for this disease to prevail. A few years later, west nile made its way to the valley due to similar ecological features, this time by way of animal hosts probably related to a unique local land use feature just north of New York City–a zoo.
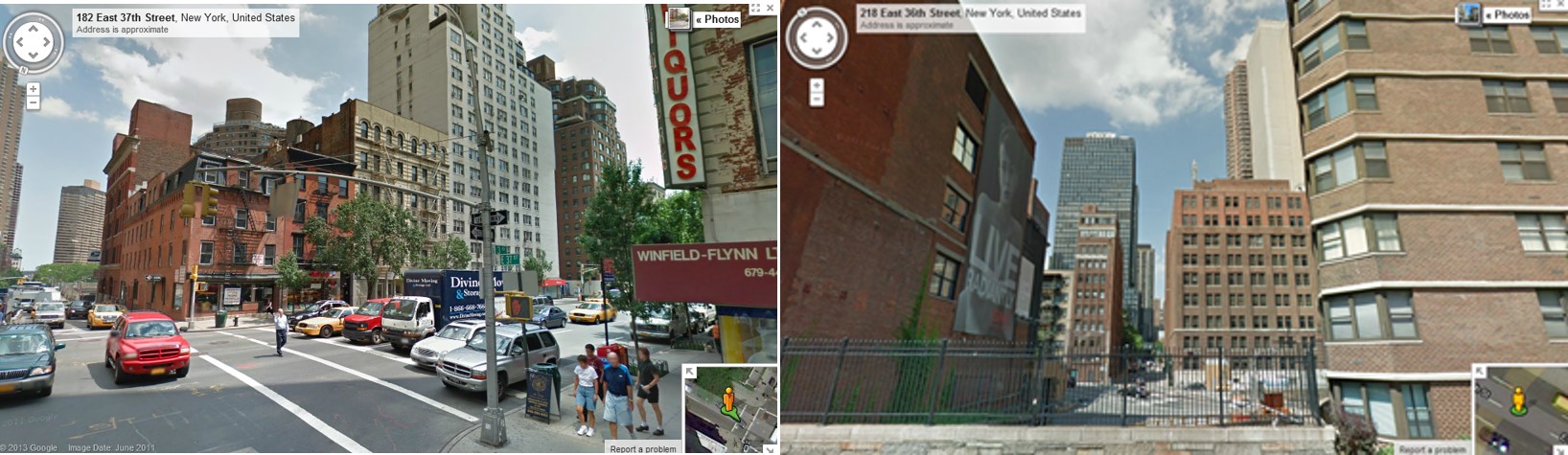
Some of the Districts monitored by Sanitation Officers.
Diseases that come into the United States do not have to rely upon natural ecology to successfully penetrate this country and make their way into its interior. Human ecology, defined primarily by population density features, make the New York City setting and Hudson Valley region very susceptible to diseases that make their way from one victim to the next via direct or indirect person-to-person contact. Other areas along the east coast are also densely packed and so serve as potential niduses for a new disease as well. The Hudson valley differs however in terms of its environmental and ecological set-up. Assuming a disease can make its way this far north of the equator, the transportation or commercial activities of the region make it likely for any new disease to find its way into the interior more rapidly than in other parts of the east coast. There are natural topographic barriers to disease for example situated up and down the east coast due to the less densely inhabited, high elevation setting known as Appalachia. But in New York, the Hudson River provides a rapidly traveled avenue between Appalachia, the Catskills, the Adirondacks, and the western part of New York and Pennsylvania along to Allegheny plateau to help diseases with natural history requirements effectively find their way into this country’s interior population settings.
A simple example of this role the Hudson River Valley plays in natural and human disease ecology is presented with this review of the public health reports published on New York City in the 186os, in particular from 1865 to 1870.
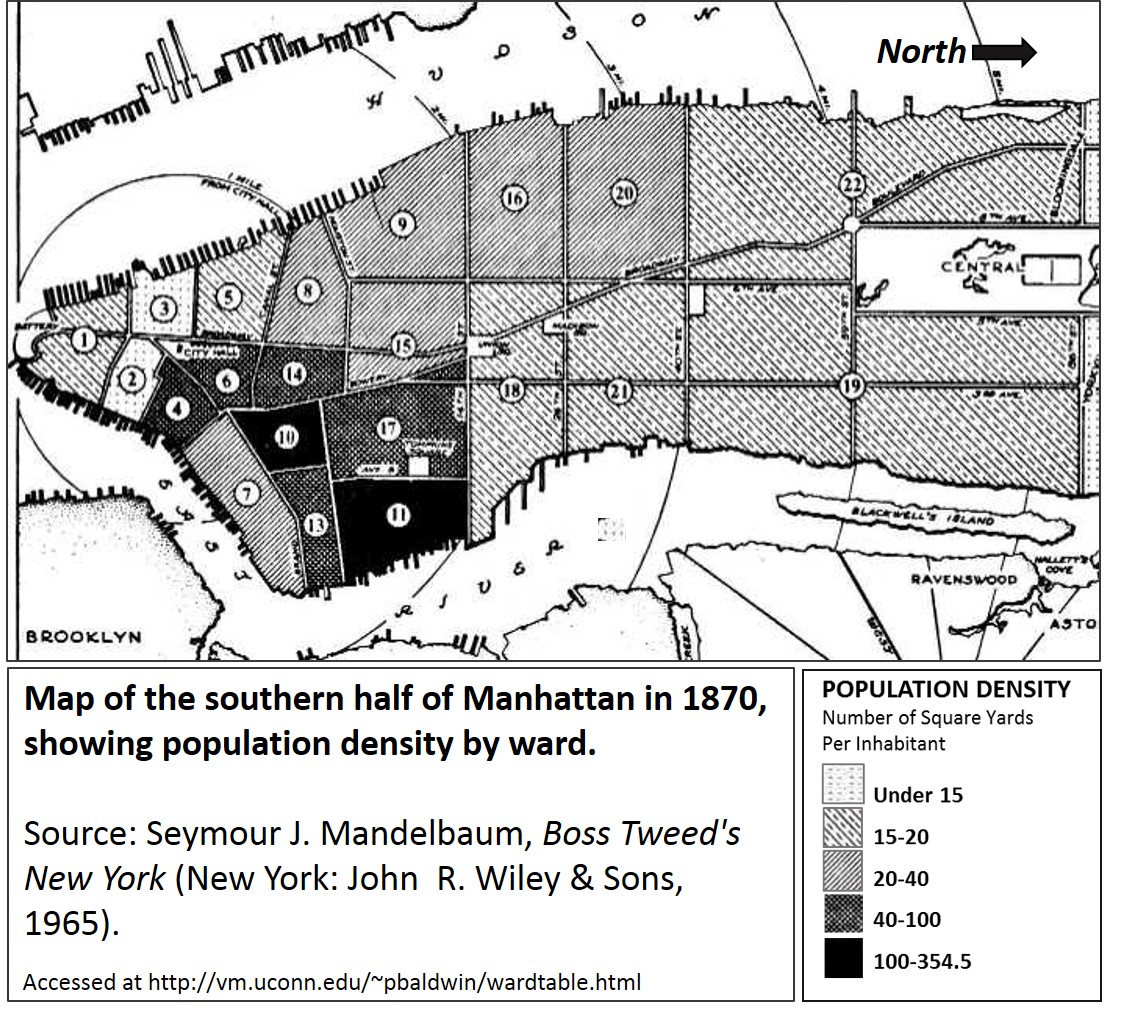
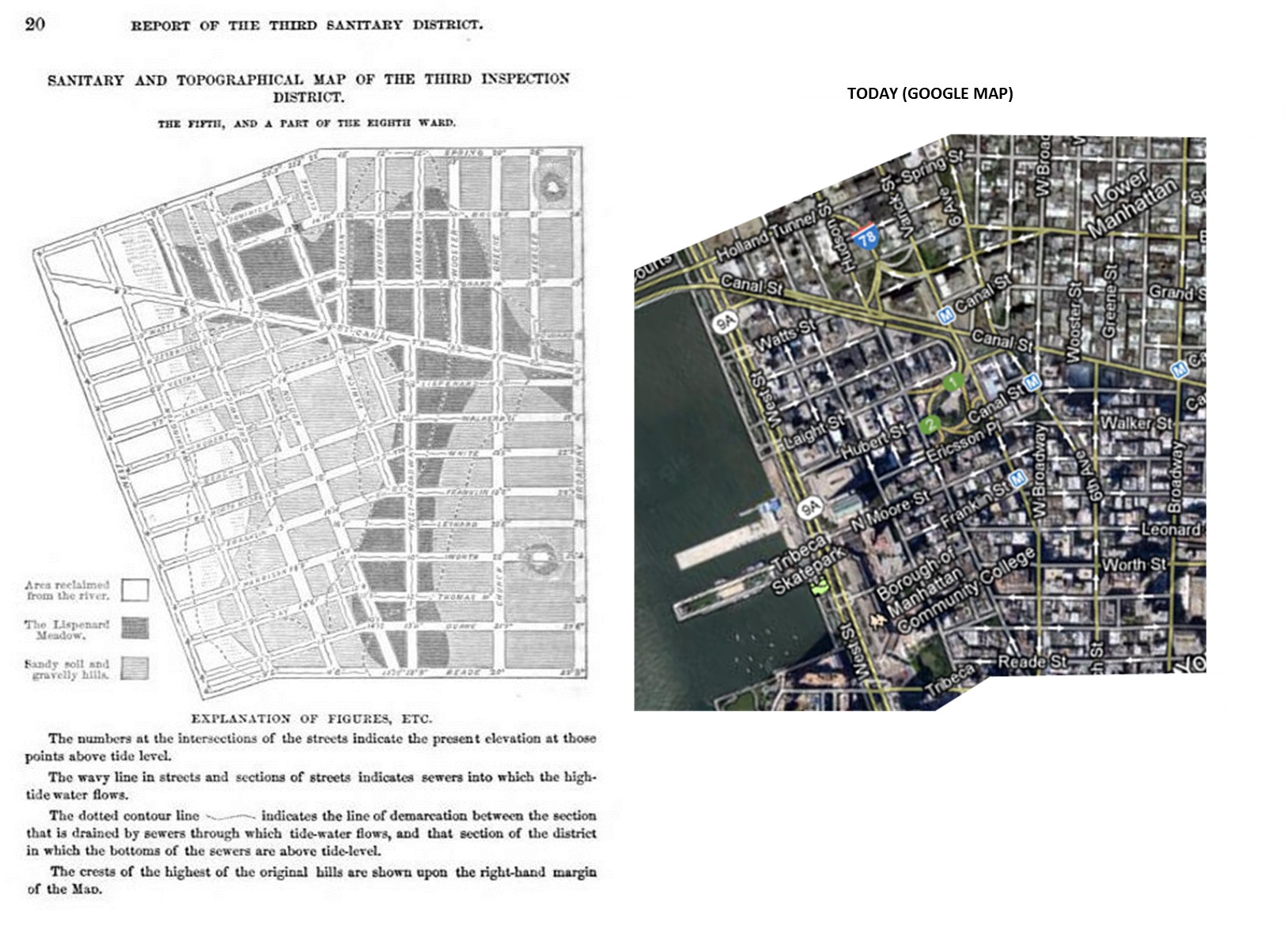
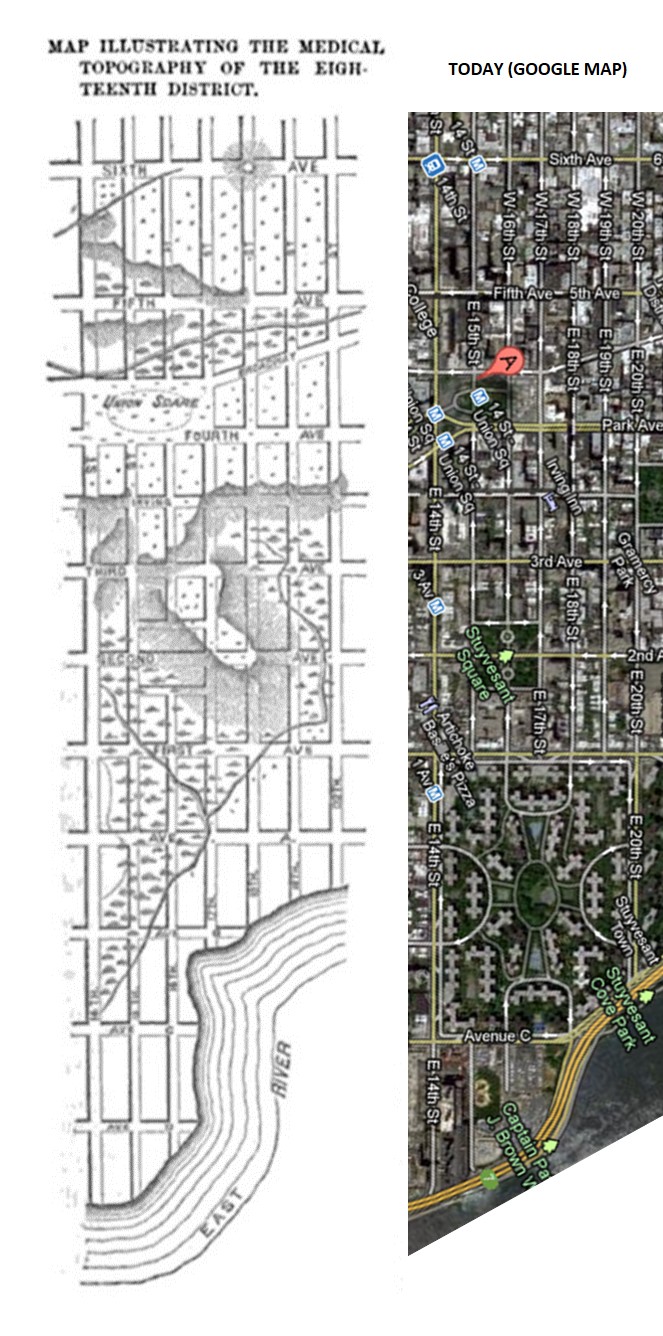
Important notes: the population density is inversely related to the “Number of Square Yards per Inhabitant” the above legend depicts! This means that light areas are actually the most heavily populated areas.
Demographics
The growth of the population on Manhattan Island began at its southern tip. The two most heavily populated areas on this map are regions 2 and 3.
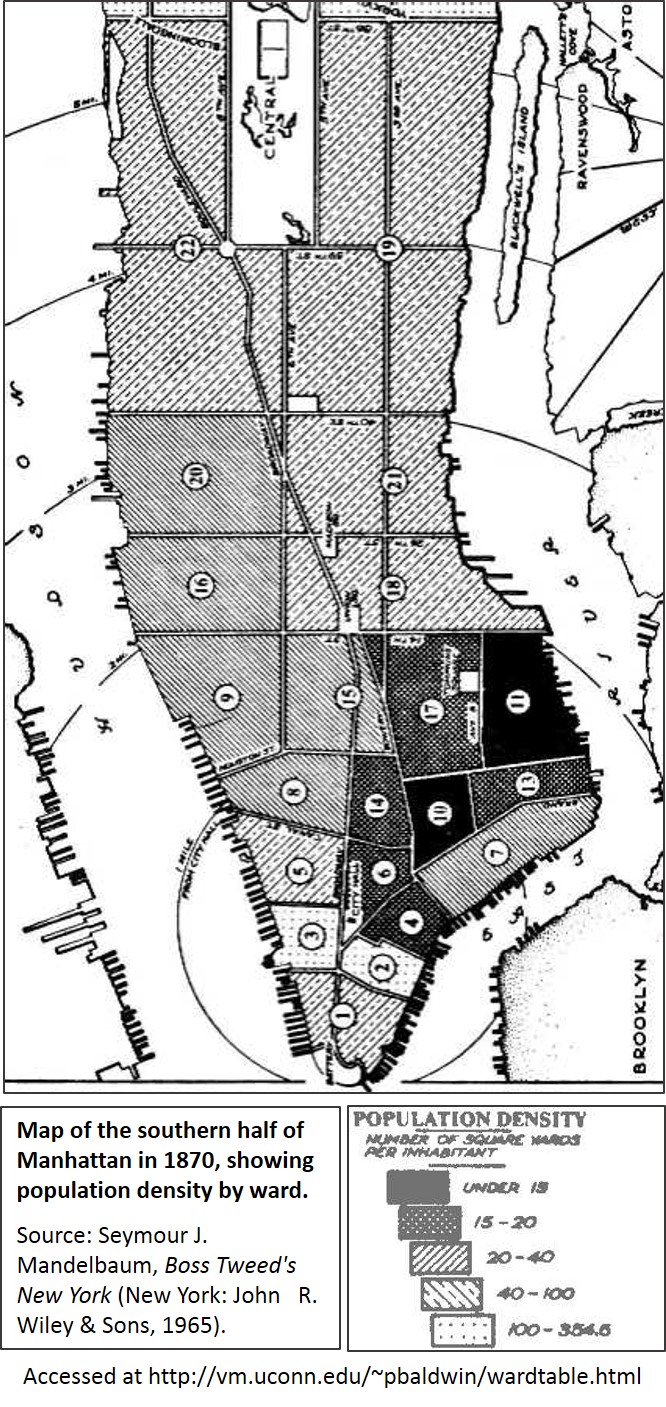
Note: the map above defines the isopleth pattern based on “Number of square yards per inhabitant.” Population density is being depicted.
.
Topography.
The topography of Manhattan worth mentioning for public health reasons and history include the following:
The island is about 13.5 miles in length and 2.5 miles wide.
It is surrounded by estuary river water, and back in the 1800s held several bodies of water within its landmass. It was also home to numerous marshlands, consisted of dozens or more trickling rivulets, creeks and brooks passing over hilly terrain. The soil consisted most of riverwash sediment surrounding some fairly sturdy rock beds comprised of a unique type of schist that is fairly dark due to black mica or biotite. This rock is known as Manhattan Schist.
During the earliest years of settlement, the belief was that the healthiness of this island depended primarily upon its swamp cover–the lesser the better. This land first became a small village surrounded by farms during the mid to late 1600s, It formed a small city at its southern end by the 1790s, but perhaps had a city-style culture forming as early and the mid-1700s. Population density didn’t become a major financial and land use concern until the 1810s or 1820s, when rapid growth in turn led to the stratification of this population of both the rich and the poor into distinct communities. Inequality was a major social problem by 1830, just in time to prepare for the import of a new form of deadly cholera in 1832, which effectively struck the city and took many lives due to the poverty and poor health suffered by members of its most ignored communities.
In the decades prior, disease seemed to relate more to place due to proximity to water. The yellow fever had this tendency to attack mostly port settings. Be they rich of poor, people residing in this region suffered the consequences of this epidemic, usually brought in by someone from afar, on board the ship, or working and spending time in close proximity to the stench-filled atmosphere of an actively thriving port. At the time it appeared as though this disease was very much a punishment for the way the city was built, and the way city-life was changing people’s lives, attitudes and behaviors to one another. But the yellow fever barely had the impact that cholera would have on the social problems with social inequality and their tendency to bring disease to a seemingly healthy setting. Yellow fever we first explained as the consequence of God’s and then Nature’s revenge upon us for how we were evolving with each other and with nature. Cholera, in particular that from the other countries considered to be of a Malignant nature, was a consequence of population size and sanitation. It demonstrated a tendency to strike certain people first, and then become capable of infecting the city as a whole. The most common solution proposed for this problem pertained to the lack of sanitation these people had. You could effectively quarantine something like yellow fever coming in by contaminated ships; you couldn’t isolate and fence in a community ridden with very unhealthy living conditions and filth-stricken people of the other social class. This was the initial problem heavily populated settings like New York City had to offer the medical field. This is what made this setting the birthplace of many public health related discoveries, concepts and attitudes.
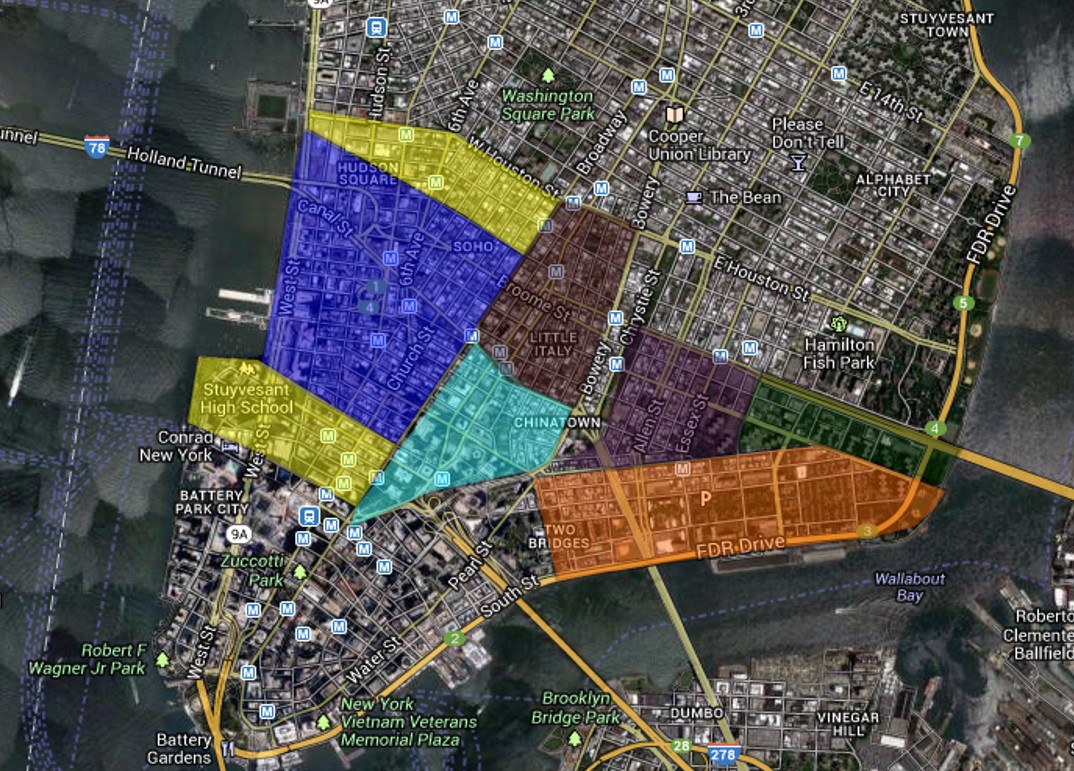
The following medical maps and figures include close-ups from above, depicting aerial landscapes. These are a very unique series of medical maps.
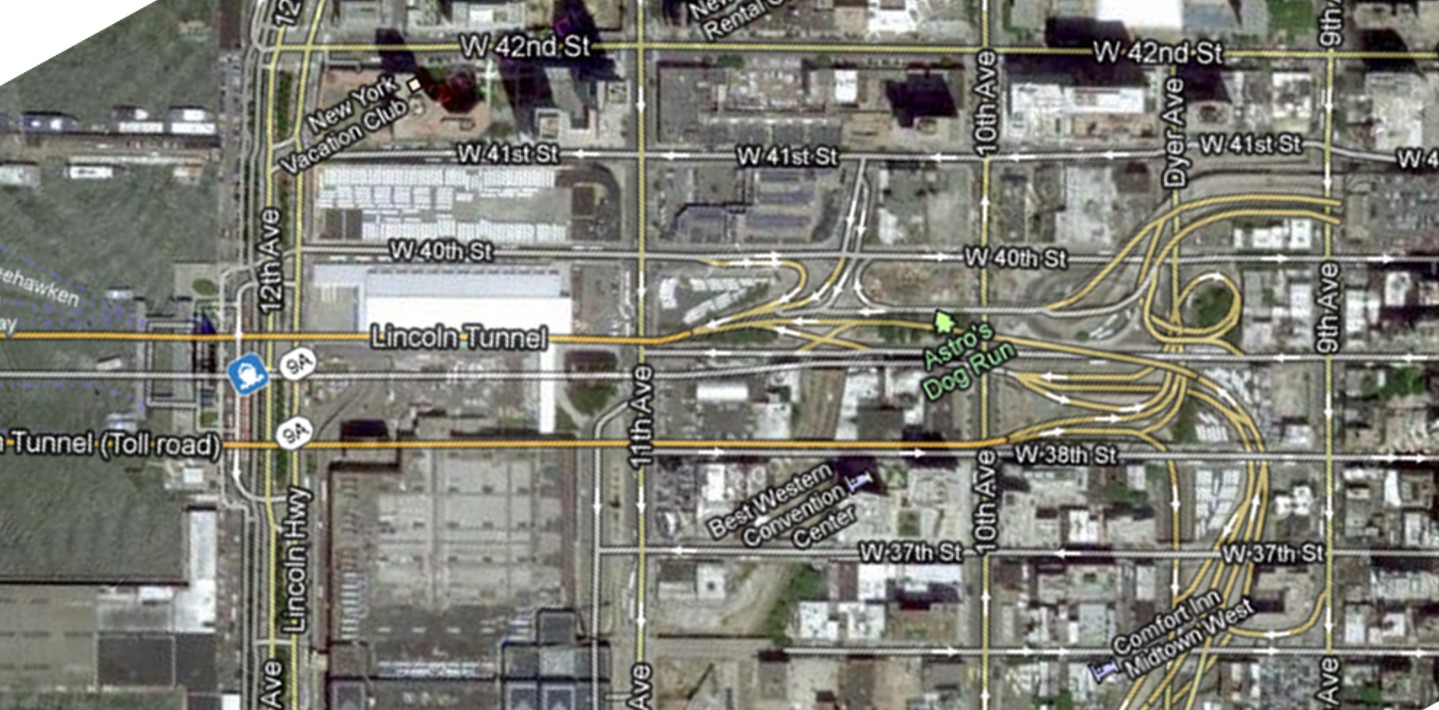
Attempts were made to link each map in the article to a modern aerial depiction of this part of Manhattan pulled from Google Map.
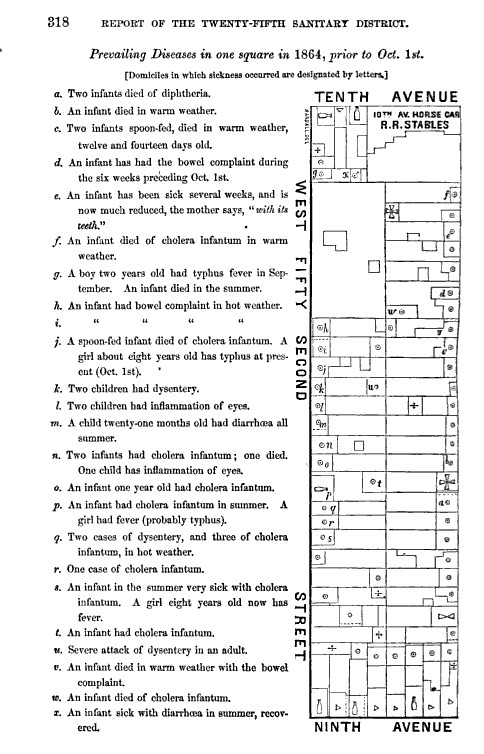
Some notes have been added on and off in this series. Notice the various causes for possible disease focused on by the different officers reporting of their specific areas. Sometimes factory buildings and the purpose of the factory are focused on because they are considered the chief cause, other times the officer is focusing on the placement of shanties and conditions of the privies. A few sanitation officers focus on the bordellos as a source for disease in their community.
The lessons we can learn about disease and population through the suffering of urbanites residing in early Manhattan are quite interesting. The following topics were the focus fmost of these reviews provided by inspection officers.
- Population size and density
- Population types or cultures
- Neighborhood community structures
- Dwelling types
- Personal waste management
- Water supply and related water use practices
- Food and Dram-ways
- Unhealthy Behaviors
- Occupation
- Workplace types and settings
- Workplace water management
- Policing and inspection
- Building use and place
- Neighboring landuse comparisons
- Recreation, Parks and Exercise
 .
.

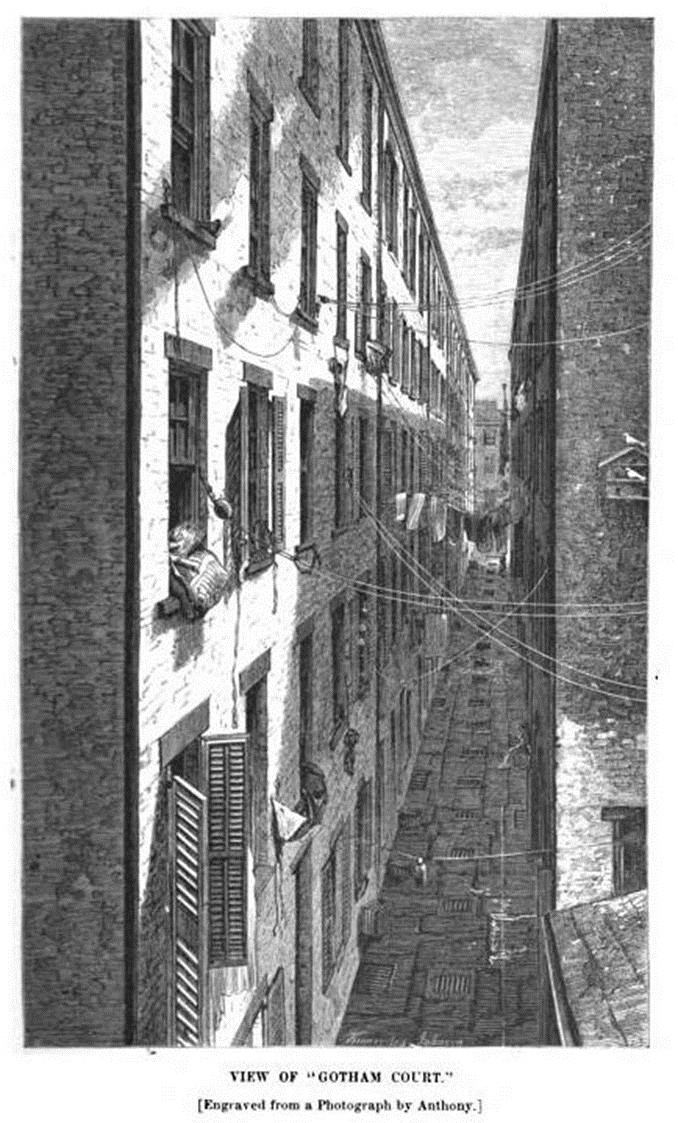
Is this the “Gotham Court” alley on the drawing above?
(A side view of looking down the alley behind 152 Ludlow St.)
.
The Maps
.
Third District


Fourth District
This area was totally leveled and replaced, and is somewhere close to Baruch Drive on the map below.

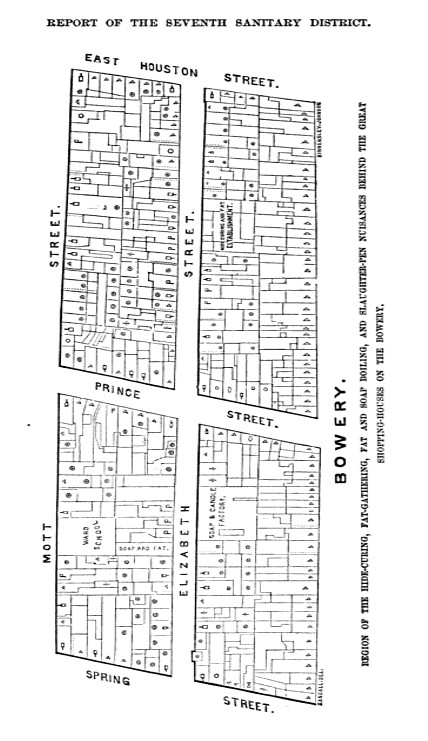
Seventh District
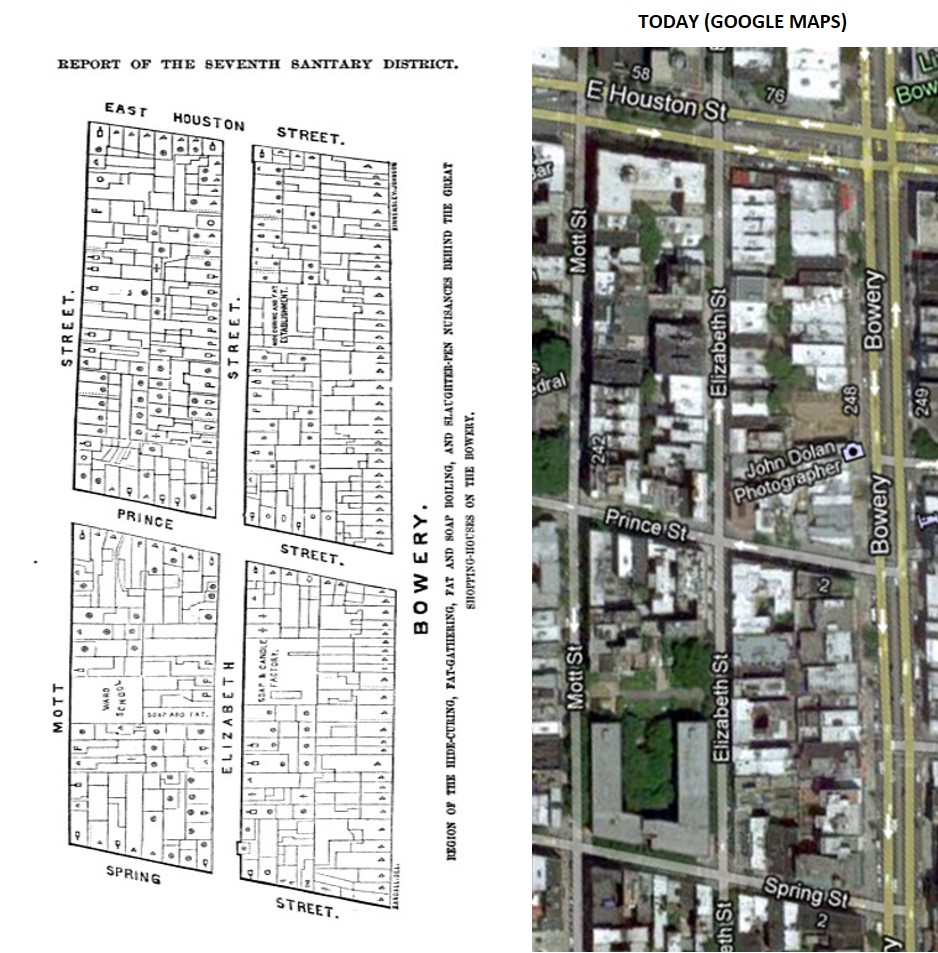
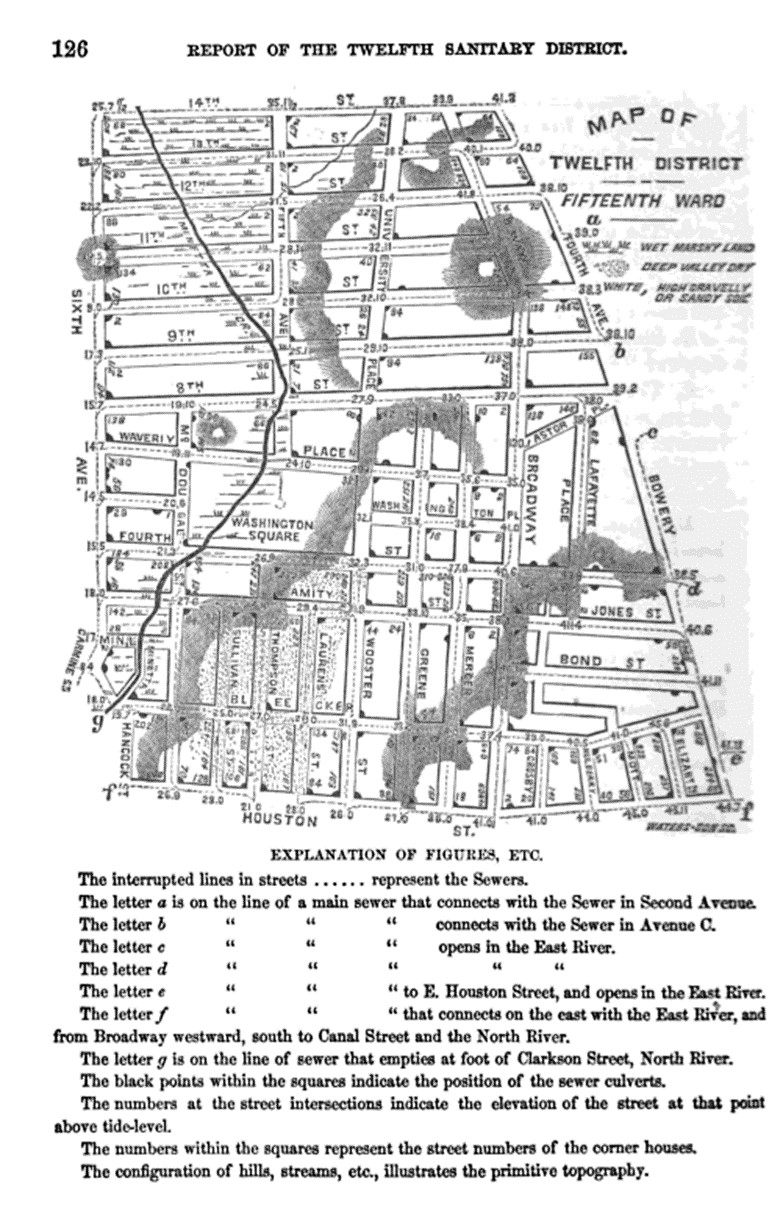
Twelfth District

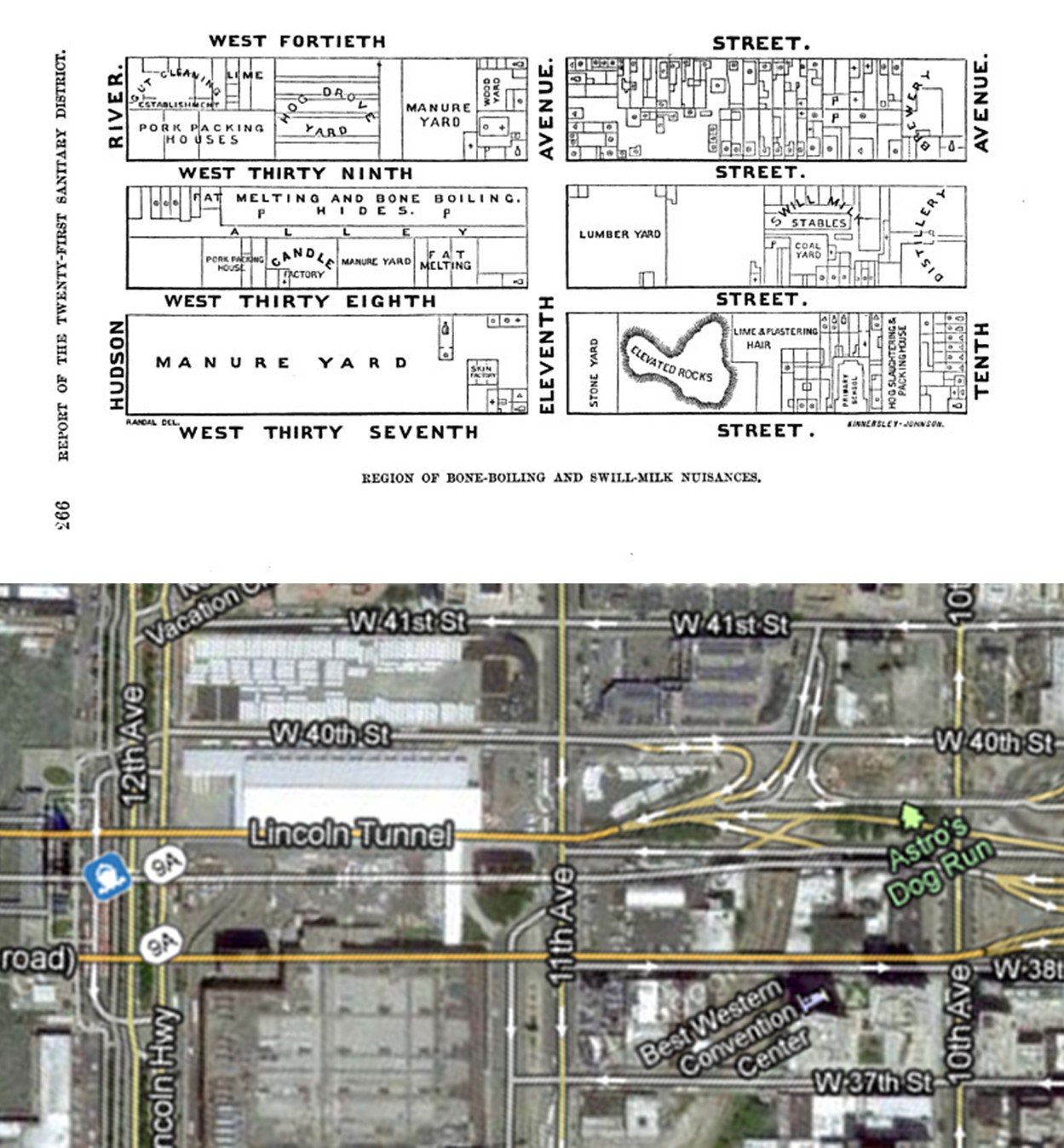
Innards or entrails from an animal in Australia — the cause for disease at many a meat, hoof and bone factory
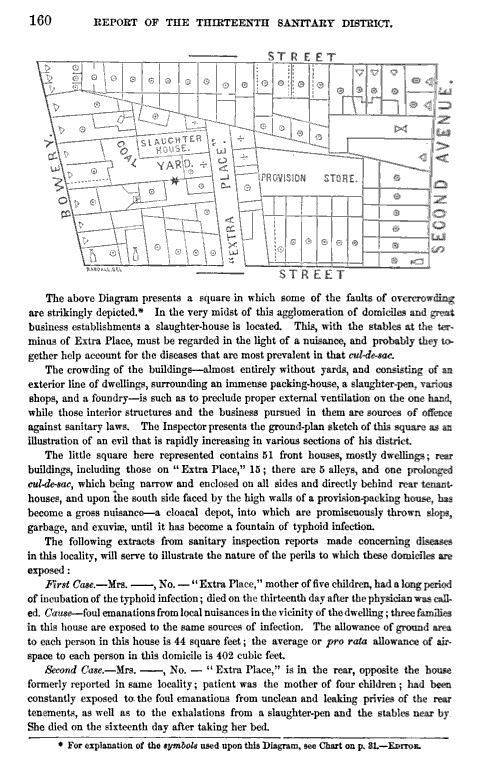
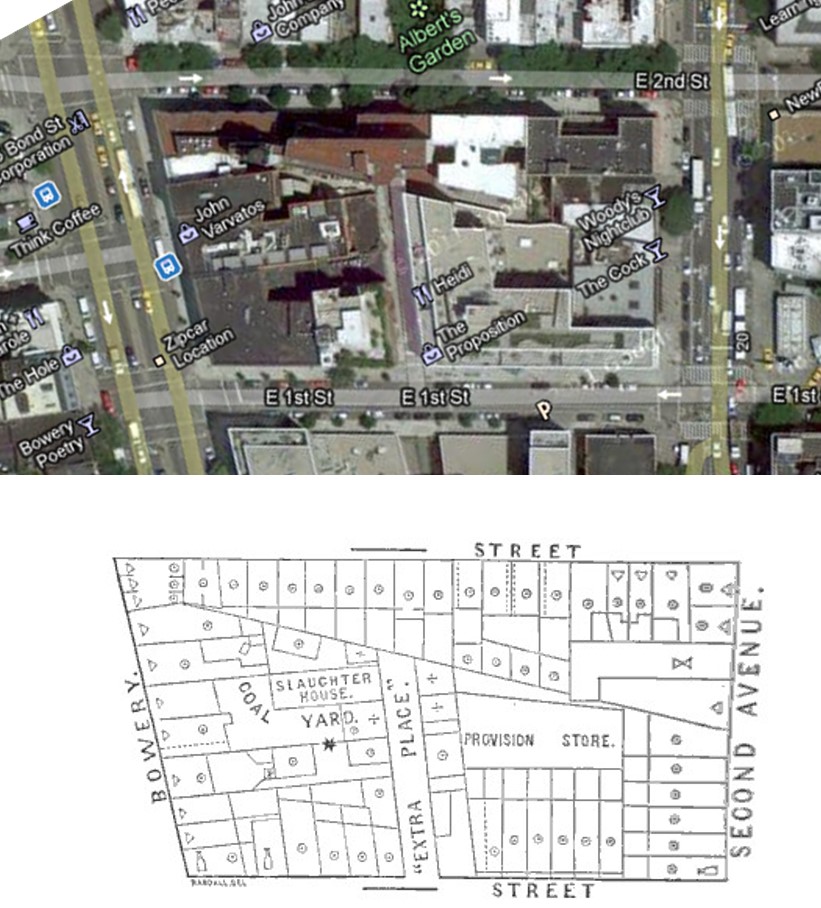
Thirteenth District
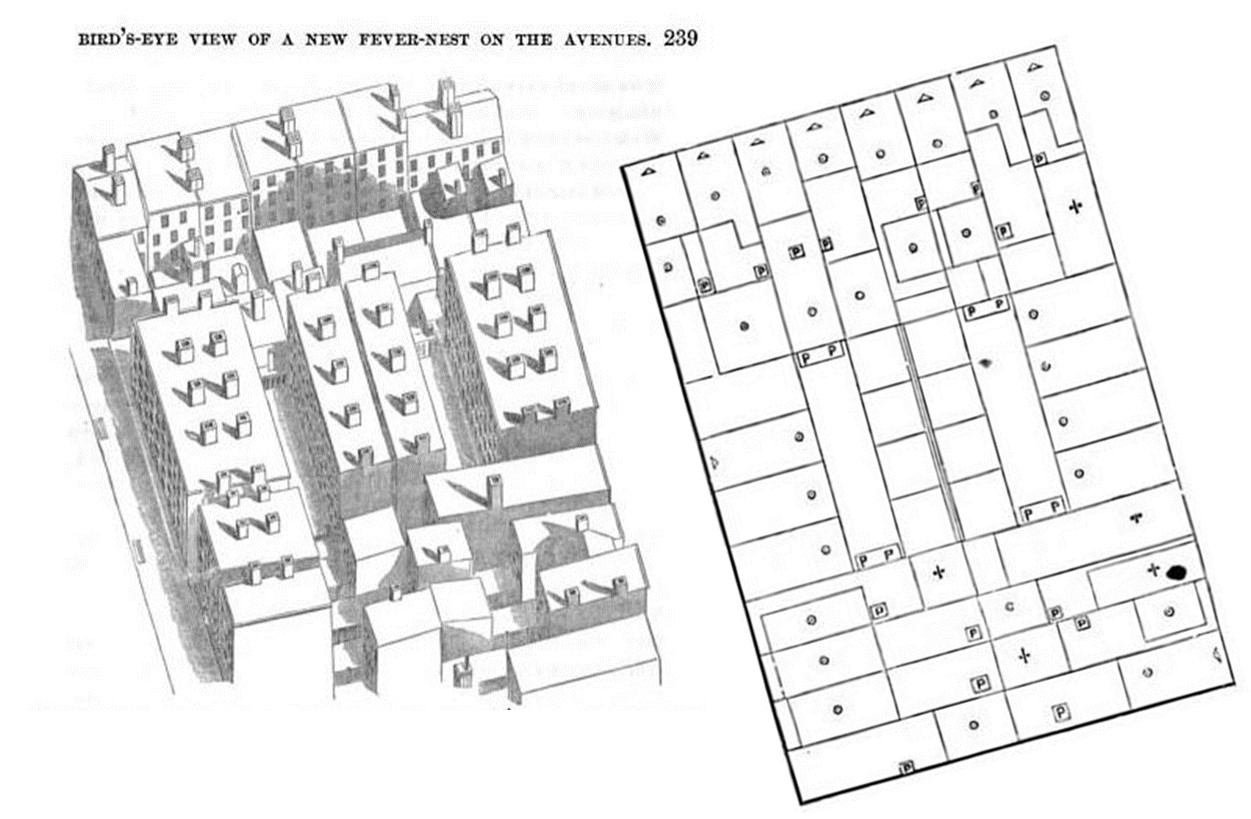
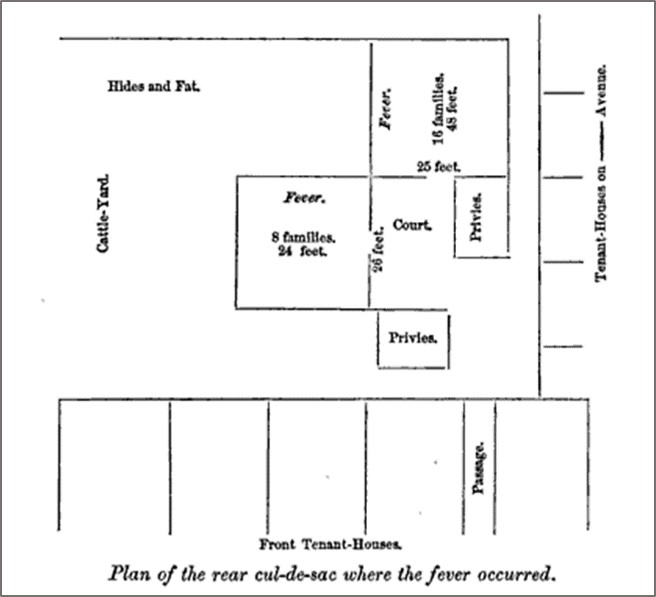
Slops, garbage and exuviae turned a section of the thirteen sanitary district into a what was called a cloacal depot, one of the filthiest, smelliest places in the city. This one was situated just east of the Bowery. A packing house for fresh cut meats added to the likelihhod of illness recurring in this region due to typhoid. Two cases were noted around the section of street called “Extra Place”. These are described in the text below. In the double row of buildings beneath the word street is a row of four rear-houses, the unhealthiest places of all aside from shanties and the actual site where the disease was generated. Notice the Provisions Store in close vicinity to this setting as well.

Eighteenth District

Twentieth District
.
[]
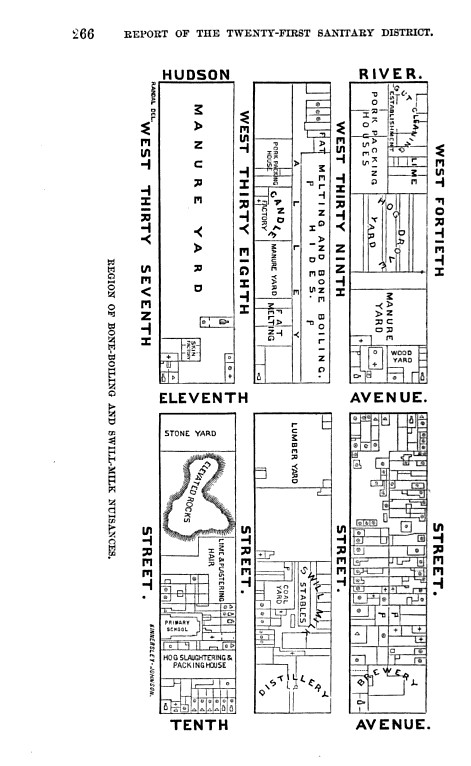
Twenty-first District
Twenty-second District
Twenty-second District

The above area was in the middle of the Kips Bay Towers section
Twenty-third District
.

.

.

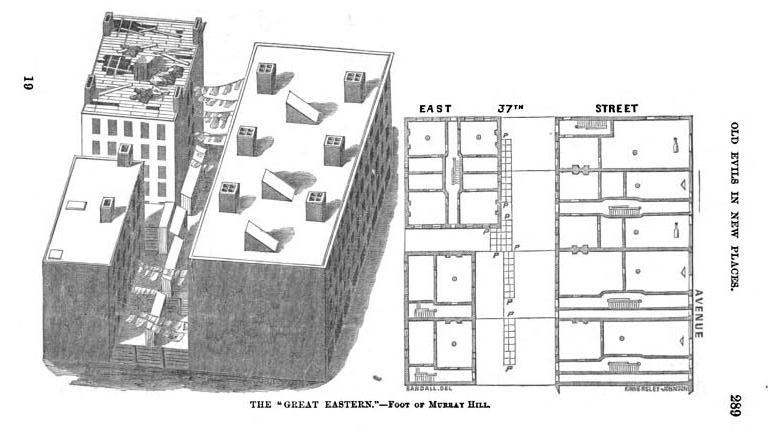
It was reported that people got ill due to the leaking, rotting roof
.
.

Is this the same building, with its roof replaced?
Twenty-fifth District
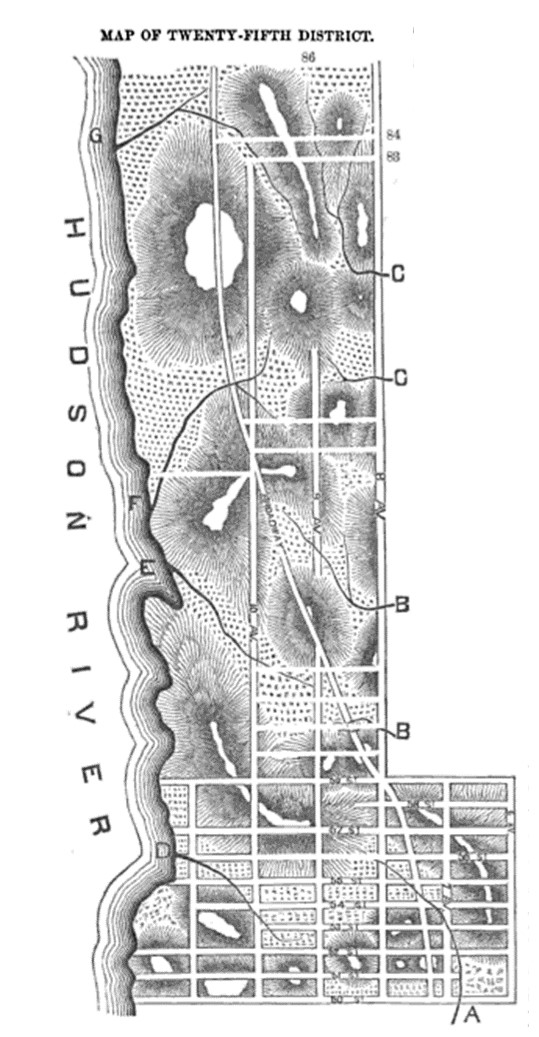
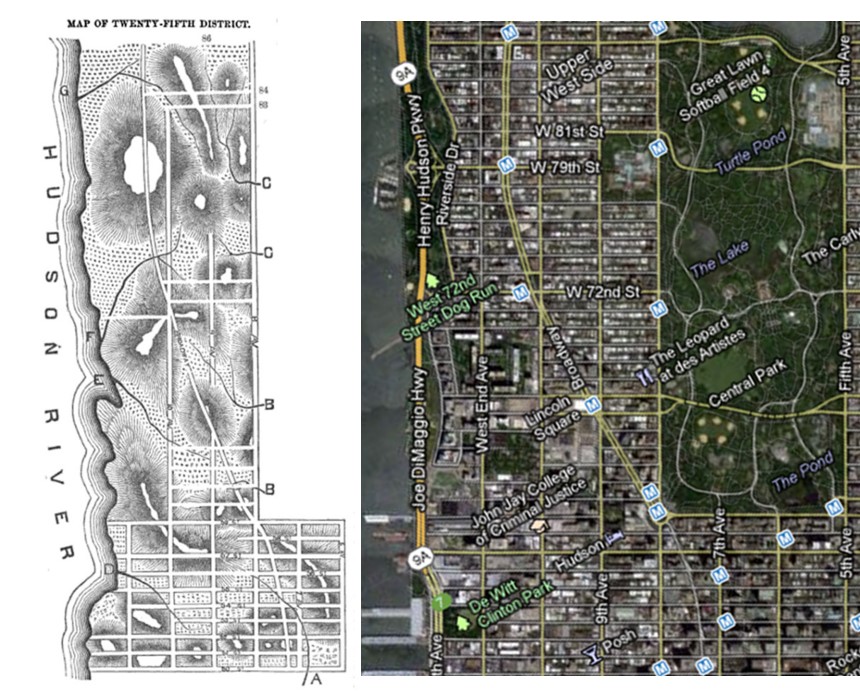
Twenty-fifth District
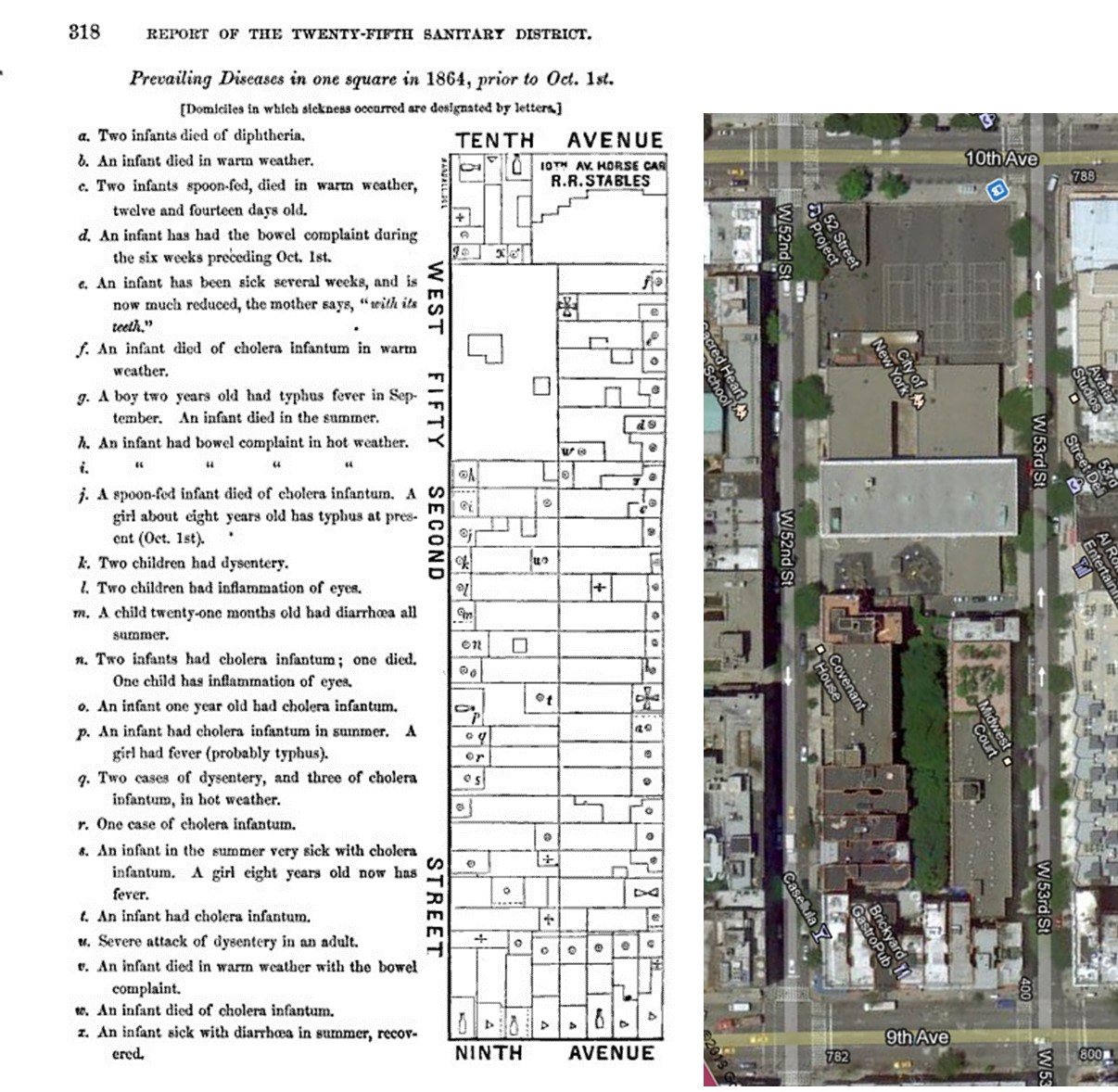
Twenty-fifth District (by Central Park today) .

Once upon a time there was a shanty in Central Park where, believe it nor not, people lived! . . .
.
Other Notes
For the above maps, a series of other findings were noted in this review. They are as follows.
Sanitation Policy. Medicine had become the science of sanitation. The description of diseases and the causes published since 1855 were focused on hygiene and cleanliness. How we live, how well we kept up our domestic setting, how our neighborhood was kept, how clean the work settings were and the waste and refuse of life was produced, kept and disposed of were the focus of the sanitary officers since 1855, when laws were put in place in response to William Farr’s work.
Sanitation laws were around in the New York vicinity since the 1780s or 1790s. The taming of hogs in New York and keeping them off the streets made of mud was one of the earliest concerns on behalf of local citizens. The odors of muddy fields laden with animal refuse and rotting vegetable matter left there for them to feed upon, the stench of swamps and port settings getting filled with the waste of local industries and materials washed ashore from the nearby estuary were enough to make it essential for some sort of control of these waste-ridden areas to be developed during the early 1800s. The lay out of streets, neighborhoods, homes, businesses, churches, dram-houses, bordellos, roads, parks, wells, cisterns and privies made for some very interesting settings where diseases could develop.
.
Communities. The most common diseases striking the city proper during this time were very much dependent upon how we lived. People were for the most part sloppy and resided in filth. Even though there were well groomed animals and neatly kept homes made of brick and stone, there were also the numerous shanties and wooden houses lining most of the streets, with the more heavily settled blocks lined with tenant houses and tightly pack main-frames with rear-houses raised in the alleys. Some of these houses were given a healthy personal water-closet setting, most had privies located on the river edge or draining into the back and side yards, some even emptying out into the soil below from set-ups located down in the basement. Privies in a multilevel tenant-home setting might only be located on two floors–the main floor or basement and the second floor, draining down a long sewage pipe and finally making its way into the sewage lines below, and on occasion gushing back up into the basement due to saturation of the soil, blockages or recent flooding.
According to some of the writings about the living conditions in New York, there was a new aroma, miasma, malarial plume, vapour, fomite, gas or excrescence about every corner, every nook and cranny in the three-dimensional local topography formed by buildings and floors. This gave rise to the concentration of three-dimensional modeling and illustration of the placed we worked and resided in. It was possible for the next cause for an epidemic to arise from the spaces between soil particles in the basement floors, or stones lying out there in the backyard where the privies were raised and wells dug, or in the spaces between the layers of wood rotting in hallway walls and rooftops covered by leaky planks of mixed oak and pine removed from a local farmers’ street up by Harlem River.
The lay out of low income communities was most atrocious during this time. The conditions of three major low income groups were often reported in these public health reviews. Germans, Irish and Negro settled areas were very often mentioned.
Occupations.
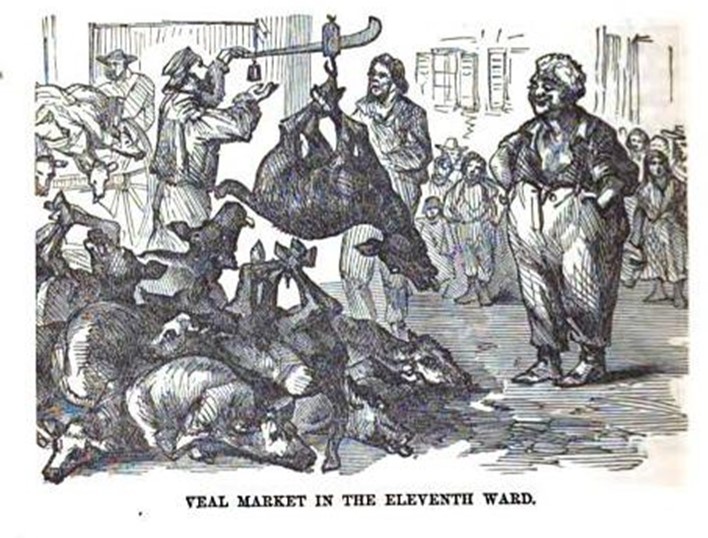
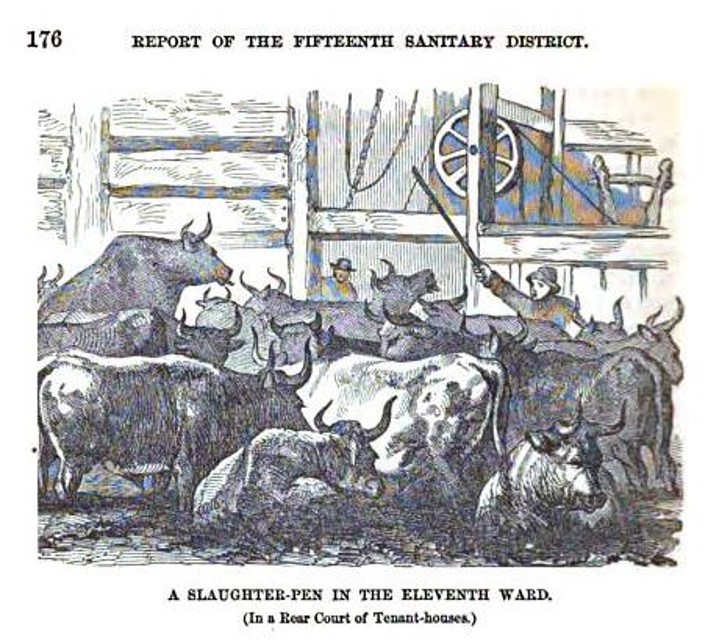
Slaughterhouses. By far the most descriptive comments made about unhealthy industries pertained to slaughterhouses.
.
.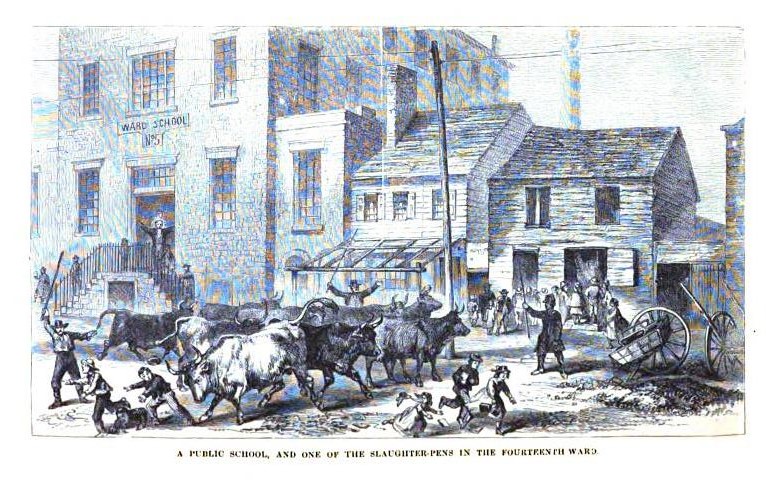
Slaughterhouse herd brought to the street in front of Ward’s School for children.
.
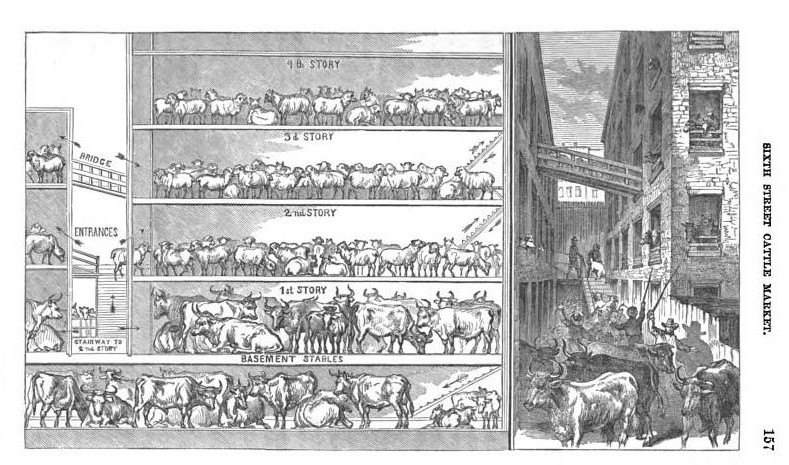
A Highly Productive Slaughter House in the City

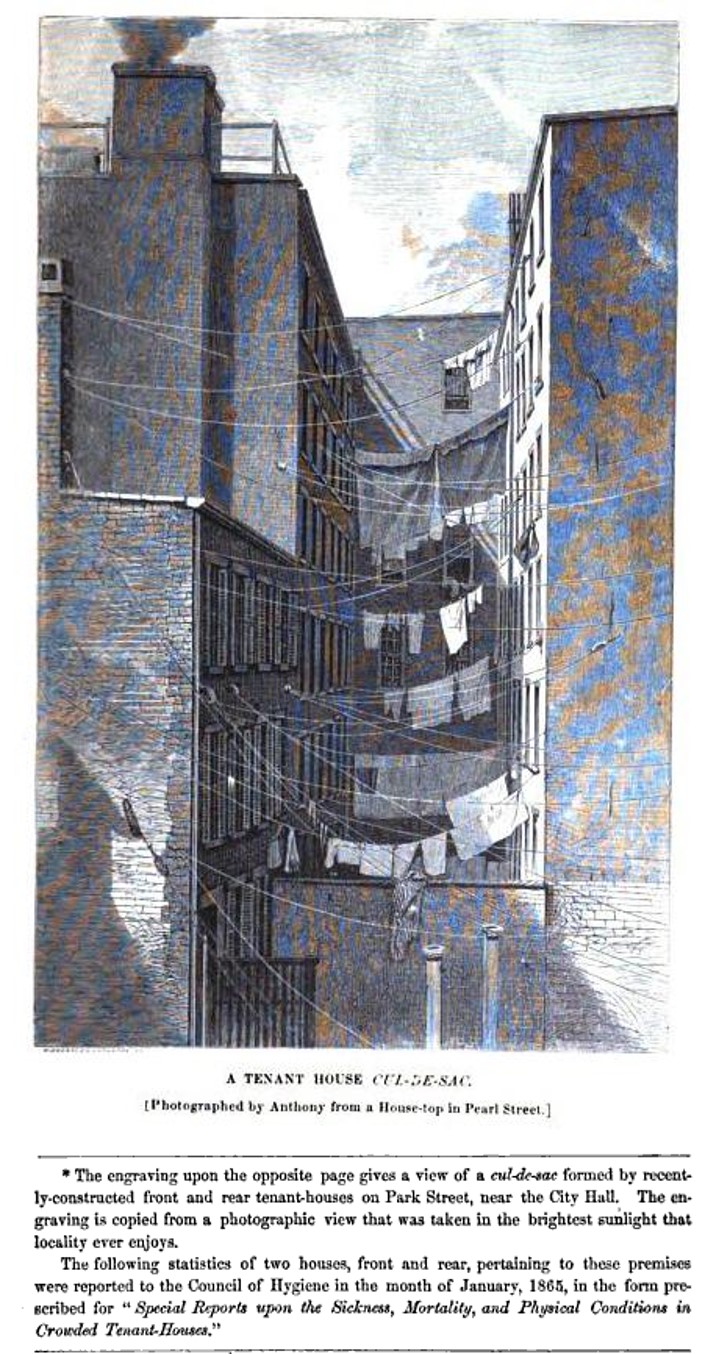
New York City Tenements, 1869
Lifestyle and Habits.
Dram-Houses.
Bordellos (to be covered on a separate page)
.
.
.

……………………………………………………………
Public Health Inspection
Public health inspection began almost immediately after the Revolutionary War was over. For decades the notion of disease quarantine officers was important to health, and this was the purpose the first police were hired in Manhattan urban setting. In the 1780s after the war was over, an example of the problem at hand was noted in Samuel Loudon’s packet published and distributed out of the city once again. At the northern end of Manhattan Island there were the healthy springs located in what today is Spanish Harlem. The owner of this property charged his visitors a small fee to have access to this water for health related purposes. Another advertisement posted at this time demonstrated the increasing problems of population density in relation to land use patterns and practices. A local farmer raising hogs allowed them to wander freely on the muddy streets, making for an obnoxious, and offensively odorous environment for his neighbors–a law had to be passed making it illegal to allow your farm animals to roam the increasingly traveled streets.
By the 1790s, industry and commerce were increasing in the port settings of Manhattan island. This would ultimately allow new diseases to be introduced to the region such as yellow fever, brought in by people infected with the disease as well as water barrels with larvae ready to hatch and thereby further spread this disease on board the vessel and within harbor village settings.
In 1792, the cause for this disease was unknown, and the theory for the time for this problem as well as many other illnesses seeming spread from one person to the next was that some form of miasma or cause for the illness was being spread from one object to the next, not necessarily one person to the next. In the records of military procedures engaged in with Alexander Hamilton acting as the General in charge of these duties, the letters (not published, but transcribed by me a number of months ago) provide important insights into how this and other diseases were being interpreted. Hamilton and other felt it could be spread by contaminated cloths and fabriccs, and so the wagons and wagoneers in charge of delivering these goods from port to quartermaster, and from quartermaster to military facility, had to be inspect to make sure they packaged the material correctly, or kept it in its original packaging, and then stowed on the wagons and transported without potential for contamination along the way. (Recall the old spreading measles or small pox to the Indians adage) .
From 1793 to 1794, the belief and fears were that this is how diseases were spread, and once the yellow fever began to diffuse into the city of Philadelphia and certain other smaller community settings, these wagoneers and their unhealthy personal behaviors and unprofessional work practices were blamed for these outbreaks. But by the end of just one season of this problem, physicians observing the cases knew enough about the facts about the conditions of the materials purportedly carrying it that such a manner of diffusion was unlikely the case.
When the second epidemic struck 1797, the rules of quarantine were developed and the theory for how yellow fever was introduced and then spread across the region changed.
That same year, the meat inspection and packing act was passed in New York, the congressman of which was Dr. Samuel Mitchell, the Chief Editor of the Medical Repository and a faculty member of the School of Medicine in New York. (There were two programs, two teaching facilities then, a New York medical college affiliated with the large hospital setting, and an actual college without this clinical setting that operated on its own and offered a degree in Medicine.)
During the next few years, Mitchell produced a number of articles with unique theories for epidemic and endemic disease patterns. He provided some new terms and definitions for the potential miasma-like agents responsible for disease, and published numerous articles from other physicians telling their own interpretations of the cause for illnesses. Mitchell himself is best known and forgotten for his septon theory–a theoretical substance produced by spoiling garbage and waste, nitrogen-based, ammonia-like in stench, etc. But poor management of latrines and poorly management slaughterhouse and meat processing businesses were also commonly blamed for disease and illness. From 1797 to 1800 about, this early version of the sanitation based cause for disease was popular, alongside weather-climate-topography related causes then being published as well.
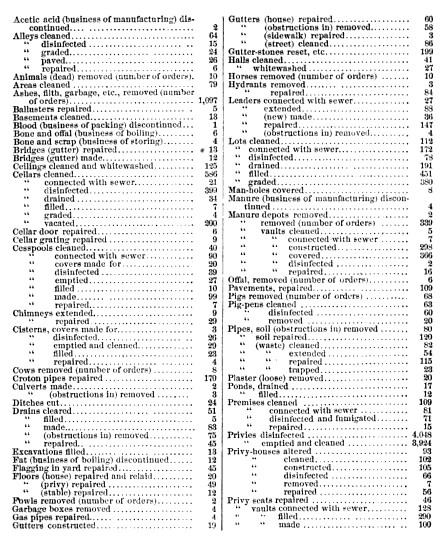
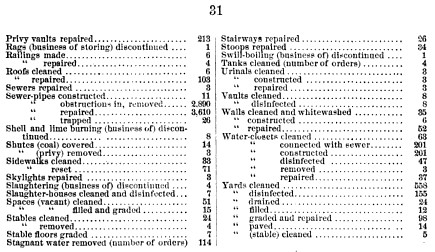
The rapid growth of the urban core of Manhattan Island led to a replacement of fields and farming lands with densely packed buildings. This had a major impact on cholera behavior when this disease came to the city in 1849. Poverty and ethnicity were linked closely to the initial deaths and all subsequent deaths that ensued over the days and weeks. The large numbers of poor Irish and German people making their way into the city made for poor living settings, many in unsanitary settings to begin with, now made even more contagious and pathogenic by unhealthy living and toiletry/personal cleaning habits. These experiences led to the establishment of standardized public health inspection programs. By the end of a decade, this program was extremely active and quite successful in the latitude and variety of health inspection activities and services engaged in. Illustrating this is the following table of activities engaged in during the 1869 calendar year.

Suspicions about possible causes for disease and the miasma or its new theoretical equivalents had obviously become quite complex by this time. Bone boiling operations, fat-rendering and gut-cleaning operations, breweries, distilleries, packing-houses, hide and tanning facilities, cattle yards, slaughterhouses all had their features considered to be unsanitary that had to be prevented. Business-generated and personal human waste were concerns. Dumps, compost operations settings, places where the dead are made to lie all had to be inspected as well for any risks of producing a new gas or effusion or source of water contamination for local drinking wells.
The development of a major reservoir connected to New York City, the Croton Reservoir, was completed by the early 1850s. There was water coming into a city-generated plumbing system. Yet the use of local wells was still very common, and the nearby placement of latrines and water closets a problem for some of these drinking water settings. During the time this report of 1870 was printed, many to most of these wells were still in use [and in the process of being mapped for one of my related projects].
[Insert map]
The following activities were engaged in by the public health inspectors during this time. For each of these a small report was generated.
- Inspection of Food
- Explosive Burning Fluids
- Cellars and Underground Rooms
- Public Urinals, to be built beginning 1867, major facility erected at 8th and 9th in Astor Place
- Public Drinking Hydrants, just approved for construction by the City Board
- Manure Dumping Locations and facilities, est. Dec. 1868
- Manure transportation plans
- Lime generated by Shell burning establishments
- Development of a life-saving apparatus for drowning victims
- Illuminating gas manufactories, est 1868.
- Tenement home inspection and survey regulation, since 1866
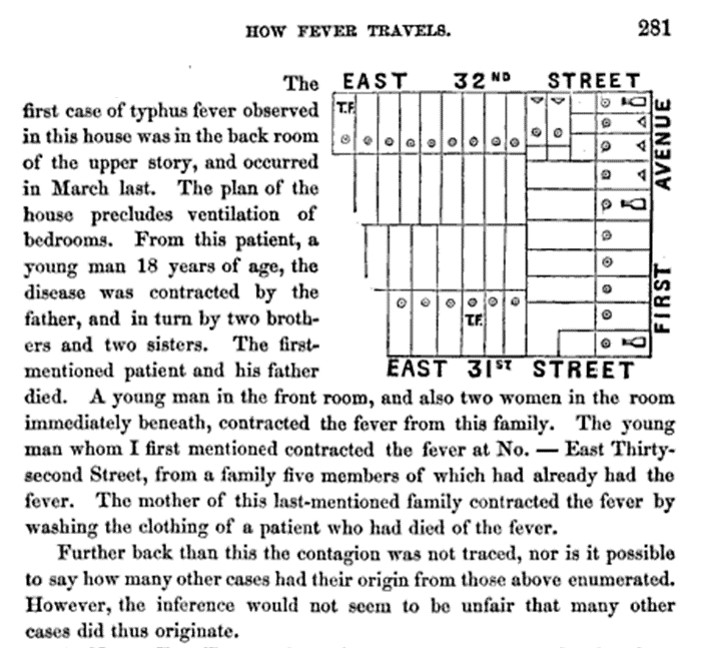
- Typhus Fever Superintendent
- Animal drive and slaughterhouse regulations
- Public building ventilation
- Nitroglycerine transportation and storage facilities
- Vacant Lots drainage (Brooklyn and Manhattan)
- Emigrant vessel permits and inspection
- Swine disease
- Street Cleaning
- Care of Rabid Dogs
- Dead Animal Removal
- Housing inspection for unfit living facilities
- Bones, scrap and refuse management
- Glanders
- Swine and Goats
- Garbage on abandoned lots
- Night Scavenger licenses and regulations
- Milk/Dairy product investigators
- Small pox vaccination program
- Straw, bedding and clothing import inspectors
- Street railroad accidents
- Dead animal rendering and utilization facilities
- Garbage/Garbage box inspectors
- Tenement house managers inspectors
- Washington and Fulton St. market officers
- Cleansing water supplies for cleaning filthy neighborhoods
- Offensive trades management (fat-melting, tallow-rendering, etc.)
- Slaughterhouse facility permits
- Summertime disinfection program for cleaning gutters, and other refuse sites with smells
- Contagious disease care facilities
- Quarantine settings.
The following is a listing of Orders and their counts, prepared by the Sanitary Superintendent:
.
.
The following is a list of findings and other important health related items noted repeatedly throughout the writings:
- Fever Hospitals
- Dens of Death
- Domiciles
- Rear-Houses
- Fomites
- Offal-dock
- Waste-pipe
- Privies
- Fever-Dens
- Idio-miasma
- Malariousness
- Vitiation
- Foetid Exhalations
- Contagion
- Cloaques
- Shanties
- Scuttles
- Pesthouses
- Fever Nests
- Sewerage
- Privy-vaults
- Swill-pails
- Garbage-Houses
- Dirt-Catchers
- Dilivium
- Paludal Miasma Flies
- Carbonic Acid
- Purulent Ophthalmia
- Slaughter-Pens
- Fat-Boilers
- Gut-Cleaners
- Swill-milk
- Tripe
- Foul Slop
- Rag-pickers
- Groggeries
- Dram-shops
- Assignation-house
- Bordellos
- Tenant-House Rot
- Insalubriousness
.
Vaccinations
The tenements houses set up the need for the development of vaccination programs
.
A Final Note
Several times in New York history we see this sudden focus on mapping, resulting in numerous maps included in the journals. This took place around 1800 when the Governor of New York asked the physicians on the state board to require doctors from the different counties report on the medical topography, climate, hydrology, geography, medicinal plants, disease natural history, etc. for their region. This emphasis on producing medical topography reports on a regular basis re-emerged in the 1804s, resulting again in numerous articles with maps depicting many of their claims or findings. This document represents one of several that came about during this time due to yet another series of bills passed requiring thorough reviews be made of developing urban centers. Being both one of the fasting growing and most certainly the largest city, New York tried to take an advanced position in this part of the sanitary movement. New York had some of its first of these types of events emerging in the 1860s, but the series presented here (the city and the page on the upstream Hudson Valley River reports), represent a considerable change in this reporting practice.
The use of aerial drawings was the consequence of such a change. These are detailed reports and depict important building features. Room size, cubic footage per person in a living space, amount of cross ventilation, air quality, water supply, privies, etc., were all taken into consideration as attempts were made to quantify the healthiness of a given building or block, in case the next epidemic or endemic disease should arise in the months to come. So these reports provide some very interesting insights into these years when zymotic theory for disease prevailed, with additions link to the more traditional beliefs in “miasma”, referring to air and other natural events considered to possibly be pathogenic.
Another report on this will focus on the regions up the River, and provided on a separate page.

June 7, 2017 at 7:27 pm
Congratulations, this post is very interesting.
August 21, 2017 at 5:09 pm
You need to also consult: https://archive.org/details/annualreportofme02newy the copy I consulted for my book <> has a much better population density map from the NYPL copy of this report at the block level (see my page 28).