March 2015
Monthly Archive
March 30, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Applications for a New Technology, overdue in the new HIT programs
The ways in which important discoveries come into medicine are sometimes unbelievable. Medicine is sometimes too slow at changing its standards and protocols once important discoveries are made.
For the past twenty years, this has been the case with GIS. The current science of spatial epidemiology is a study that has the potential to completely reform managed care and better address the rising cost concerns we are now facing. Yet, we are still not ready for these changes, or taking on GIS at full force.
Like twenty years ago, the use of GIS remains an experimental process with most managed care and insurance agencies, and is not at all required for any annual QI or Meaningful Use reviews. With the mining and use of Big Data now common to HIT, the industry is unprepared for this more rigorous, thorough, cost saving method of monitoring healthcare.
The following articles are examples of the application of GIS to managed care and quality assurance processes in healthcare.
*******************************************
READINGS
Agency for Healthcare Research and Quality (AHRQ). Using Geographic Methods to Understand Health Issues . (2014/5) Access at http://archive.ahrq.gov/research/geomap/geomap1.htm
Panth, M., & Acharya, A. S. (2015). The unprecedented role of computers in improvement and transformation of public health: An emerging priority. Indian Journal of Community Medicine, 40(1), 8. DOI: 10.4103/0970-0218.149262. Accessed at http://www.ijcm.org.in/article.asp?issn=0970-0218;year=2015;volume=40;issue=1;spage=8;epage=13;aulast=Panth
Dalton, C. M., & Thatcher, J. (2015). Inflated Granularity: Spatial ‘Big Data’and Geodemographics. Available at SSRN 2544638. Accessed at: http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2544638
Lee, D. C., Carr, B. G., Smith, T. E., Tran, V. C., Polsky, D., & Branas, C. C. (2015). The Impact of Hospital Closures and Hospital and Population Characteristics on Increasing Emergency Department Volume: A Geographic Analysis. Population health management. Accessible via http://online.liebertpub.com/doi/abs/10.1089/pop.2014.0123
Adams, A. M., Islam, R., & Ahmed, T. (2015). Who serves the urban poor? A geospatial and descriptive analysis of health services in slum settlements in Dhaka, Bangladesh. Health policy and planning, 30(suppl 1), i32-i45. doi: 10.1093/heapol/czu094. Accessible via http://heapol.oxfordjournals.org/content/30/suppl_1/i32.short
Lee R Mobley, Tzy-Mey Kuo, Jeffrey Traczynski, Victoria Udalova and HE Frech. (2014). Macro-level factors impacting geographic disparities in cancer screening. Health Economics Review 2014, 4:13 doi:10.1186/s13561-014-0013-7. Accessed at http://www.healtheconomicsreview.com/content/4/1/13
Simms, I., Gibin, M., & Petersen, J. (2014). Location, location, location: what can geographic information science (GIS) offer sexual health research?. Sexually transmitted infections, 90(6), 442-443. doi:10.1136/sextrans-2014-051695 http://sti.bmj.com/content/90/6/442.short
Angier, H., Likumahuwa, S., Finnegan, S., Vakarcs, T., Nelson, C., Bazemore, A., … & DeVoe, J. E. (2014). Using Geographic Information Systems (GIS) to Identify Communities in Need of Health Insurance Outreach: An OCHIN Practice-based Research Network (PBRN) Report. The Journal of the American Board of Family Medicine, 27(6), 804-810. dos:10.3122/jabfm.2014.06.140029. Accessed at http://www.jabfm.org/content/27/6/804.short .
Ana Lopez de Fede, Kathy Mayfield Smith, John Stewart. The Role of Geography in Health Care Spending and Monitoring Services Use. A Getis-OrdGi* Statistical Hot Spot Analysis of SC Medicaid Paid Claims per Capital by ZCTA. Policy and Research Institute on Medicaid and Medicare, Institute for Families in Society, University of South Carolina. Accessed at http://ifs.sc.edu/NewPRMM/Products/HotSpotAnalysisMethods.pdf
David Moskowitz, Bruce Guthrie, Andrew B. Bindman. (2012). The Role of Data in Health Care Disparities in Medicaid
Managed Care. Medicare & Medicaid Research Review, 2(4), E1-E15. Accessed at http://www.cms.gov/mmrr/Downloads/MMRR2012_002_04_A02.pdf
Peter W Gething, Fiifi Amoako Johnson, Faustina Frempong-Ainguah, Philomena Nyarko, Angela Baschieri, Patrick Aboagye, Jane Falkingham, Zoe Matthews and Peter M Atkinson. (2012). Geographical access to care at birth in Ghana: a barrier to safe motherhood. BMC Public Health 2012, 12:991 doi:10.1186/1471-2458-12-991 Accessed at http://www.biomedcentral.com/1471-2458/12/991
Michael Sparer (2012). Medicaid managed care:
Costs, access, and quality of care. RESEARCH SYNTHESIS REPORT NO. 23. SEPTEMBER 2012. Robert Wood Johnson Foundation. Accessed at
http://www.rwjf.org/content/dam/farm/reports/reports/2012/rwjf401106
Paul Guttry. (2012). 21 NOV 2012 RESEARCH & IDEAS
What Health Care Managers Need to Know–and How to Teach Them . Working Knowledge. Accessed at http://hbswk.hbs.edu/item/6933.html
Peter J. Cunningham. (2011). State Variation in Primary Care Physician Supply: Implications for Health Reform Medicaid Expansions. HSC Research Brief No. 19. March 2011. Accessed at http://www.hschange.com/CONTENT/1192/
Tomas J. Philipson, Darius Lakdawalla,Dana Goldman. (2010). Addressing Geographic Variation and Health Care Efficiency. Lessons for Medicare from Private Health Insurers
July 19, 2010 | American Enterprise Institute. Accessed at http://www.aei.org/publication/addressing-geographic-variation-and-health-care-efficiency/
America College of Physicians. (2010). RACIAL AND ETHNIC DISPARITIES IN HEALTH CARE, UPDATED 2010. ACP, A Position Paper. Accessed at https://www.acponline.org/advocacy/current_policy_papers/assets/racial_disparities.pdf
American Hospital Association. (2009). Geographic Variation in Health Care Spending: A Closer Look. American Hospital Association. November 2009. Accessed at file:///C:/Users/Brian/Downloads/twnov09geovariation.pdf
Sylvester J. Schieber, Chairman. Dana K. Bilyeu, Dorcas R. Hardy, Marsha Rose Katz, Barbara B. Kennelly, Mark J. Warshawsky, (2009). The Unsustainable Cost of Health Care. Social Security Advisory Board, September 2009. Accessed at http://www.ssab.gov/documents/TheUnsustainableCostofHealthCare_508.pdf
Donald M. Berwick, Thomas W. Nolan and John Whittington. (2008). The Triple Aim: Care, Health, And Cost. Health Affairs, 27, no.3 (2008):759-769. Accessed at http://content.healthaffairs.org/content/27/3/759.full.pdf+html
Dummer, T. J. B. (2008). Health geography: supporting public health policy and planning. CMAJ : Canadian Medical Association Journal, 178(9), 1177–1180. doi:10.1503/cmaj.071783 Access at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2292766/
Daniel Callahan, (2008). “Health Care Costs and Medical Technology,” in From Birth to Death and Bench to Clinic: The Hastings Center Bioethics Briefing. Book for Journalists, Policymakers, and Campaigns, ed. Mary Crowley. (Garrison, NY: The Hastings Center, 2008), 79-82. Accessed at http://www.thehastingscenter.org/Publications/BriefingBook/Detail.aspx?id=2178
John Carroll. (2007). How Doctors Are Paid Now, And Why It Has to Change. December 2007. Accessed at http://www.managedcaremag.com/archives/0712/0712.docpay.html
Sarah Hudson Scholle. (2007). Efforts to reduce racial disparities in Medicare managed care must consider the disproportionate effects of geography. The American journal of managed care (Impact Factor: 2.17). 02/2007; 13(1):51-6. Accessed indirectly via http://www.researchgate.net/publication/6575638_Efforts_to_reduce_racial_disparities_in_Medicare_managed_care_must_consider_the_disproportionate_effects_of_geography
Stefane M Kabene, Carole Orchard, John M Howard, Mark A Soriano and Raymond Leduc. (2006). The importance of human resources management in health care: a global context.
Human Resources for Health, 4:20 doi:10.1186/1478-4491-4-20. Accessed at http://www.human-resources-health.com/content/4/1/20
William H. Frist. (2005). Overcoming Disparities in U. S. Healthcare. Health Affairs, 24, no.2 (2005):445-451. doi: 10.1377/hlthaff.24.2.445 . Accessed at http://content.healthaffairs.org/content/24/2/445.full.pdf+html
Betancourt, J. R., Green, A. R., Carrillo, J. E., & Ananeh-Firempong 2nd, O. (2003). Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Public health reports, 118(4), 293. Accessed at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1497553/
Martin Sipkoff. (2003). Nine Ways to reduce Unwarranted Variation. Managed Care, November 2003. Accessed at http://www.managedcaremag.com/archives/0311/0311.variation.html
David M. Cutler, Louise Scheiner. (1999). The geography of Medicare. Accessed at http://www.federalreserve.gov/pubs/feds/1999/199918/199918pap.pdf
Mark Rosenberg. (1998). Medical or Health Geography? Populations, Peoples and Places. INTERNATIONAL JOURNAL OF POPULATION GEOGRAPHY 4, 211-226 (1998).
http://www.geo.hunter.cuny.edu/~dgreimer/TEMPALSKI/rosenberg%5B1%5D.pdf
Sarah Curtis and Ian Rees Jones. (1998). Is there a place for geography in the analysis of health inequality? Sociology of Health & Illness.. 20(5), 645-672. ISSN 0141–9889.
Access at http://onlinelibrary.wiley.com/doi/10.1111/1467-9566.00123/pdf
See on Scoop.it – Global∑os® (GlobalEOS)
March 23, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Watch 2 magicians destroy the anti-vaccine movement in 90 seconds

Measles in Disneyland should be a wake-up call for the anti-vaccine movement. Magicians Penn and Teller show us why anti-vaccination is nonsense.
Source: www.kevinmd.com
Hey. It’s magic. Better magic than prescribing to anti-vaccs.
See on Scoop.it – Global∑os® (GlobalEOS)
March 20, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on CDC’s ‘inconsistent’ lab practices threaten its credibility, report says – CNN.com
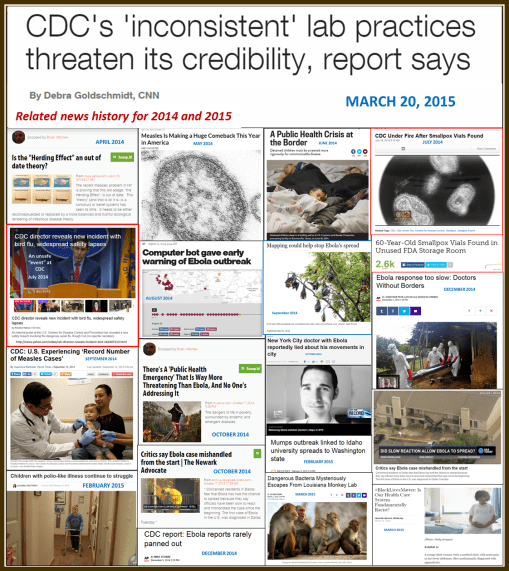
QUOTE: “A report calls CDC’s commitment to lab safety “inconsistent and insufficient.” The report also says “laboratory safety training is inadequate.””
A reminder that respect from the public is also very important. These are the events from this past year which were preventable (even if just in an ideological sense). They should be used to define the goals for the up-coming year. Notice that two quality of care related needs have been included (limited coverage by SES, and ethnicity/race).
Source: edition.cnn.com
A good reminder of how we got this way is to simply look back at the past year’s events. Since March 2014, we have had several global disease outbreaks or concerns arise in the news, about 1/5th of which really could have been managed better–the rest are status quo for surprising outbreaks and such. This 20% that weren’t well handled have "issues", we can call it, with poor management and preventive health practices. Another 10-20% also have public health related medical practice problems, that are the consequence of mistakes made at the clinical level, by provider or management and administration. But the bulk of medical emergencies do have a certain amount of unpredictably that make them hard to predict will emerge–hard to prepare for.
But once the signs of a problem are there, those 20% (or maybe 30%) of events we could have taken preparatory action for, should have been managed professionally and quickly in due time.
The problems arise when we don’t respond to an emergency in time. The fact that this in the past years has involved several kinds of emergencies, tells us the system is in really deep trouble. Now if we add to this our poor responses to natural disasters, there is much more to complain about, and god forbid, should another 9-11 event happen, odds are we will not respond any better to this disaster as we did to the prior.
October 2013 (the cases of measles that struck the Palisades Mall in Hudson Valley NY) gave us the warning we needed to be prepared for the 2014 Measles outbreak via Disneyland. My April 2014 posting noted our lack of preparedness in this matter (need I say, living in close proximity to the 2013 outbreak, I have the right to know and experience needed to realize the dilemma we are in.)
The medical field itself knew it was not ready in May 2014, before the famed 2014 outbreak, it was realized that "Measles is making a comeback." [The Disney outbreak initiated in December 2014.]
The border crisis with people coming into this country caused some hype, in June; that too became true and is the reason Disneyland could be so successfully infected.
But these are not the main concern with this posting. The main concern here boils down to one thing–poor management and leadership. Safety procedures are not abided by at CDC. Record keeping was historically poor, and so we are still finding those old 1950s vials of small pox we put away for the moment, perhaps to send later to some biosecurity/bioterrorism storage facility. Imagine what might have happen had that rubbish made it to the landfills instead of the incinerator, by a third party company hired to clean out the building for renovation or leveling.
Technology wise, the public masses are better informed that the leaders. I know that childhood diseases can spread because of what I saw in my neighborhood for twenty years in the Pacific Northwest, after talking openly with neighbors who weren’t on any health insurance (even MCD), and who refused to immunize their children. The fact that Bot users knew about Ebola before other in WHO or healthcare is a scary finding–it’s like having to rely upon your ham radios more than your TV or regular battery-run AM/FM radio during the cold war era. If I were a survivalist, I would interpret this as a sign to invest in a new multifaceted high tech shortwave communicator.
The medical world in general has been lazy about some technology. GIS is one of the best examples of this. It is heavily used by national programs, for internal reasons only. Theoretically it has epidemiological, preventive care use, but is rarely employed by experts for meeting such needs. We know this because neither the spatial diffusion prediction models nor ecological models for what Ebola was have rarely been mentioned or published with much determination. Even more, as always, this technology is used mostly as a retrospective tool; not a preventive tool. Could the flight of Ebola positive cases to Houston, to New York, where ever, been prevented? It’s easy to say no, not having developed a system to base your decisions upon. The Middle Eastern respiratory Infection and Chikunkunya could not have been predicted for their outbreaks. The latter could have been ecologically assessed more thoroughly and successfully. Makes you wonder which ones (zoonotics) are going to arrive in 2015, the some tick disease, or perhaps a south american encephalitis, or perhaps Bos Tb infecting our cattle? Like the one article states: "Mapping could help stop ____ spread", if it were engaged by the right experts.
Our concerns about polio are too few. We use the Herd Theory as the reason for this. But disease regression is happening apparently; if the herd theory continues to fall apart as a useful paradigm, we’ll need to address once more the return of poliomyelitis (but there are still several more countries that have to be penetrated first by it).
Because we have done little to deal with ethnicity differences in health, and poverty related differences, we do have even worse issues to contend with in upcoming years. Cultural emergence in the US is going to make some diagnoses and diseases become more prominent, be they of an infectious or physical/ physiological nature (culturally-link cardiac abnormalities, genetics diagnoses, etc.) , or of a cultural philosophy and behavioral cause (infibulation, culturally-bound syndromes).
These are not so much directly CDC related–CDC cannot regulate the in-migration of people who believe is some of these controversial behaviors and practices.
But CDC can oversee and regulate its own workers and their fellow workers in the health care field more efficiently–like teaching MDs not to be so self-egotistical about the improbability that they could cause the next epidemic, by allowing a patient to not be treated, or refusing to place their own self into CDC-recommended quarantine. Common sense is apparently not a physician’s (or nurse’s) primary skillset.
In the end, we must link these problems to managers and directors. Of course, the president or CEO is often who we try to blame and expel. But that individual alone is not the cause.
Rewriting the rules does not eliminate the problems. Having a committee developed to oversee past behaviors and uncover the mistakes will not suffice. Ultimately, leadership has to change for this program to get better. Then the policies need to be rewritten. Finally, the right skilled individuals need to be hired, so the agencies can catch up on their IT skills, especially the ones they cannot employ that well, for the moment.
See on Scoop.it – Episurveillance
March 16, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Confirmed: Disneyland Measles Outbreak Linked to Low Vaccination Rates
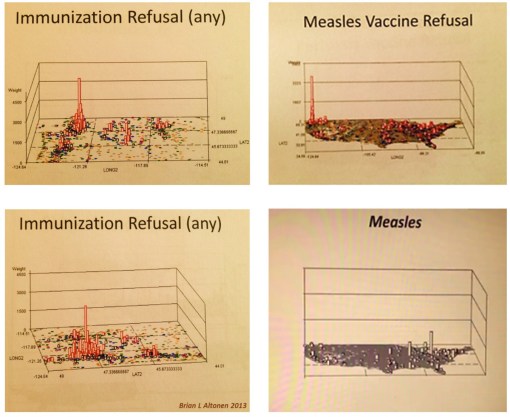
Low vaccination rates are likely responsible for the large measles outbreak that began at Disneyland in California last December, a new analysis suggests. The researchers estimated that the MMR (measles, mumps and rubella) vaccination rate among the people who were exposed to measles in that outbreak may be as low as 50 percent, and is likely no higher than 86 percent. Since the beginning of this year, 127 cases of measles in the United Stateshave been linked to the Disneyland outbreak, according to the Centers for Disease Control and Prevention (CDC). Because measles is such a highly contagious virus, vaccination rates of 96 percent to 99 percent are necessary to prevent outbreaks, Majumder said.
Source: news.yahoo.com
How much more proof did we need? (These are several year old V-code maps.) ‘Tis a shame when programs that are initiated for prevention become the last to know.
See on Scoop.it – Global∑os® (GlobalEOS)
March 15, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Traditional Chinese medicine is getting a voice at the World Health Organization
Doubts about the effectiveness of traditional Chinese medicine remain.
Source: qz.com
One of the least known facts about traditional chinese medicine in western society is that it has several times been supported by the western medical traditions for the time.
In fact, the first time we see evidence for this happening is during the 17th century, when French travelers and explorers were traveling through the orient, publishing books about their experiences in which they included the curious philosophies that Chinese doctors had, regarding pulse therapy, tongue diagnosis, moxibustion, their materia medica philosophy and their use of "accupuncture"–and how much it resembles their use of "fire", one of the four galenical elements, to define their four humours principle.
Acupuncture and its various offshoots were practiced on and off as a variation on the increasingly popular form of electropathy methods of healing. For much of the 17th and 18th century, it was the parallels that could be drawn between the ancient humoural theories, the discovery of the sympathetic nervous system, and the more recent "nervous energy" or excitement theory of the late 1700s that facilitated the addition of acupuncture into western practices by 1810-1820, in both western Europe and the U.S.
During the late 1800s, early 1900s, Chinese medicine regained its popularity, due to the relatively large numbers of practitioners engaged in this healthcare tradition. Not only were members of Asian cultures in the U.S. taking advantage of this form of health care, so too were some of the alternative healers of western allopathic medicine, ads for which appear in many US urban region newspapers.
The twentieth century has several periods when allopathy tries to first understand the philosophy underlying Chinese medicine, and then determine whether or not it fits into the western allopathic paradigms. There are a number of interesting arguments posed by allopaths trying to explain the many who experienced acupuncture at work–the parasympathetic nervous system reasoning was following by the endocrine system paradigm at the turn of the century, which in turn has been followed by allopathic arguments trying to claim "natural opiates", enkephalins, neuroendocrine system, and most recently, psychoneuroimmunological reasons as to why this philosophy keeps finding new supporters. Countering these were traditional claims regarding placebo effect, belief system related "cures", psychosomatics, and mindbody influences. (Recall the popular point therapy faith now implemented for fibromyalgia treatment.)
This recent increase in interest in Chinese medicine is focused in part on the materia medica once again. With Chinese herbal remedies, the world health belief system has transformed from its 18th century existence, relying heavily upon ginseng root and smilax root flour, to its late 20th, early 21st century period of curiosity about ginkgosides and their impacts on aging glial cells in the brain.
The most common feature to all of these periods of acceptance, withdrawal and change in traditional Chinese versus "traditional western" allopathic medicine is that a belief system is required and must be adhered to for the healing effect to take place. In many cases, physicians have little to no control over what the body and its owner decide what to do, no matter what the cause might turn out to be–believe it, or not.
See on Scoop.it – Global Health Care
March 13, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Long Term Care – How much will Chronic Disease Cases Cost the System over the next 20 years?
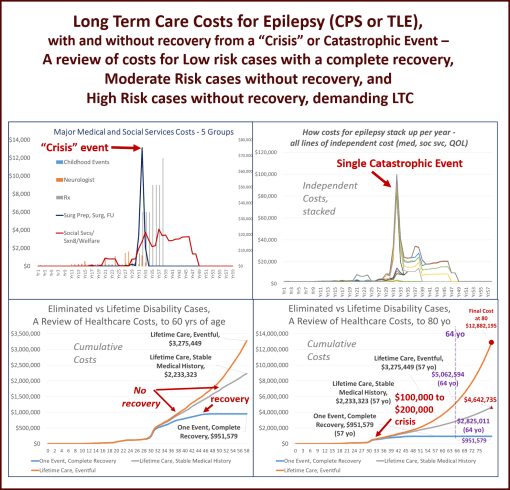
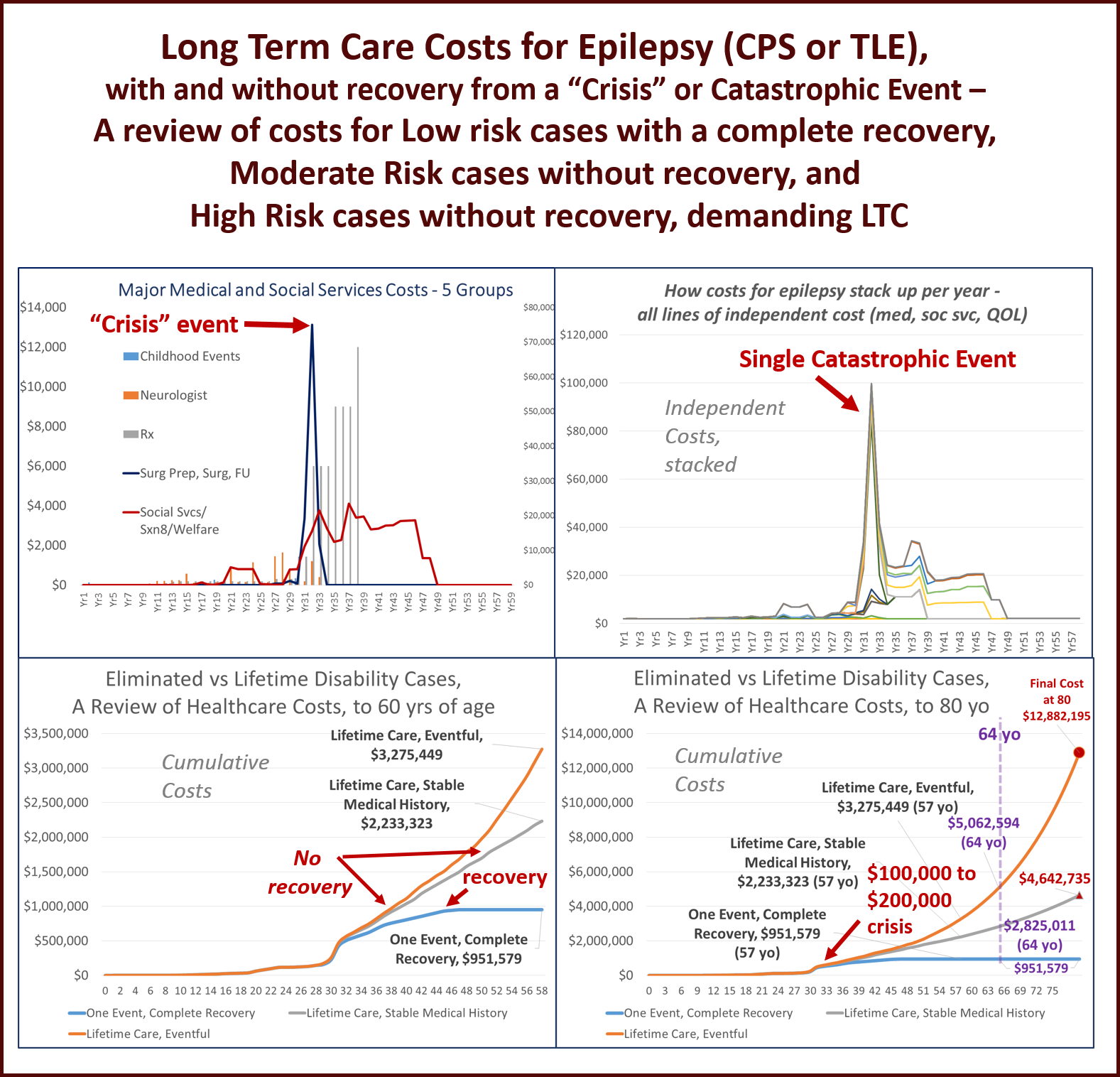
I recently completed a major portion of an ongoing research project I have been involved with over the years–the evaluation of the cost of long term care to epileptics in the past, and how we can use it to predict the cost for epilepsy care for upcoming decades.
My method of analysis was quite simple. I took the historical data for specific case(s) and then used the consumer price indexing adjustment formula for inflation to adjust all past costs to the present. I then took the real case data, which resulted in very low risk of need for future care once the “crisis” was complete soon after the age of 45, and expanded it by creating a slightly riskier pre-catastrophic event period (no high cost events) and an ongoing post-crisis/catastrophic event period, with similar activities as those of the previous years, leading up to high cost long term care accomodations.
This methodology is based in part upon methods used to perform a similar analysis back in the late 1990s. I added to this technique, more data on the costs for health care visits, screenings, labs, prescription drugs, CNS testing, emergent care events, etc., etc. than utilized in previously published studies. I also engaged in a full cost analysis of living costs, assuming the patient had no other health condition that might impact results as a covariant.
The emergent care event(s), and subsequent crisis for these cases was a neurosurgical process (left anteromesial temporal lobectomy, applied to this diagnosis for child and adults with the implied CPS or TLE ICD noted in the graphs above.)
For the baseline case, the surgical process is assumed to be 100% effective, performed at the midlife of the patient’s life. This lowest risk case is also assumed to recover completely from the crisis and return to education and/or work without further complications (essentially representing a “cure”).
The moderate risk case continues to experience post-surgical seizure events, although less at first, but over time requires new testing, new medications, further tests and screening, changes in therapies, etc.
The high risk case is assumed to have ongoing debilitating conditions develop even after the surgery is completed, as the seizures recur and reduce quality of life over the next 20 years.
The costs for each of these cases up until the age of 57/58 yo were then reviewed (again. starting with real time/life costs for care data for the baseline case). The other two were then evaluated.
Based on changes in cost over time, and their linear versus polynomial form, a prediction modeling equation could defined for each of the moderate and high risk cases (formulas were different), to determine how much ongoing medical care for this health status would cost the system ,first by the age of 65 (retirement year, if any were still employed), and finally, by the age of 80.
The results of this study demonstrated that the long term cost for lifetime care for a patient with epilepsy, who reaches the age of 80, but requires special housing in the later years due to long term complications, could easily reach 10 MILLION DOLLARS (much of this due to long term care demands).
(All additional costs were not CPI adjusted for future inflation, but the prediction model equation takes much of the trend with inflation into account).
The moderate risk cases (presumably the majority of cases in this age range), cost the taxpayer-funded healthcare system (preretirement years=Medicaid; post-retirement=Medicare) a little less than five million dollars.
What makes this analysis different is the inclusion of costs for social services related services and intervention events, for all stages in the a patient’s life, from childhood years through college and early employment years, into hospitalization and post-hospitalization/post-surgical years (counseling, neurosurgical counseling, neurosurgical testing, WAIS, and post-surgical occupational and cognitive speech therapy reviews were included.)
Each of these two types of patients was also assumed to receive continued MCD/MCR assistance for the rest of his/her life, including Section 8 and Food Stamps coverage, to name a few of the additional costs not fully evaluated in the older forms of this study performed back in the late 1990s.
No early mortality was assumed for these cases. Since people with active, ongoing epilepsy are normally assumed to demonstrate a reduced lifespan of about 10-20 years, this could be considered the one flaw in this analysis. With such a reduction in longevity, a significant number of these two high cost groups would die off well before the age of 70.
Nevertheless, this provides a reason for engaging in more aggressive, early interventions into epilepsy care. The recovered individual cost the system nearly a half-million dollars in real money, a little less than one-million dollars once these costs are CPI adjusted. And such an outcome (“the cure”) is an infrequent event.
In sum, the moderate case can cost anywhere from 4 to 5 times more than the recovered epileptic.
The highest risk cases can cost the system as much as 12-fold, according to this analyses. Even if we cut this amount in half, we are still talking about an additional 6 million dollars in cost of care over time.
These amounts per patient by the way represent costs per year that are higher than what most individuals earn in these same age groups, were they employed.
Each case therefore represents a reduction in taxpayer income for the country, with each dollar traded over for each dollar required of the medicaid or medicare systems. This amount doubles for high risk patients.
More importantly, the cost for caring for a typical high risk patient between 70 and 80 years of age will cost the system about a quarter million dollars per year.
The total cost for the care of retired people with epilepsy in upcoming years has been estimated to be in the billions, with about one million people who are now eligible for this health care assistance, should they still be around about 20 to 25 years from now.
For more on this study, go to https://altonenb.wordpress.com/
See on Scoop.it – Global∑os® (GlobalEOS)
March 11, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Michigan disease outbreaks spark backlash
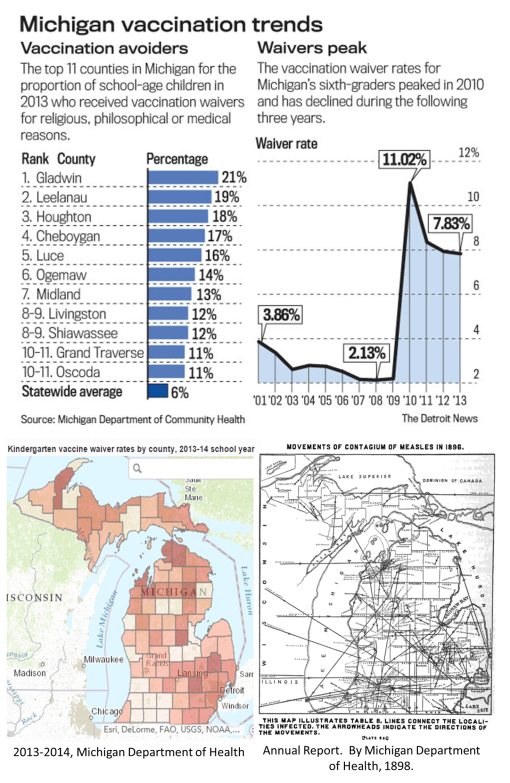
Measles in Michigan–Today and 120 years ago. Anti-vaccination trend irks parents, especially in Traverse City where outbreaks occur. Statistics on current antivaccine trends in Michigan (top figure and lower left). Geography of the 1896 outbreak that struck Michigan (lower right), from the State of Michigan Department of Health Annual Report.
Source: www.detroitnews.com
A series of interesting spatial epidemiology questions can be generated from this news.
The first is ‘is this a continuation of the Disneyland’ outbreak or a new outbreak with different roots?’
The second, ‘could certain parts of the diffusion process in Michigan mimic their beahvioral patterns during the outbreak in 1896?’ We have the map to follow up on this question with.
Thirdly, ‘can we relate the Michigan introduction and diffusion process to human behaviors in the adjacent country of Canada?
See on Scoop.it – Medical GIS Guide
March 8, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Protected: More of the Truth – When Ageism and Sexism Hit Home
March 3, 2015
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on The First Decades of Homoeopathy, Part 2
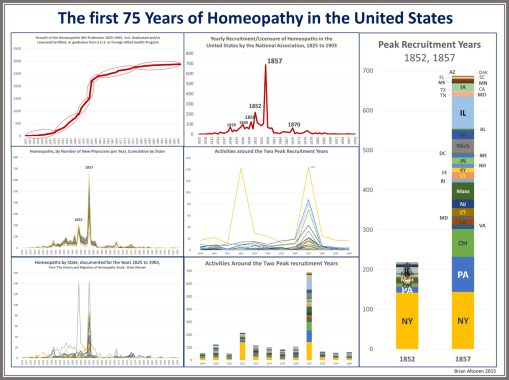
These data, obtained from a review of the profession by principal leaders in the early 20th century, demonstrate the phases of development homeopathy endured, as it was introduced (1825-1836), developed a substantial small following (1837-1845), went through an early growth period (1846-1852), then took off at an incredible rate (1853-1857/8) [Plot 1]. This process is very much in agreement with the plots generated for studies of innovation. If we consider the growth in popularity that ensued during the 20th century, we come up with something that closely resembles the Gartner plot (not displayed), referred to colloquially as "hype cycles".
The peak years in annual growth in numbers of people becoming certified in this profession shows to major peaks at 1852 and 1857.
The research question for this moment is "why are there these obvious peaks in acceptance?"
Since 1993, I have been teaching that cholera was the reason Americans began questioning the value of allopathy. The failure of allopaths to explain, treat, or eliminate cholera from our nation’s history made many question their controversial practices, in particular the administration of mineral remedies and the continued use of the lancet. Homeopathy was one of three major alternatives to allopathy during this time. The homeopaths had successfully taken the teachings of the great epidemiology mathematicians in England, an duplicated their studies on various institutions, hospitals, clinical facilities, prisons and asylums, and when mortality rates for patients were compared between homeopathy and allopathy treated patients, every study demonstrate allopathy mortality rates were at least twice those of the homeopaths (more on this to be posted).
To this day, the methodology, validity and outcomes for these results remain undeniable and are the crux of why allopathy was about to fail.
The return of cholera in 1854/5/6 renewed people’s faith in the non-allopathic professions. In addition, the recent history of the public health failure that ensued in the military hospitals at the Crimean War solidified such claims for the borderline doubters still out there truing to decide (this is cited as a major reason in the homeopathy journals themselves).
For whatever reason, there was an explosion in recruitment of individuals interested in learning and practicing homeopathy, about a quarter of whom were regular allopathic MDs. The allopathic medical profession was now financially, politically, and at the government level, floundering.
In the U.S. , the advancements made by the military due to the Civil War help suppress these previous failures in the profession. The role of the lancet was reduced, although not eliminated, as homeopaths continued to publish their supporting statistics on lower mortality rates linked to homeopathic treatment.
The bar charts in this presentation demonstrate the large numbers of stated that engaged in the enrollment of new homeopaths.
The homeopathy profession also become a popular culture craze a short while later. Even with a lesser number of MDs interested, due to a number of steps the AMA took to disenroll or delicense MDs practicing this profession, the public was still interested and the homeopathic schools and hospitals developed by then flourishing in spite of the legal and gubernatorial promotion of allopathy.
Beginning around 1882/3, State Medical Licensure boards were required to have an Eclectic, Allopathic and Homeopathic MD on board, to monitor and maintain their specialty’s credibility.
For the next 50 years, what few officially trained homeopaths there were, continued to practice according to their faith. Fortunately for the allopathic profession, the role of statistics in demonstrating success with regard to patient mortality rates became a less popular way to engage in this medical political argument.
The ending of many major epidemic patterns helped solidify the support for allopathy. Quarantine, not better practice or reduced death rates, was one major reason allopathy re-emerged around the turn of the century. The other major reason allopathy began to prevail around 1900 was the development of a strong anti-fraud and "anti-quackery" program, with political and publishing power, more than support generated by way of clinical success.
The strengthening of the bacterial theory for disease, accompanied by the refusal of homeopaths to accept the bacterial theory, were the reasons homeopathy ultimately lost much of its support by the public during the 1920s and 1930s. Both World Wars continued to strengthen the basis of the bacterial theory, a concept the Civil War helped to initiate due to the sanitary/microbial theory it gave rise to.
Homeopaths tried to counter this reduction in popularity during WW II by entering the war as a specially train medical group. For the next 50 years, it was mostly the popular culture version of homeopathy and the naturopathic profession that kept this profession alive.
See on Scoop.it – Episurveillance