
PART V
The Pacific Northwest
In the course of my review of regional health patterns in the US as these may be predicted or defined by demographics and population health statistics, I found that there were several major features of the large regions of this country defined above.
- Several regions had larger families, with at least one parent and children receiving care; typically an employed spouse/parent is providing the health insurance coverage, but in the case of Medicaid families, where two parent families are less frequent, such is less often the case.
- One region has an exceptionally high number of people over the age of 65, so much that this particular population feature makes it a standalone.
- The Pacific Northwest had population features that were not that far from extraordinary. However, once ICD related evaluations were added to this evaluation process, such was certainly not the case.
Medical Care and Treatment Decisions
It has already been demonstrated that immunization is the chief indicator of possible cultural differences with the Pacific Northwest versus other parts of the country.
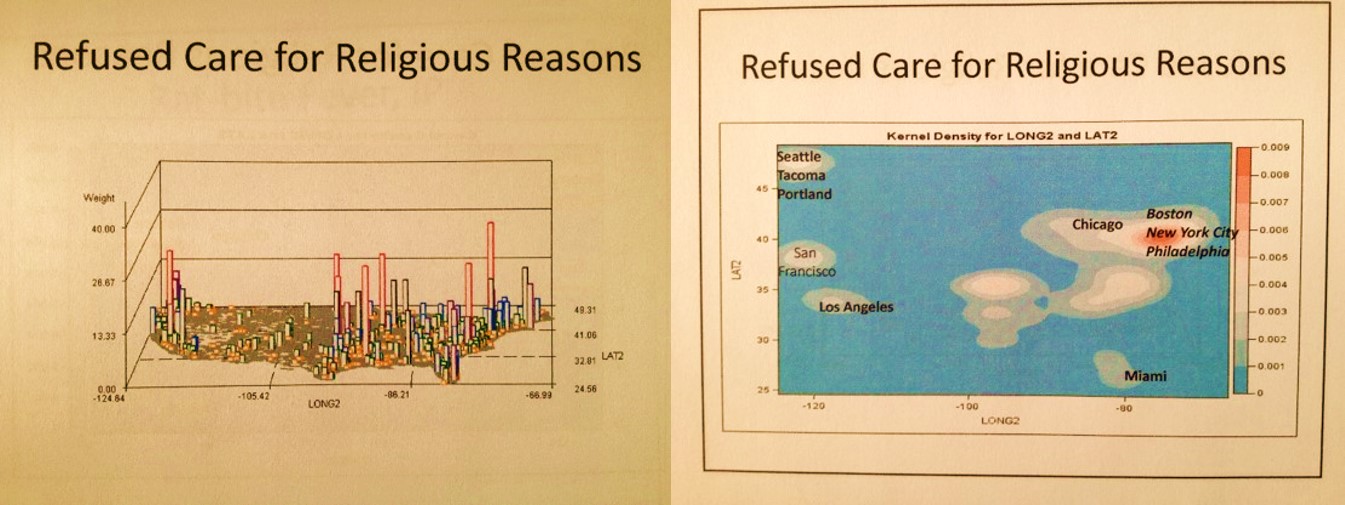
Another socially sensitive indicator of popular culture based health attitudes are the issues underlying religious based reasons for refusal of care. This behavior is not as well pronounced in the Pacific Northwest, and there are not many parts of this country bering peaks in the amounts of refusal of care practiced for a given area.
Ρ
.
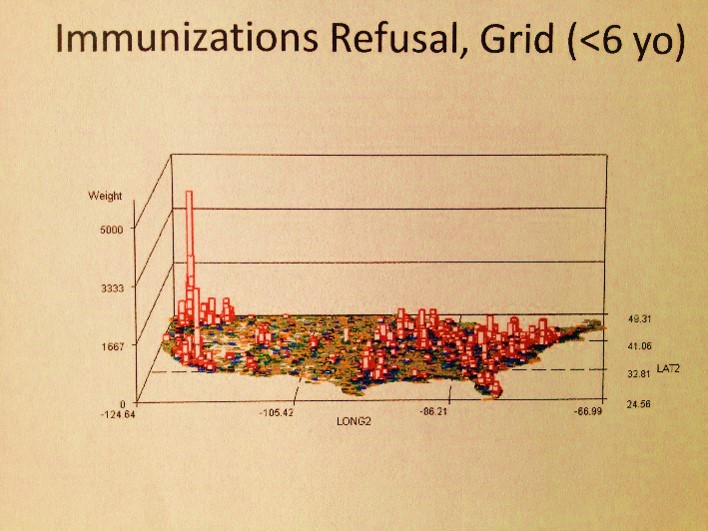
In contrast, Childhood Immunization demonstrates the single most important example of the uniqueness of character of the Pacific Northwest. This uniqueness is due to many of the same features that exist elsewhere in this country–culture, economic history, living a life characterized by social inequality and poverty. refusal to engage a child in the immunization is perhaps one of the most common of these sociocultural behaviors found to be prevalent throughout the Pacific Northwest.
At first we might assign this particular form of refusal of care to a simple line of reasoning–parents are concerned about the impacts these immunizations have on their children in terms of behavior, growth and academic performance. During my course of studies in Portland, I had numerous friends with these opinions about the impact of the measles vaccine for children–all were against its use due to its mercury content. Most used the argument that mercury can cause autism or ADHD, but some people were more against the immunization process in general, and as is typically of this part of the country, very much in support of alternative methods for obtaining health care and maintaining good health.
For this reason, I assumed measles immunizations would be the major program then impacted by this public concern. However, once I began my work as a population health analyst for the Medicaid/Medicare populations, I discovered that it was not just the completions of the measles vaccines that was being limited by this public perception. Digging further into this topic, it became clear that all immunizations in general were impacted by this popular belief. There were several reasons for this shared activity.
Some individuals confessed that if one vaccine was to be avoided, others had to be avoided as well, since combination vaccination products were often in use. Others claimed that they really did not know the difference regarding when their child was receiving the mercury based measles shot or some other non-mercury based immunization product. Still others felt that avoiding all vaccines made it easier to avoid the potential for autism or ADHD, and therefore gave their children better chances at experiencing an academically health childhood.
But still, childhood vaccinations are not the only vaccinations that are impacted by this kind of behavior. Other conditions that could benefit from vaccines were impacted as well, and in some cases it was the parent refusing his/her own vaccine of himself/herself based on this argument. For this reason, diseases not a part of the standard immunization program had peak refusal of care actions perpetrated as well on behalf of the overall parent’s health, not at all the overall child’s health. Such is a behavior possibly shared in other parts of the country, but most certainly one of the strongest indicators of the regionally defined high prevalence of childhood immunization refusals in the Pacific Northwest, and maybe even primarily or mostly in the Pacific Northwest.
The following are the national refused immunizations patterns.
- measles (variola), measles [grid]
- mumps [grid version]
- rubella
- diphtheria [12 sec. grid]
- pertussis
- tetanus
- polio [12 sec. grid]
- typhoid
- tuberculosis
- viral hepatitis [grid]
- childhood immunization refusals, all
- all standard, required immunizations in the above listing, combined
An important thing to note here is that immunization refusal to date has not impacted where these diseases prevail due to lack of engagement in this preventive medicine. The following demonstration are the places where immunized diseases occur, which does not spatially correlate with where immunization refusal patterns are refused.

.
Foreign Diseases
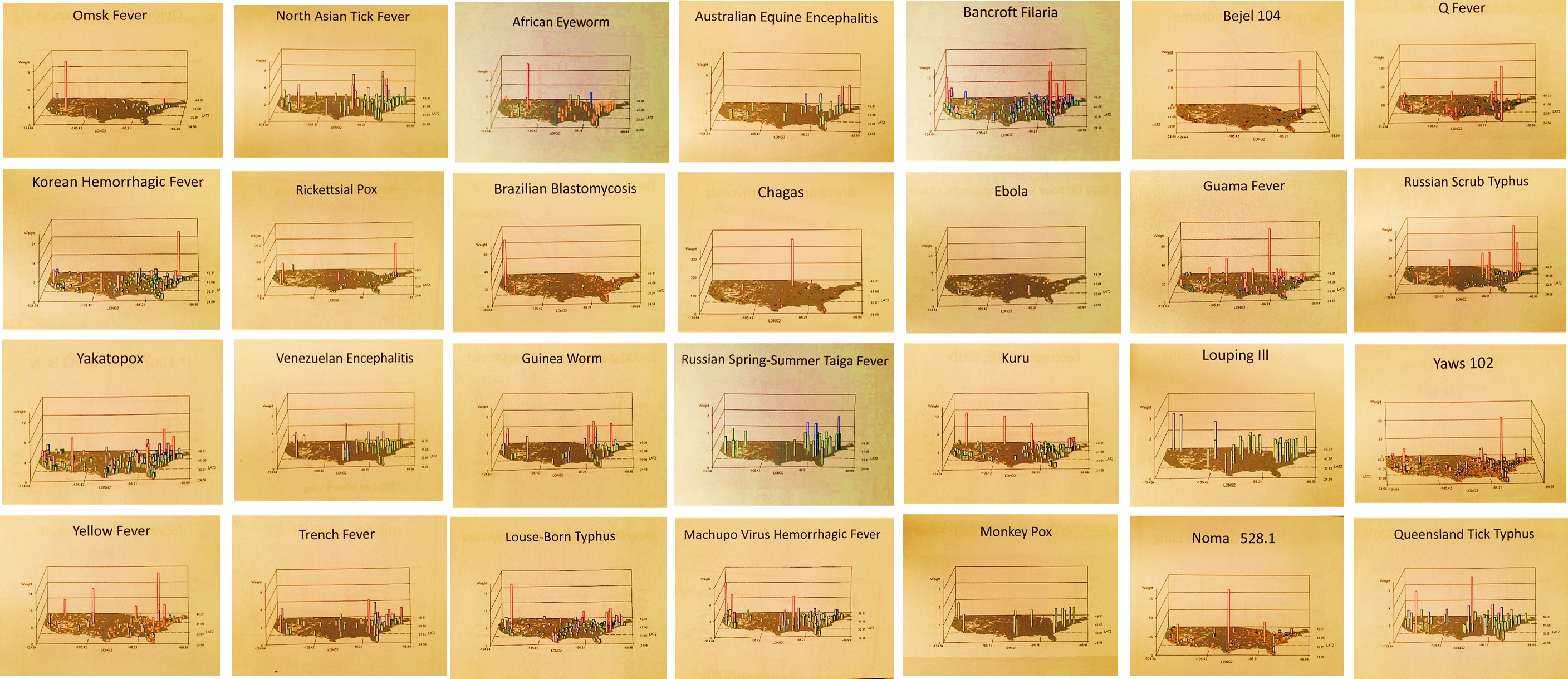
Foreign diseases pose one of the greater risks to the Pacific Northwest. At any time and place where ships dock for mercantile or passenger migration reasons, the opportunity exists for diseases to make their way to mainland. The most classic examples of foreign-born diseases are yellow fever, malaria, dengue and Asiatic cholera. Each of these can be mapped and the maps reviewed in respect to the Pacific Northwest and the oceanside urban settings for Oregon in various maritime towns, most importantly Astoria and Portland.
In general, there are several possible routes of entry of disease into the Pacific Northwest. There is the expected Pacific Rim route, the south-to-north Mexico/Central America in-migration route or path, and the north-to-south Vancouver, BC to US route (not mapped).
One of the first such diseases I researched back around 1999-2001 was tuberculosis. This was in part due to the large number of South Asian families from Vietnam, Laos, and Cambodia in Portland. These families immigrated to the United States during the late 1970s, 1980s and early 1990s. In the public health sector, there were primarily concerns for the tuberculosis that could be brought in by the elders of these groups.
With time, it became apparent as well that a number of psychological and psychiatric problems were being diagnosed due to the culture shock some members of these families had. These sociocultural aspect of a particular ethnic group’s health concerns provided an opportunity for a combined qualitative-quantitative review of this local sociocultural and public health issue.
A recent review of the congenital tuberculosis demonstrates a possible continuation of this public health issue. It is not known however if these cases are in high amounts in the Pacific Northwest due to peaking in urban settings brought about by Pacific Rim related migration and trade, or if these congenital cases are a result of local active cases still prevailing in the Asian and/or non-Asian communities less likely to be engaged in Tb testing and immunization practices. Another possible, but less likely cause for this spike in the Northwest is related to the local annual rainfall patterns, which results in very humid old growth forest settings, environments usually quite supportive of fungal organisms.
Ý
Yellow fever demonstrates a possible inland route from the north, not from the south as was expected. We expect this disease to enter this country from the south due to its ecological link to tropical ecological settings. But such is not the case with yellow fever. This may be due to ‘a lowering of the guard at the northern border’ so to speak, or due to migration of carriers across the country from both eastern and western shorelines and Great Lakes shipping ports into the interior.
In the case of Asiatic Cholera, a nidus is demonstrates for a single set of cases at the southern end of the Pacific Coastline in the U.S.
Ç
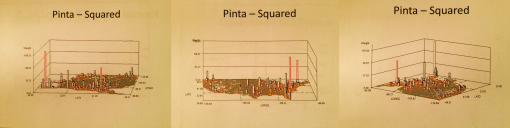
Pacific Rim disease in-migration patterns include those of the following foreign-born, vectored and/or zoonotic diseases:
[Insert]
Occupational Diseases
The following is related to an occupational disease pattern that is not unusual to the Pacific Northwest. This disease, mushroom grower’s lung, is common to the region due to the popularity of the mushroom growing industry. Back in the 1990s, while working on the form of Allergenic pulmonary disease experienced by lumberman, I also met up with a Shiitake grower who had successfully bioengineered the fungal culture and growing medium for an increasingly popular oriental medicine. During the conversation one could tell he had a partially obstructed airway due to spore-induced long-term edema and scarring.
The following map of this disease however showed the primary nidis for this to be in the midwest, not the Pacific Northwest. A review of this same industry in newspapers, magazines and journals shows that a fairly successful mushroom growing industry was established in this region as early as the mid-1800s.
Μ
Sociocultural Diseases and Culturally-bound Syndromes
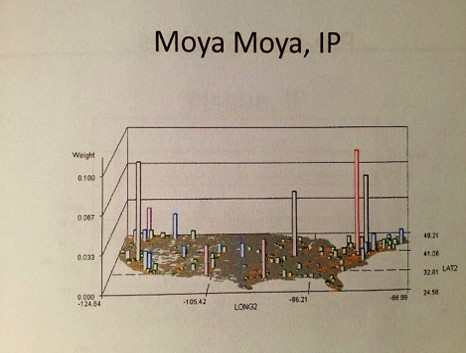
The Pacific Northwest is situated on the Pacific Rim. A large amount of commercial travel occurs along the Rim, and this had significant impacts on the Northwest’s Asian populations. There are a number of sociocultural syndromes linked to this demographic setting, and a few combination biological or anatomical-sociocultural disease states. Examples of these diseases are as follows:
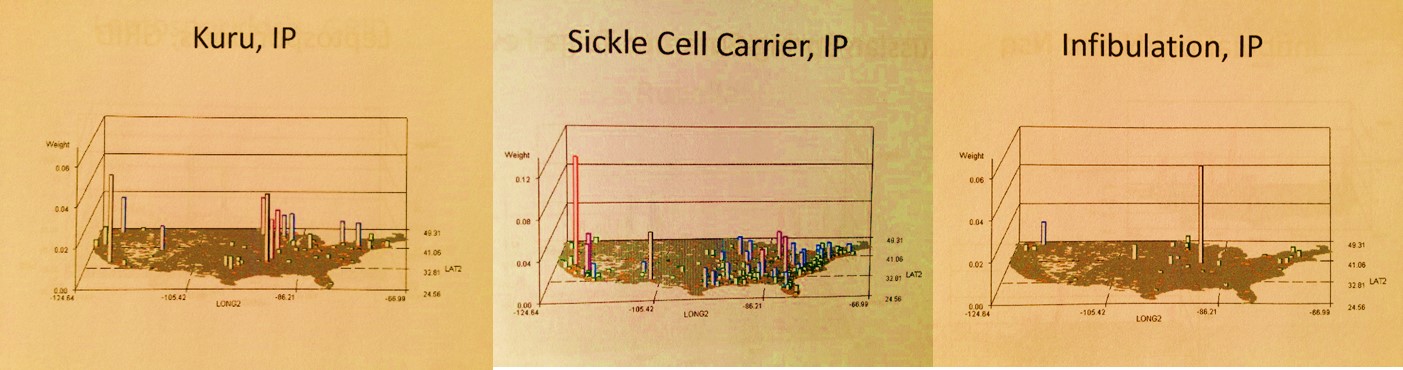
Some diseases are culturally-linked rather than culturally-bound. Culturally bound conditions are human behavioral related, and require a sociocultural belief system to develop and present clinically. Culturally-linked disease patterns are those which are somehow linked to a particular sociocultural group, but being a member of that group does not necessarily mean you are at increased rick for this condition, only that the history of this link, mostly genetically, predisposes in some way to the problem or condition.
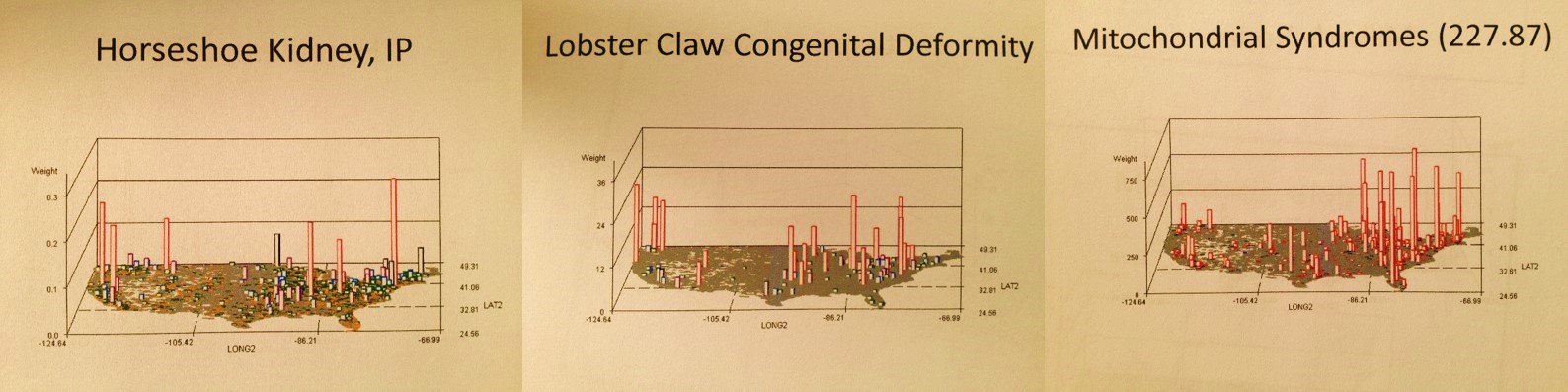
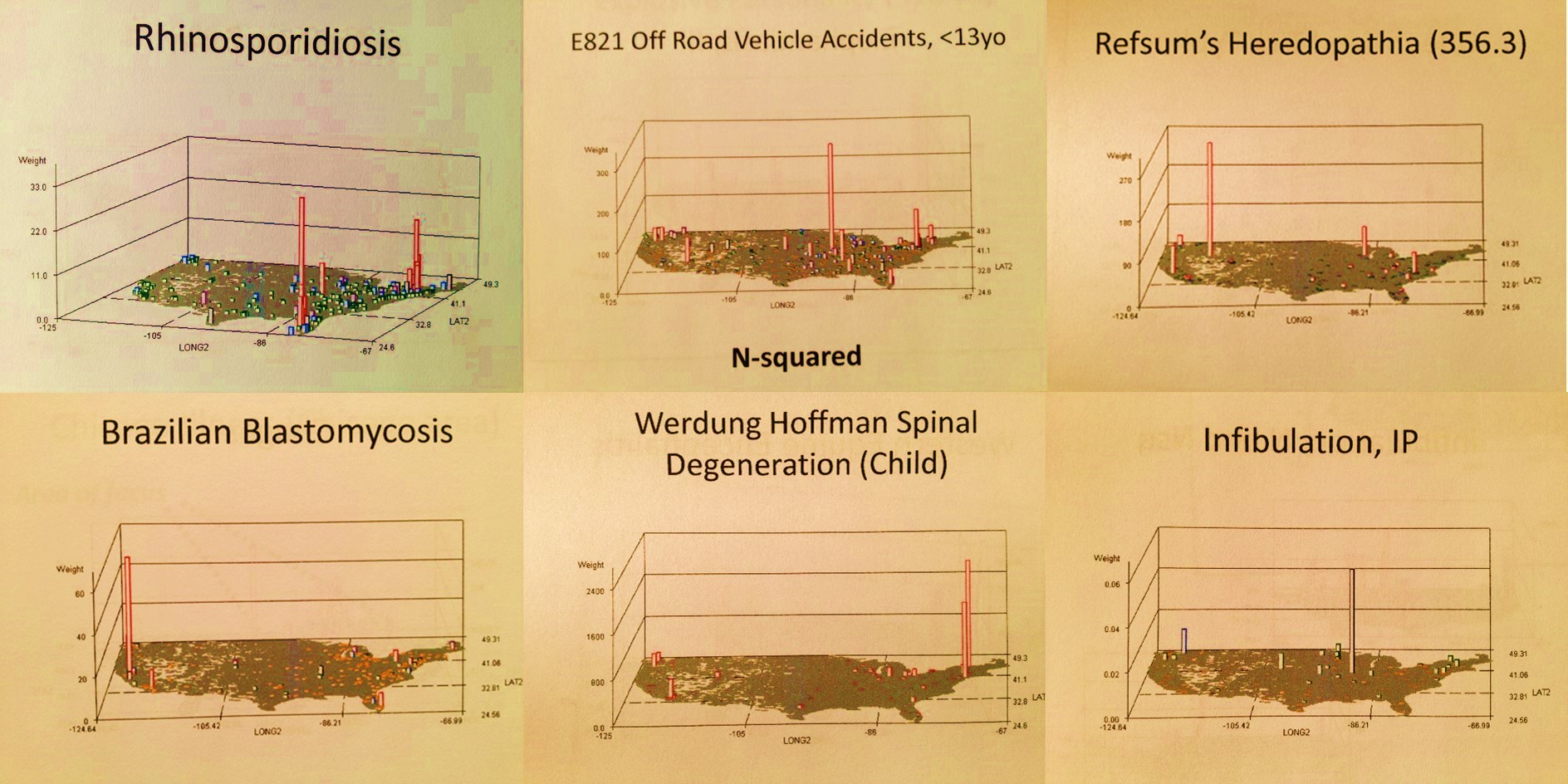
A classic culturally-linked disease is the African/African-American Sickle Cell disease and its carriers. Perhaps the most extreme example of a culturally-bound syndrome with physical and mental health repercussions is a form of genetic manipulations known as Infibulation. A more unique form of culturally-linked syndrome or malady or condition is Kuru, a non-infectious condition that is the result of foodways behaviors and practices engaged in within a specific African community setting. Within the Caribbean African-American community there is clay-eating, a form of Pica behavior. A very genetically based condition of African/African-American families is Obscure African Cardiomyopathy, no longer just linked to the African patient population. Physical disease examples of African-linked disease patterns include Yaws, which has links mostly due to its physical distribution on the globe, its origination and propensity within African settings, and Noma, a condition experienced only by the most impoverish communities, normally missionary settings. The African community experience with the metabolic syndrome, urban-linked chronic asthma-related COPDs, diabetes Type II, and even cervical and breast cancer, are the results more of human behavior, at the patient end as well as the health care provider end, than the results of genetics and purely family linked behavioral pressures.
The mapping of migration for the various census-defined ethnic groups helps to shed some light on the kinds of culturally bound syndromes that could occasionally arise in the Pacific Northwest. Due to the migrations in from the far north by the Inuit, Pibloktoq and Uqamairineq are likely (see page), for the Cree a condition known as Windigo. From Mexico and other parts of the Americas to the south are colerina, iich’aa and Susto. The Pacific Rim offers Pa-Leng, Koro, Shenjing Shuairuo, Taijin Kyofusho and perhaps Hwa-bung, all conditions we expect clinicians to learn about through the Oregon College of Oriental Medicine, a specific health plan not included in the State’s Medicaid and Medicare health coverage to any complete extent. The Latah of Malays has as its equivalents the following possible culturally bound syndromes available to impact Pacific Northwest patients: amurakh (Siberia), iekunii, ikota, okan, myriachit, menkeiti, Lapp panic (Lapps), bachtschhi (Thailand), imu (Ainu indigena of Japan), mali-mali (Philippines), silok, susto (Mexico), yuan (Myanmar, formerly Burma), jumping (French Canada).
As the varieties of culturally bound and culturally linked syndromes and diseases continue to grow, regular medicine on its own becomes less valuable and effective for treating these patients, more in need of the complementary, integrative practice counterparts.
Ï
Parenting in the Pacific Northwest
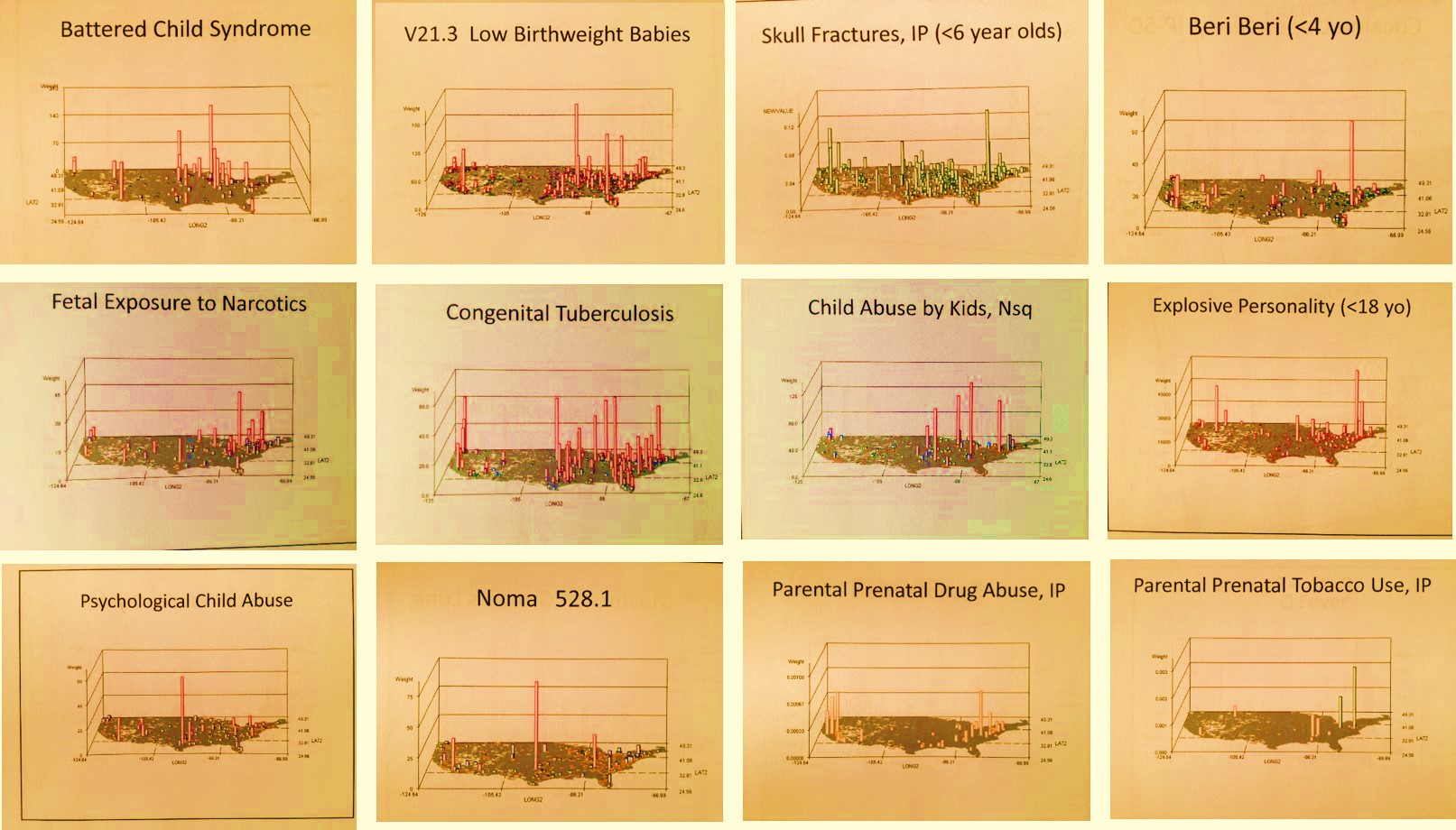
Aside from the immunization issue presented in the beginning of this review, there are a number of social and moral issues pertaining to parenting that are possibly in need of review for the Pacific Northwest. Certain ICDs, V-codes and E-codes can be used to identify these problems, some of which might even be considered valuable indicators for certain areas in the region most in need of interventions.
On my basic review of the map videos produced, the following topics are focused on parenting related issues with kids. Not all of these demonstrate problems within Pacific Northwest community settings.
Poverty and Human Behavior
- SIDS (Sudden Infant Death Syndrome), IP
- Desertion of Newborn [background noise/radio]
- Very low birthweight baby
- Children with inadequate material belongings
- Children with poor housing
- Childhood Nutritional Marasmus
- Childhood (0-3 yo) Beriberi
- Childhood Homelessness
- Young children struck by cars
- Physical Child Abuse, IP
- Psychological Child Abuse, IP
- Hepatitis Carriers, IP
- Physical Adult Abuse, IP
- Psychological Adult Abuse, IP
- Sexual Adult Abuse, IP
- Opium Abuse/Addiction/Dependency
- Cocaine Abuse/Addiction/Dependency, IP
- Homelessness, highest risk places, IP
The various health problems found to peak in the Pacific Northwest include the following:
- Low Birthweight Babies
- Off-road motor vehicle accidents involving children less than 13 years old
- Pedestrian accidents involving young children
- Hereditary and Developmental conditions
.

Social and Moral Issues
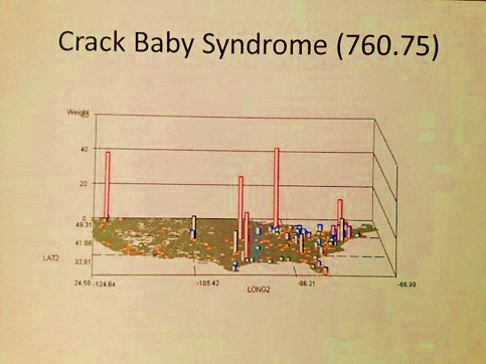
Along with poverty there is drug abuse, and along with drug abuse there is Cannabis use and abuse. Drug abuse and Cannabis use/abuse are not directly related. The utilization of cannabis can be linked to drug abuse behaviors, but not always vice versa. Portland, Oregon is the first place to have a law passed allowing for Cannabis use for medical related purposes. Denver would soon follow.

This preference for legal use of Cannabis is more a social phenomenon of the entire country than it is a particular event related to a particular part of the country. The ubiquitous nature of Cannabis smoking rights is noticeable in the related video map. Also note, this is a map of “dependency”, not abuse, and therefore also illustrates perhaps the reduced likelihood of receiving such a diagnosis in the Pacific Northwest, in part due to its local interpretations as ‘dependency’, ‘abuse’ or even ‘improper’ (not coded), by the clinicians at large.
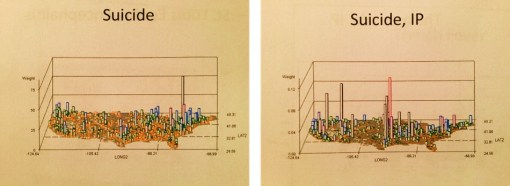
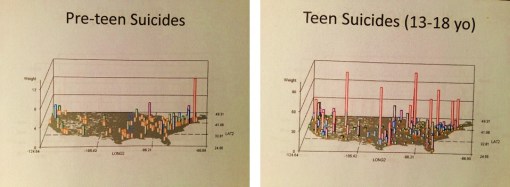
In this first video, suicide was reviewed for 19-25 yos. The Pacific NW has a problem with teen and young adult suicide. In this first video, a Suicide Peak in the Pacific NW is evident. Even though peaks to east are larger, PNW is more concentrated in terms of case density, and as contour map shows, is the nation’s peak for suicide by this age group.

At some sort of intellectual angle, a number of scientific theories have been proposed for suicides in general in the Pacific Northwest. The focus for most of these theories is the sunlight-melatonin theory, typically evaluated clinically through the use of sleep monitoring equipment and light therapy.
The most likely reasons for these suicide cases are not simple, but the high numbers of streetbound, homeless teens or runaway teens residing on the streets of Portland perhaps provide some clues for this problem. In contrast, we do not see Inadequate material belongings in relation to poverty as a claim common to children’s records for Pacific Northwest residents.
One of the most common crimes linked to these teens, and noted in the medical records, pertains to abuse of a child by an adult. This too can be mapped and evaluated relative to the other teen problems related to teen-rich urban streetlife communities. The most disconcerting of these maps is the last of the four, pertaining to the sexual abuse of children, a story common to the local news over the years along with the issues related to children, especially teens and young adults living on the street as part of the local homeless population.

.

Chronic Diseases in the Pacific Northwest (Urbanization)
High Cost Diseases in the Pacific Northwest
My other pages on sequent occupancy and epidemiological transition and/or my applications of this theory include the following:
.

{kind=link}
Leave a comment