 .
.
[Article] IV.—On the Geographical Distribution of Disease. The Substance of a Lecture by James Little, M.D., Professor of the Practice of Medicine in the Royal College of Surgeons. The Journal of the Royal Dublin Society. Vol. 2, no. 1, pp. 62-71. 1878.
Biography source: http://en.wikipedia.org/wiki/James_Little_(physician).
.
Introduction
Disease theories don’t just change overnight, and often, one theory doesn’t necessarily totally replace the other. And in cases where the old theory is wrong, we do not necessarily totally accept the fact that the new theory is absolutely correct. In some cases, we combine both concepts into some unified theory, as is illustrated by this article.
This is a case in which both the old and new philosophies each were partially correct. We can accept parts of the zymotic theory as substitutes for the terribly wrong parts of the miasma theory, upon which much of medical geography and the earlier disease maps have been based, but still, in spite of the value of this theory, there were some parts of the old philosophy that we could just not get rid of as of yet. Due to this, we see the hybridization of the old medical topography and climates theory with the new zymotic philosophies. This allows for the elders in the profession to retain some of their heritage as valuable doctors, whilst providing the younger the new route they need to take to advance their profession. Regardless of age, those in the same field want to accept a newer theory but not at the risk of discarding most or all of the older theories already out there. This is the route James Little took with this article, making it a classic example of how old theories give way to the new in medicine.
Even more amazing is that this article represents a merging of geographic theory with zymotic theory for the explanation of disease, coming from an Irish medical journal. There is less ego and pride underlying the writing style for this author, unlike those English writers who tend to be very self-centered, and even ethnocentric at times about their sometimes very personal discoveries. Little fills this article with all the necessary details we need to understand (and for students learn about) about the zymotic theory for disease, out there for others to learn during the 1840s but not very popular until the 1860s and 1870s. Like most level minded writers and thinkers, Little wasn’t naive to the new and upcoming theory for disease, which was only about 3 years away, the bacterial theory, and so mentions it in his writing. (In 1881, the bacterial theory was considered formally accepted.) Along with their coverage of zymosis and medical geography, physicians like Little provide us many hints about human behavior when it comes to medical discoveries. During their discussions about their knowledge of the up and coming new theories for disease or how to heal someone, new philosophies and mindsets develop, some reinforcing the old and others justifying the new, others merely a byproduct of these two common forms of human behavior.
This means that the particular year, 1878, represents a time when we can learn about three forms of medicine–the medical topography and climatology period in disease theory, the pre-bacterial or zymotic disease theory period, and the earliest stages of the bacterial disease theory period. It also demonstrates how early disease mapping philosophy and microbiology once again comes together in that old classical way, by combining the macrocosm of disease ecology and spatial epidemiology with the microcosm represented by how the way we interpret disease today, as a result of the zymotic and bacterial theories, a focus on the microscopic nature of diseases causes and its impact upon human physiology and body chemistry.
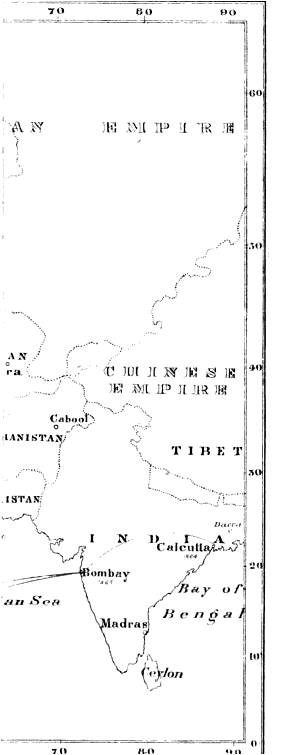
Unfortunately, there is also a map included in this article which I haven’t obtained a full version of, as of yet. It is an example of the problem we researchers sometimes have with Google Books and sometimes Archives.org books. In situations where efforts were made to speed up or facilitate processing, the copiers/photographers tend to disclude all of the much larger illustrations to speed up the processing and productivity. Unfortunately, as this book illustrates, important information is often lost through due to this part of the scanning process.
.
The Google Books partial map strikes again:
.
IV.—On the Geographical Distribution of Disease. The Substance of a Lecture by James Little, M.D., Professor of the Practice of Medicine in the Royal College of Surgeons.
In dealing with the subject of the Geographical Distribution of Disease it is desirable to keep in view the two great classes of disease. In the admirable lectures of Dr. Stokes and Dr. Moore you have already heard a good deal about one of these classes, namely, Zymotic Diseases. The derivation of this term almost suffices to explain the sense in which we apply it. It comes from a Greek word which signifies “leaven,” and under the term are grouped a number of diseases in which the disease-process is supposed to bear an analogy to that which is set a-going when leaven is added to dough. One of the most prominent members of the zymotic group is small-pox. When a certain quantity of the contagium of small-pox is introduced into the system nothing is observed for some time, but after the lapse of a certain number of days, varying from nine to twelve, according to the mode in which the poison is introduced into the system, changes begin in the individual—he becomes ill, various symptoms are developed, and there is a multiplication of the poison in his body. One of the essential character’s of these zymotic diseases is that the poisons which produce them are all received from without—the individual gets the poison from some source external to his body.
The other class of disease is the Diathetic. This term is derived from a Greek word which signifies “disposition.” There exists in the bodies of some people a disposition or predisposition to a certain disease, or more correctly to a certain kind of vital action which results in disease, and an essential feature of this class is that the cause of the disease is generated within the System of the sufferer, and is not received from without, as is the case in diseases of the zymotic class. Gout and scrofula are examples of diathetic diseases. Men do not exhibit the phenomena of gout or scrofula because some poison has gained access to their bodies from without, but because there is something wrong in the chemico-vital changes going on in their own bodies, because in them there is a disposition or predisposition to form an unhealthy kind of blood and tissue. Diathesis is sometimes hereditary and sometimes acquired, but whether hereditary or acquired it may be intensified or lessened by the habits of the individual and the circumstances in which he is placed.
Some diseases belonging to both these groups prevail in every part of the world, or nearly in every part of the world, but the majority are confined to certain areas.
I. Some are confined to a very limited area, beyond which they are never, or very seldom found; for instance, along a certain part of the coast of Hindostan and the opposite coast of Ceylon, between 15° and 20° north latitude, and extending not more than sixty miles inland, there prevails a constitutional disease known as Beriberi. In persons affected by it the blood becomes watery, and ultimately dropsy occurs; it prevails principally in gaols and overcrowded barracks. In this district many conditions unfavourable to health exist; we do not know the precise ones which determine the occurrence of Beriberi, but we do know that by attention to ventilation, the use of pure water, the avoidance of damp and cold, and the administration of small quantities of iron, persons living within the affected area may be protected from the malady.
II. Other diseases, again, though usually confined to a limited area, extend beyond it under exceptional meteorological conditions. For instance, in the equatorial region of America, extending from 48° north latitude to 35° south latitude, Yellow Fever prevails. In some part of this region it is always present, but it requires a temperature of 72° Fahr. for its propagation, and hence, although there is constant communication between the countries in which the disease prevails and England, and ships have several times arrived in British ports with the disease, it has never spread in these islands; it has spread, however, when introduced into ports in southern Europe, where the temperature and other circumstances were favourable to the reproduction and diffusion of the poison on which it depends.
III. In Cholera, again, we have an instance of a disease which has for some time prevailed in nearly every part of the world, and under very varied climatic conditions, but which nevertheless has a limited area of persistent existence from which its epidemic journeys commence, and where, after it has died out in other lands, it continues to prevail.
IV. In Influenza we have an example of a disease which has no persistent area, but which, arising sometimes in one part of the world and sometimes in another, spreads thence with great rapidity.
V. Finally we have diseases such as Goitre and Leprosy, which are met with in nearly every country in the Old and New World, but only in limited districts of these countries, where certain unhealthy influences generate and perpetuate them. Goitre is found in India, in the New World, in parts of England, and in Switzerland, but always where the water used for drinking contains lime in considerable quantity. Leprosy is a terrible disease, which once existed here. It prevailed in various parts of Great Britain and Ireland, and up to the end of the last century in the Shetland Islands; at present it prevails in India, in North America, in Equatorial Africa, and elsewhere, but whether in the warm or cold regions, in the Old World or the New, it always presents the same characteristics. It is an hereditary constitutional disease, prevailing among people who are badly fed, and live in filth and misery.
If, setting aside the two last classes, we proceed to inquire into the circumstances which cause the limitation of certain diseases to certain areas, we will find that temperature is the most powerful—so powerful is it found to be that some years ago Mr. Keith Johnston, the eminent geographer, constructed a map in which he divided the world into three great disease realms, according to isothermal lines; that is, according to lines passing through places of mean annual temperature. If we look at Mr. Johnston’s map we will find that the isothermal lines do not run parallel with the equator; nearness or distance from the equator is indeed the circumstance which has most effect in determining the temperature, but other circumstances often interfere to disturb the influence of this condition, and hence the lines of mean annual temperature at some points approach and at some recede from the equator.
The Torrid Disease Realm has its centre at the equator, where the annual mean temperature is 82° Fahr., and extends north and south to the isothermal line of 77° Fahr.; in it therefore we find the Southern States of North America, Mexico, and the northern part of South America, the great region of Central Africa, Arabia, India, and China. This realm includes the most unhealthy portions of our globe. Most of its diseases are of the zymotic class, and in their symptoms resemble the affections which prevail among ourselves during the heat of summer and autumn. Over the entire of this disease-realm intermittent fevers prevail. In tlu portion of it which lies in the New World yellow fever is the most wide-spread and fatal malady, while in that which lies in the Old World cholera is the most important.
Intermittent and remittent fevers are also frequently spoken of as malarious fevers, because they are supposed to depend on an emanation from the soil, to which the term malaria has been applied. The fevers which prevail in this country are called continued fevers, because in them from the commencement of the illness until its termination there is persistent fever, that is, persistent elevation of the temperature of the body above the limits of health; in intermittent fevers, on the contrary, after the patient has suffered for some hours, the fever subsides and does not return until the following day or until the second day. Some intermittent fevers are comparatively mild while some are rapidly fatal, but whether the fever has been a mild or a severe one the person who has suffered from it—instead of being protected from a second attack, as is the case after recovery from our continued fevers—has a permanent impression made on his constitution, so that for years after he now and then shows symptoms of the febrile paroxysm. Though it is within the tropics that these fevers are most prevalent, they are seen in a severe form in Southern Europe, and in a less severe form in Britain, and wherever they prevail a certain condition of soil exists, namely, an alluvial soil, which, never thoroughly dry and never completely flooded, is daily expose* I to a hot sun; heavy rains on the one hand and long continued drought on the other prevent the development of malaria, and it is most intense during the autumn when the damp ground is covered by decaying vegetable matter. In the deltas of great rivers, where an immense body of water finds its way to the ocean through innumerable small streams, as is the case with the Ganges and the Nile, malaria is intense; it also prevails where extensive systems of irrigation are carried out, and where there are undrained swamps. Some of those who are now present have no doubt visited the beautiful Basilica of St. Paul, a few miles from Rome, and have heard how the monks who have charge of it are obliged each summer to leave it on account of the fatal fever which is generated in the undrained Campagna, yet this region was at one time quite healthy, when the aqueducts and watercourses, which are now in ruins, carried off the water and kept the soil dry.
I have already mentioned a few of the characteristics of yellow fever, the most conspicuous disease found in the torrid realm in the New World, but as cholera, the prominent disease in the torrid realm in the Old World, possesses a far greater interest for us, I shall devote to it a little more attention.
Cholera,* as all here are aware, has from time to time prevailed over nearly all the world, but in most countries after raging for some time it dies out, and is no more heard of for years ; but there is one part of the earth’s surface where this is not the case. Somewhat similarly typhus fever has under certain conditions, which I am sure you will hear fully described by my friend Dr. Grimshaw, prevailed extensively in many parts of Great Britain and of the Continent, but in most of these situations it dies out as soon as the crowded camps or other aggregations of human beings among whom it has prevailed have been broken up, but in this country, and more especially perhaps in this city, typhus fever in isolated cases is constantly present, and under certain favouring circumstances becomes epidemic. Cholera has in Lower Bengal, and especially in the great towns of Dacca and Calcutta, a home; when its ravages have ceased elsewhere, it still prevails in this region, sometimes appearing in Isolated cases, and sometimes putting on the character of an epidemic. Here it seems to find the conditions necessary for its permanent existence or constant reproduction, or perhaps I should rather say in Lower Bengal there are circumstances which prevent the disease dying out as it does elsewhere. In the great Delta of the Ganges we find everything which is necessary for the development of malaria in its greatest intensity, an alluvial plain so flat, that for 200 miles inland it barely rises above the sea level, exuberant vegetation, vast expanses of jungle, a great network of rivers and canals, and a tropical sun; in the habits of the people too we find everything favourable to the spread of an epidemic. “A bustee or native village,” says Dr. Tonneore, ” generally consists of a mass of huts, constructed without any plan or arrangement, without roads, without drains, ill-ventilated, and never cleaned. Most of the villages and towns are the abodes of misery, vice, and filth, and the nurseries of sickness and disease. In these bustees abound green and slimy stagnant ponds, full of putrid vegetable and animal matter in a state of decomposition, whose bubbling surfaces exhale, under a tropical sun, noxious gases, poisoning the atmosphere, and spreading around disease and death. These ponds supply the natives with water for domestic purposes, and are also the receptacles for their filth. The arteries which feed these tanks are the drains that ramify over the village, and carry out the sewage of the huts into them. Their position is marked by a development of rank vegetation.
* The most complete account of cholera, and especially of the routes by which its epidemics have travelled, will be found in “A Treatise on Asiatic Cholera,” by C. Macnamara, Surgeon to the Calcutta Ophthalmic Hospital. London: Churchill. From this work the accompanying Map is, with certain alterations, borrowed.
“The entrances to these bustees are many, but not easily discoverable, while the paths are so narrow and tortuous that it is difficult for a stranger to find his way through them. The huts are huddled together in masses, and pushed to the very edge of the ponds, their projecting eaves often meeting together, while the intervening spaces, impervious to the rays of the sun, are converted into necessaries, and used by both sexes in common. In these huts often live entire families, the members of a hut all occupying the single apartment of which it is not unfrequently composed, and in which they cook, eat, and sleep together, the wet and spongy floor, with a mat spread on it, serving as a bed for the whole.
“The distinction of caste extends to these bustees; but it assumes in these places a new form, by the fact that some portion of them, called parrahs, are inhabited by people of one occupation or trade, whose habits of living give a distinctive feature to each parrah, and modify its general appearance. Amongst the Hindoos the worst and filthiest bustees are those occupied by Gowallahs, Coloos, Chumars or Moochees. Amongst Mahomedans the worst and filthiest bustees are those occupied by Garry wans and Khollasees. In bustees occupied by Gowallahs, in addition to the usual filthy tank, the water of which is used by them to dilute the milk sold for public consumption, there are pools of liquid filth covering a large surface, the area of one of them I have ascertained by actual measurement to be over 150,000 square feet.
“None of these villages possesses a single road, or thoroughfare properly so called, through which a conservancy cart or even a wheelbarrow can pass in order to remove the filth. This filth is laid at the door of every hut, or thrown into a neighbouring cesspool. Not a single hut in the village is properly built. The dwellings are badly constructed, crowded together without regard to ventilation or the means of being kept clean. The principal defects are due not only to ignorance and utter disregard of all sanitary considerations by the ryots, but also to the apathy and negligence of the impropriators, who care very little about the welfare of their tenants provided that their rents are paid regularly.”
This is a faithful and not overdrawn description of village life in Bengal, and it presents to us conditions eminently favourable to the prevalence of such a malady as cholera. Observation at home has shown that some diseases, markedly typhoid fever and cholera, are very frequently spread by the emanations from the sick finding their way into the drinking water, and thus gaining access to the bodies of the healthy. Now, the drains which Dr. Tonneore describes, though usually stagnant and invariably receptacles for the refuse of the huts between which they flow, during heavy rain are flushed, and discharge their contents into the neighbouring tanks from which the drinking water of the village is drawn. Need we be surprised then that in Lower Bengal cholera never dies out? and it is from Lower Bengal that it invariably sets out on its epidemic journeys. The routes it has followed on these journeys have been various, but the more closely we examine them the more convinced will we be of the truth of the doctrine taught long ago by the late Dr. Graves, that cholera travels along the highways of human intercourse, carried from city to city and from country to country, as the case may be, in the caravan, in the crowded ship, in the coach in the olden time, or in the railway carriage in our own day. Before us we have a map on which is shown the route by which it reached Ireland on its last visitation.
In the beginning of the year 1864 every part of the world was free from cholera except Bengal. The disease had died out except in its endemic area, but during that year it spread through Central India and into the Bombay Presidency. There are several places in India to which, at certain seasons, vast numbers of the natives journey from great distances; at some of them fairs are held, to others they go on pilgrimages. Into these assemblages cholera was introduced by those who had come from Lower Bengal, and when the gatherings had broken up the individuals who had contracted the disease earned it with them to their native towns, and so it was found that in 1865 cholera prevailed as a severe epidemic in Bombay. Between Bombay and the Southern Coast of Arabia there is constant commercial intercourse, and in March, 1865, cholera was raging at Mokalla and Mocha, to which it had been earned by native traders from Bombay. Now, this year, 1865, was one of special importance in the Mahometan calendar, and during the early summer devout Mahometans set out from every country in which that faith prevails on a pilgrimage to Mecca and Medina; they came from the East, from India and China, and the Indian Archipelago; they came from the West, from Turkey, and Egypt, and assembled to the number of 90,000 around the holy cities. Among the vessels which conveyed them were two, the Persia and the North Wind. These ships came with pilgrims from Singapore, and after calling at Mokalla disembarked their passengers at Djeddah, the port of Mecca; but between Mokalla and Djeddah cholera appeared among the passengers, and with them it found entrance into the assemblage of pilgrims around Mecca. These unfortunate people were living under conditions in the highest degree favourable to the spread of any pestilence; they were crowded together, very scantily supplied with water, and surrounded by every kind of filth, and by the remains of the animals which had been sacrificially slaughtered. It is believed that 30,000 persons died, and those who were left hastened away from the plague stricken encampment. As I have already mentioned, many of the pilgrims came from Turkey and Egypt, and on May 19th the first ship with returning pilgrims reached Suez; many of the passengers had died of cholera during the voyage, the others were immediately conveyed by rail across the isthmus to Alexandria, where they encamped outside the town. The condition of Alexandria and its environs at this season was eminently favourable to the multiplication and diffusion of the contagium of cholera. In a less degree Lower Egypt presents the same features as Lower Bengal. It is the delta of a great river; it is exposed to an almost tropical sun; its vegetation is luxuriant and its inhabitants are uncleanly. Here cholera broke out and prevailed with great severity. The port of Alexandria too is the place of all others in which the greatest facilities exist for the rapid diffusion of any pestilence. In it you may see every day the flag of almost every European nation. It is the great highway between Europe and the East, and from it are daily starting English, French, Russian, and Austrian steamers. The first case of cholera occurred at Alexandria on June 2; on June 11 it was at Marseilles, on June 28 at Constantinople, and on July 7 at Ancona. Considerable precautions were adopted to prevent its entrance into English ports, and it did not appear at Southampton until September 17; it did not spread there nor did it come to Ireland by that route. We have now reached the autumn of 1865. During the autumn and the ensuing winter it prevailed in various parts of northern Europe; it had found its way there by two roads ; from Constantinople it had spread along the shores of the Black Sea and up the Danube, and by a totally different path it had gained access to the very heart of Europe. Not a few of the pilgrims who fled from Mecca were Persians, and they journeyed homewards along the coast of Arabia and up the Persian Gulf; they carried the cholera with them up the Gulf, along the valley of the Euphrates, to the shores of the Caspian Sea, and hence it was soon carried into Russia. Reaching northern Europe by both these routes in the spring of 1866 it prevailed extensively in Holland, and on May 2 two persons who had just arrived from Rotterdam died of cholera in Liverpool; and, beginning in the streets inhabited by the Dutch and other foreign emigrants and sailors, cholera spread through various parts of Liverpool. On July 26 a girl died of the disease in Dublin, and on investigation of the case by Dr. Mapother it was discovered that she came from a Liverpool lodging-house frequented by these sailors.
The Arctic Disease Realm extends from the isothermal line of 41° Fahr. to the poles. In the countries lying in this region there exist many conditions unfavourable to health; extreme lowness of temperature and dampness are among the most powerful; in this region vegetation is less rapid and luxuriant, and the great body of the people have a less abundant supply of food; nor must we omit the long nights and short days and deficient sunlight from which those countries which approach the poles suffer.
The lowness of temperature indeed is not an unmixed evil, for it is eminently unfavourable to the spread of zymotic diseases, which, in consequence, seldom prevail in the Arctic realm. It is from constitutional diseases that the inhabitants of countries within this realm chiefly suffer; the conditions under which they live are unfavourable to long life or vigorous health, and they suffer in consequence from scrofulous diseases, and other diathetic diseases characterized by a low standard of vital action.
Between the torrid and the arctic disease realms lies the Temperate, in which our own land is situated. The diseases met with in this realm will be largely discussed, I have no doubt, in the subsequent lectures of this course; they are due less to the climate in which the inhabitants of this region live than to their habits—to the artificial life they lead and the various unfavourable conditions imposed upon them by the crowding and the struggling for existence in our great towns, and the still more unfavourable influence exercised by their vices. The deadly miasm of the tropical jungle does not kill more surely, the bad food and sunless winter of the polar regions do not lower the standard of health and shorten life more certainly than does intemperance, which, in these lands, at the present day, prevailing as it does, among rich and poor, seems likely to inflict a blow on England’s greatness more deadly by far than any we could receive from pestilence or war. Zymotic and diathetic diseases are to be met with in about equal proportions in this the temperate disease realm; among the former we have typhus fever, the crowd-fever of the poor, and typhoid fever—a malady which seems very intimately connected with the extensive system of sewerage which the arrangements of our modern houses require, and is hence as commonly, nay more commonly, met with in the mansions of the rich and the comfortable homes of the middle classes than among the very poor; it is the fever which is endemic in many of the large continental towns, such as Naples and Geneva, and which in these cities not unfrequently causes the death of English tourists, who, coming freshly under the influence of the miasm, are specially liable to be affected by it. Conspicuous among the diathetic diseases we have consumption—a malady which is the expression of a low state of vitality, however induced, but which recent observation has shown to be in a great degree preventable; investigations carried on in England, under the direction of the medical officer of the Privy Council, have brought to light the fact that the mortality from consumption stands in a very constant relation to the dampness of” the soil, and that where effective drainage has diminished this the mortality from consumption has, in proportion, been lessened. In Salisbury the consumption death-rate has diminished one-half since the town was thoroughly drained.
The subsequent lectures of this course will, if I mistake not, impress strongly upon you this fact, that it is not only the duty but the interest of the rich to care for and to seek the health of their poorer neighbours; you will learn how the fever which is bred in the lanes and alleys of our city creeps into the broad streets and open squares, and the facts I have mentioned teach the same lesson. I have shown you how the pestilence, which finds the conditions necessary for its permanent existence in the undrained swamps and filthy villages of England’s great dependency, travels thence until it reaches the busy hives of” English industry and gathers its victims from the mansions and homesteads of Britain itself.

Leave a comment