. PREFACE I can start off by stating that “the Extraordinary disease” that struck Nantucket in 1763, and referred to by the writer of this article, was not yellow fever, or at least not just yellow…
Sourced through Scoop.it from: brianaltonenmph.com
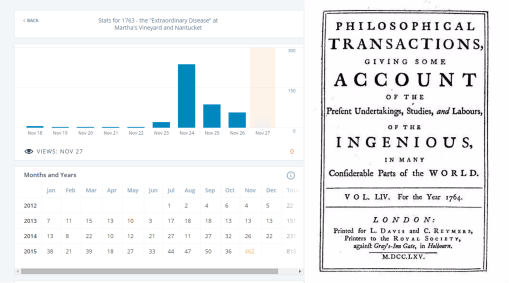
A few days ago, November 24th, I had 450 people visit one of my historic medical geography pages. This page reviewed the epidemic that stuck Martha’s Vineyard in 1763.
I use two well tested theories to evaluate this diseases most likely to strike this setting during some of the earliest years of colonial history. Sequent Occupancy and its equivalent idea penned around the same time by Benjamin Rush as a variation on the newly population Erasmus Darwinian evolution theory.
Erasmus Darwin (grandfather of the famous Charles Darwin, founder of the more modernly accepted evolution theory), identified the concept of speciation [“Speciation transition theory”], in which beings develop as a consequence of their ecosystem. Applying this to humans, Rush stated that as people mature and their work environment and community mature, so too does their way of living and occupation (see “1786 – Benjamin Rush – An early rendering of Sequent Occupancy” at https://brianaltonenmph.com/gis/historical-medical-geography/1786-benjamin-rush-an-early-rendering-of-the-sequent-occupancy-philosophy/ ). Rush referred to these periods of sequential development in reference to the different “species” of mankind they produced. Man’s way of living, building houses, setting up business, raising or grown food, all changed as well as a result of these changes in the colonial setting. To contemporary readers, this seems figurative at first, but a review of the Erasmus Darwinian theory makes sense of it–that theory claims the same natural events and forces occurred throughout nature, not just to plants and animals, but also to stones, the environment, mankind, etc.
In the late 1800s, the geographers reiterated Rush’s theory, without knowing he had in fact already invented it, when they described the sequent occupancy theory for how people evolve and change as the place they live in changes as well (“Epidemiological transition”, at https://brianaltonenmph.com/6-history-of-medicine-and-pharmacy/hudson-valley-medical-history/european-multiculturalism/moravian-indian-medicine/medical-changes-over-time/ ). These changes in the immediate environment are a consequence of changes in prevailing occupation patterns, prevailing resource and product needs, and prevailing skills and knowledge based needs in order for that business and its factory or industry setting to develop.
For each of these E-Darwinian evolution-ecology states, or Rush species periods, or sequent occupancy stages, come a specific set of medical conditions and disease types. This direct relation of these three paradigms all precede the contemporary epidemiological transition theory by just a few decades.
Now of course, sequent occupancy, speciation, and early E-Darwinian ecology are not perfect matches for epidemiological transition. Like any theory that exists in today’s scientific community, older theories undergo change and upgrading every now and then. Sometimes they fade out, only to return years or decades later in some new form, supported by some new paradigm.
Sequent occupancy is a far better way to map diseases and health over space and time today, as much as a century or two ago. It is as much a valid theory for geographers to use in their studies of spatiotemporal disease patterns, as the traditional ecological theories are for the biological fields, or the demographic-environment theories are for pathogenesis.
Sequent occupancy is here for spatial analysts to use to study their topics with. It provides a much better, more specific format to carry out this research with, defining as well the observations that need to be recorded and discussed to help show a value to sequent occupancy theory to the modern spatial epidemiology studies.
This page more than likely had such a great following during the first days of this week due to its sequent occupancy and review of history and health for a time when colonial medical theories prevailed. Colonial medicine beliefs were very different from those of today–few overlap, except at the sentence level–we still occasionally uses leeches to treat the human body for specific conditions. We bloodlet patients, but only those who are hyperemic. We reserve religious beliefs for disease, but fall upon other culturally-related belief systems to try and explain our sickest behavioral health patients. Some doctors believed in metaphysical theory and applied acupuncture to patients, for the electric energy or vital force it transferred, spread or helped to develop. Such a philosophy differs extremely little from today’s reasons for why we want to rely upon acupuncture for treating certain medical conditions, such as back pain or even cancer.
Whatever the reason for its high popularity right now, this item out of the U.S. medical history represents one of many examples of the value of historical medical research, for use by today’s healthcare and medical research projects. Very few medical scholars know and understand medical history. They often re-write its meaning, purpose, definition and intent for the philosophy, in order to make it fit better with their own modern paradigm.
But theory is theory. Theory works when we can make it work, and when if works real well, deserves to be tested for more applicability. The sequent occupance part of this highly popular page, and its example of how epidemics in the past can be so hard to recognize and decipher when penned by non-medical writers, and why we must engage in this kind of work to better understand some of today’s medical and public health issues, are the main reasons this many people took to this page on the epidemic that struck Martha’s Vineyard, nearly 250 years ago. In it, I provide as well as contemporary historian’s take on the cause for this disease centuries ago; but the underlying basis for this modern diagnosis is so wrong in terms of time and place. To make the right diagnosis today, it helps if we know the full history, even of the disease we are trying to decipher and diagnose.
See on Scoop.it – Medical GIS Guide

