 This article is focused on the 1863 map of Erysipelas.
This article is focused on the 1863 map of Erysipelas.
(And is a work in process)
For population history of Chicago, see animated map series.
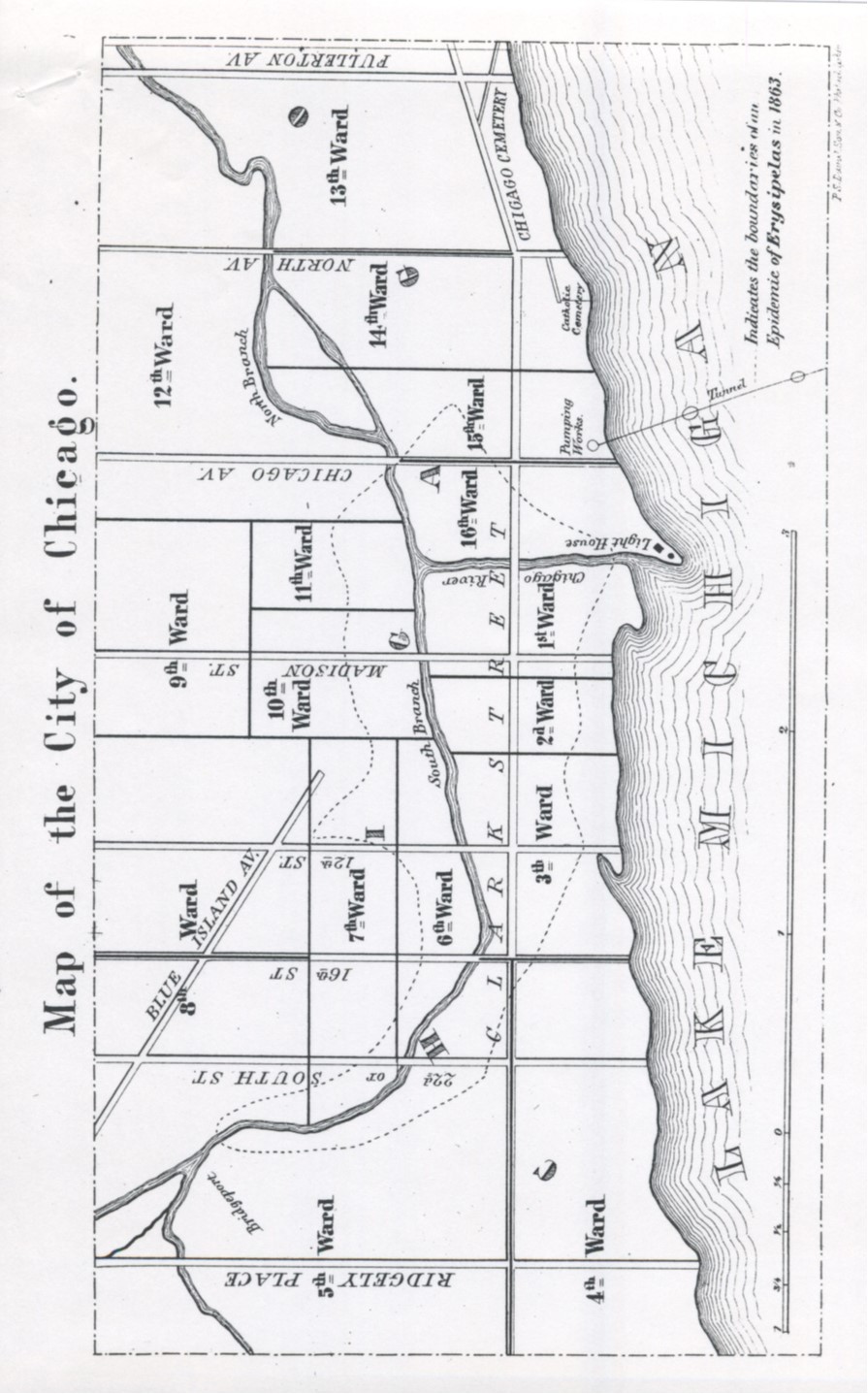
The above is the original layout of the map in the journal. All other versions of this are rotated 90 degree clockwise.

Section of “The Temptation of St. Anthony” by Hieronymus Bosch (ca. 1500). To the left is the St. Anthony’s Fire that struck France. To the right is the opposing force of natural coldness and crisp air, the causes for influenza and catarrh (the sign of “the cold”). Ergotism is depicted as a fiery epidemic flying over a city in France, perhaps Lorraine, reminding onlookers of the mal aria or miasm as well. In the United States, the term St. Anthony’s Fire was also used to refer to Erysipelas. Both of these natural causes — fire and wind — helped to define the diseases of Chicago in its early years.
.
.
St. Anthony Visits Chicago
Erysipelas is a disease of two or three types, depending upon the references you read. There is the traditional form of erysipelas that we refer to today known as the disease caused by Streptococcus bacterium. More traditionally there was this form of Erysipelas known also as St. Anthony’s Fire, a condition brought on by the effects a fungus which grows typically on the spikes of rye of ergot. The third form of disease close to erysipelas is due to the bacterium Erysipeloides, a species which penetrates the skin and resembles a mild form of eryisipelas.
Prior to 1870, it is possible that any of several other forms of erysipelas may have taken place as well, which although known by this name weren’t at all the same types of infection. These would have been cases of infection brought on by other bacteria caused a severe reddening of the skin in streaks, or the sensation of intense burning in sections of the skin that become red, inflamed, and even blistery in appearance. Such cases were common to extensive injuries and following surgical procedures due to the lack of clean practices in medical settings and the lack of effective antibacterials like carbonic acid.
From 1825 to 1845, erysipelas existed mostly as this latter form. The growth of Chicago made it possible for the changes in land use to be made for the more severe erysipelas to develop by the late 1850s. Between 1857 and 1862, the factors required for this more serious form of erysipelas were evident. Slaughterhouses that managed one or two thousand heads of cattle per day began to operate just southwest of the downtown Chicago setting along the south branch of the Chicago River. These facilities made it possible for the first epidemic to develop.
[]
Due to this particular layout of the factories just outside the bustling city of Chicago, people living in the urban core were exposed to the Streptococcal form of Erysipelas. Now it was time for a full fledged and real form of St. Anthony’s Fire to strike the city. To traditionalists ready in the religious history of the famous epidemics of the past, this may have at first seemed like another one of those famous Moses red tide events, or perhaps another example of the plague coming about. In American history, its first form of return was the yellow fever of the late 1790s into early 1800s, a couple decade later, the Asiatic cholera epidemics of the the 1830s and 1840s into 1850s were also considered equivalents to the plague.
(yellow fever-cholera scourges)
But even more so Biblical perhaps, when it came to interpretation by Bible Belt inhabitants, was the cattle plague of Mosaic time. Beginning in 1840 but definitely in 1856, a bovine epidemic resembling the cattle plague of Moses’ time, which made its way from Texas to Missouri by way of infected steer, and from the regions up north by Ohio diffusing south. The former caused by a tick these livestock carried with them, not God’s hands, or any demon natural to nature.
A common perception during this time of disease and its severity relied mostly upon one symptom, and one cause, known on and off as the unity theory of disease. The unity theory stated there was just one cause for all illness, and that how this cause effected you is what resulted in how the disease presented itself. This was very popular in the late 1700s but prior to the Revolutionary War years, and pertained mostly to an energy concept in the body traveling about, creating havoc with one organ and then another. This to many seemed much like a vital or life force concept that could be involved. The inclusion of Quaker ideology in medicine just a decade or two later, in the early 1800s when many leaders of U.S. medicine were in fact Quakers, would effectively make this philosophy very popular. Likewise, when it became popular again and again, as philosophical movements during the the birth of the Leyden jar theory (1690s -1715), early galvanism (1797-1806), medical (static) electricity (1797-1812), the birth of homeopathy (1806-1815), early European promoted acupuncture/moxi philosophy (1665, 1810-1825), transcendentalism (ca. 1830 +/-), what we find is we have so many metaphysical periods overlapping in medicine that it was hard to keep nature out of this picture. The earliest natural philosophy theories for epidemics were as we might expect. Nature caused diseases in many ways, and all of these could be called a form of miasma, which they were. In 1847, German geographer Adolph Canstatt redefined miasma to be of many forms and effects. Its various causes he defined as all of the above natural forces and events, such as comets, meteors, meteor showers, sunspots, geomagnetism, full moons, blue moons, aurora borealis, tornadoes, lightning strikes, volcanic eruptions, earthquakes, tsunamis, etc.
[]
If we take a look at the various theories for why cholera struck so fatally from 1849-1853, many of these same ideas are provided in the American medical literature. Could some of these be a result of the German migration of prior years?
By 1856, the numbers of causes for cholera in nature made the cholera seem to be a catch all disease that could be formed by any of a great number of natural events, ranging from weather and climatic changes to hydrological and pedological, or topographical and land use changes. Even a meteorite was blamed in some of the cases for an ensuing spell of cholera cases. An unusual group of cases on the west side of a city might be blamed on the local rotting apple crops and the combination of western side climates and terrain features, whereas the more exposed eastern side of the same city with its fields of flowers instead of crops might make some one blame the disease on the type of farming, the till and smell of heavily manured land, or the exposure of that part of the city to too many eastern winds. It was very easy to fall into that category of being a professional or amateur medical climatologist and medical topographer who believed that primarily weather and terrain defined disease, providing you with a reason to use local natural features to define the miasma concept to explain each and every type of miasma there could be in this natural history setting.
These forms included those traditional forms, like the miasma of a swamp or a swamp gas, or some rotting flesh, or an overexposed pile of rubbish just south of the town exposed to too much sun and hot, humid air. The 1850s claims for cholera mimicked bits and pieces of these German concepts of disease, and need we be surprised at this? After all, it was about the time that this philosophy evolved that the Germans were rapidly migrating to the United States. Kept up in their culture’s history and news, they would have been very familiar with the new and ingenious design of nature’s causes for illness, concepts that the Anglican European cultures were less willing to accept, adapt to or even listen too. They had to define these discoveries for themselves, on their own. This is what they did with the 1850s articles on “cholera” in general, which would have prevailed when the erysipelas came to Chicago in 1862, had not another philosophy taken stage in the English writing and speaking portion of the medical community. In Illinois for example, when cholera struck, the Germans shut the shutters on their windows, whereas the Irish never interpreted the disease as definitively caused by the wind of airborn miasma.
Without knowing the true cause, with each recurrence of a disease or introduction of another, physicians were also trying to determine if diseases recurred in cycles. When a new disease came to a region, they asked how does it relate to the past epidemics. Could the philosophy used to explain those events also be used to explain why this new disease has struck.
When the erysipelas came to Chicago in 1862, this event resulted in two stories that need to be told. Erysipelas that struck Chicago in 1862/3 be worse than ever before? Perhaps as an example of a cycling of severity, or due to some natural rhythm in nature, such as in the winds and weather patterns?
The logic that ensued in trying to explain the Erysipelas took two paths. The first was the traditional philosophy as just discussed, although not in the traditional sense. We had our own environmental theories were were dealing with. American doctors and English or British trained doctors afforded minimal respect to Canstatt’s teachings and philosophy, even though over time they believed in it fully, part by part.
During the five or ten years that it took for Chicago to change from a cow town with limited economic potential and value, to a bustling, young and budding metropolitan center, the medical theories for disease were changing.
Turning to the modern interpretation of theories for disease and how these theories for how disease changes over time developed, the epidemiological transition model now popular is barely enough to define the changes in diseases and place over time. Sequent occupancy theory is a better way, and the same physicians with a geographer’s take on health and disease were also applying their Erasmus Darwinian-Lamarckian-Darwinian philosophy to this problem.
Some of the best, clearest examples of what epidemiological transition consisted of can be derived from the geographer’s sequent occupancy theory. The traditional epidemiological transition paradigm is just that, only a paradigm, a way of compartmentalizing what we know in order to search for new venues towards learning. Sequent occupancy theory provides us with a better route to take.
, not that fairly broadly defined transition of a living place from that of a developing country to that of a developed country, of from a mostly countryside rural based way of being and living to a suburban to urban like setting, richly occupied and heavily settled by more than just a handful of buildings, Employing the contemporary model of epidemiological transition to a rapidly changing landscape barely does service to the complexity of changes that happen when a place or country becomes more economically established. In a purely traditional, more spatially defined way of looking at such a change, we see the value to the geographer’s sequent occupancy theory over the less specific, harder to break down epidemiological transition theory that is now out there in much of the history of medicine literature.
The story of Chicago itself is more accurately told as an example of sequent occupancy, than as a simple two step transition process of poor to rich, unsettled to overly settled people like the epidemiological transition tends to portray. The details about how and why we get sick are better told based upon the kinds of lives we live, the work we do, how we interact with our environment, and how we change this environment over time, removing from the natural setting that it once truly was. As we change a piece of property to something we can learn to live upon and with, a place which we can truly call our home, and yard, and everything else attached to the kind of social beings we all have become, we also see the consequences of these changes that take place.
We see some plants and animals die off. We see rolling hillsides get replaced by manmade steppe-like garden settings. We see lakes become smaller and swamps disappear. We watch as wildlife becomes either backyard neighbors or distant tales from a past hedonist setting that soon will no longer exist.
This is exactly what happened as the place in and around what is Chicago became the city that we call Chicago. From the Miami and Illinois term shikaakwa standing for wild onion or garlic, this setting was obvious known for its most pungent weed that frequents all of the woodlands and fields, the edges of lakes and swamps. Chicago was recognized first for its wild aroma and lack of habitability, a feature that led many to feel like they were back home in New York as the first cabins and forts were built by settlers heading eastward out of the Eastern United States. The exploration of Chicago, being largely due to the financial support obtained from New York, Philadelphia and some settlers to the south near Washington. Was like exploring their own prior homelands setting of a century or century and a half before. Any cattle you brought into this region were going to eat the garlic that grew wild at some point in time and their milk would become spoiled like it does in New York due to these habits typical of bovines. The only way to rid shikaakwa of its shikaakwa nature was to settle it, remove the traces of the wilderness that lie all around, and turn this rugged wilderness into a pastoral setting. Replace the natural grasslands with wheat and corn, convert the wild prairieland flowers setting into domesticated gardens and fields for livestock to frequent. Change the edge of the lake into first a hamlet, and then a village. Build a fort where there was no fort built before other than occasional native built shelters and such, turn the worst of the worst of outdoor settings into something as close as possible to the Garden of Eden needed for this latitude and longitude setting. This is exactly how the first settlers of Chicago interpreted their roles when making plans to settle this region, and later, make plans to move west and to occupy this region and thereby form its first roads, schools, and businesses.
Thus were stages 1 and 2 of the sequent occupancy history of the Chicago region, as it would have been interpreted by past scientists and physicians penning their geographical interpretations of these new parts of the New World, people like Benjamin Rush. Industrialization was more than just the blending of farming and factory goods.
[]
Benjamin Rush’s interpretations of places like Chicago are eluded to in an essay he presented to the physicians in England in 1787. In this essay he discusses the three stages or forms of occupancy of the countryside in the new world, these stages referred to as species of settlers or occupants, as if species was a word of traditional evolutionary, taxonomic classification use that did have applications to people and cultures as well (which most believed it did).
There were a number of sequent occupancy events, not epidemiological transition stages, that Chicago had to go through to develop the erysipela epidemic the way that it did, when it did. Sequent occupancy is the best way to look at the public health history of Chicago in the mid-1800s.
[]
Chicago first offered to people its rugged wilderness to contend with, but we imagine this ruggedness too densely perhaps. Chicago was at the western edge of the Great Lake of Michigan. From its onion-rich swampy settings westward and southward there was nothing but flatlands. The great wilderness that exist up the Hudson River and along the edges of the great lakes in the northern part of Michigan were not as rich in lumber and pine tar stores as they were elsewhere. But they were rich enough in these products to allow for early settlements. The outdoors in this setting had less of a landscape or topography to guide and protect it from the winds, no matter which one of any of the 360 degrees of flat space surrounding it these winds naturally came.
Winds from the north were in their most natural state, except for the impacts that the lake offered. They ranged from very cold to very hot and humid depending upon the time of the year. They were of that freshly aquatic to putrid miasma rich swamplike aroma depending upon time, place, temperature, water levels, man’s habits, animal’s ability to survive. The winds from the south, were not cold or humid like those from the north and east, but were usually drying slightly, but hotter. Even the tepid winds could make a man ill the settlers sometimes thought. By living on the edge of the Great Lake next to Chicago, you risked yourself to exposure to the Canadian and Great Lake winds that gave you the Cold or helped you to have Catarrh, influenza or even worse, a cold blocked lungs filled with water down below–the condition later called pneumonia. As a wildernessman you suffered the consequence of being in the wilderness.
But pretty soon the place was more settled and ships made their way in and out of the region quite frequently. By 1810 or 1815, they became capable of bringing with them the pestilence needed for fevers to develop. About this time, fevers were names for their water bodies and lakes, and so Chicago Fever may have very well prevailed during these early years had too many people remained there permanently.
However, Chicago settlers kept losing their lives to the indigenous groups around. Our measles and small pox may have created havoc in their communities regarding health and livelihood, but this known threat of their being nearby didn’t make for early successful neighborhood settings for the two. Perhaps for self-survival if nothing else, the Indians of this region several times wiped out the races of Europeans and Euro-Americans trying to settle the flatlands west of the river. From 1815 to 1825, it was difficult for people to really make themselves at home in Chicago. The only homes that then existed were rugged wilderness like dwellings, with a small area set up for farming and raising animals. Meats were still hunted down. Wilderness was still abundant. More settlers were slowly making their way westward towards more southern areas, occupying them enough to serve as some sort of security perhaps for the few living to the north or northwest. But for a Chicago to exist then as we know it today certainly was not the case. Chicago life was still primitive, or as Benjamin Rush might say, in the second stage of life, the post-pioneer, early farmer’s stage.
[]
So what diseases happened as more people began to settle Chicago in the 1820s and 1830s. We now had for the first time an opportunity for the latrines to begin to take their toll on us. Diarrhea would prevail and then dysentery if we weren’t careful about our living habits and hygiene. This is exactly what happened to the residents of the now former grasslands, onion rich meadows on the western shores of the lake. The miasma still formed through the area, and the cold airs and hot, humid temperate to tropical winds at times coming in from the southeast to the northeast depending upon the time of the year. The worst fevers still came in the autumn and during the mid-winter, a time when rodentia made it possible for certain pests to infect households like fleas and other vermins. Typhus struck in the mid-winter, spring and summer perhaps late in each of these congruent seasons. Between were the catarrh (cold) of the coldest periods, the influenza of the coldest, most ornary windy times of the winter, and the summer fever event when any of the others were getting in our way of progress. The diarrhea was mild most of the year, but on occasion more dysenteric or cholera like in nature, but still not deadly, like the cholera morbus (severe opportunistic dysentery, not Asiatic cholera), or even worse the cholera asiaticus. Fever and diarrhea were mainstays for much of the year when it came to isolated and periodical endemic illness. But other illnesses abound as well, like the Indians feared. Measles and Small Pox made their way into these regions a well, but especially during travel seasons and travel periods when the night time temperatures were too low and conducive to crowding any inside sleeping quarters whenever guests arrived.
This was the disease and medicine history of Rush’s Stage 2 that this region was in. Because it was Stage 2, we also had livestock to contend with, and unknowing for the time, specific diseases harbored by those animals. The place was not crowded, so milk or purpural fever was not that frequent. But milk sickness could be and probably was whenever the hay was lacking and cattle were forced to eat upon weeds naturally growing elsewhere. Cattle born of supported insects like mosquitoes, lie, ticks made it more possible for other disease to make their way into the local families. The cattle sickness later called anthrax was possible. But during this time, there were cattle born diseases making their way up north from Texas and the like. On several occasions the cattle plagues of Moses’ era made their way into the region. Cattle died, suffering from diseases that didn’t dissipate until it was wintertime once again. Othere diseases we rarely hear about today were frequent back then, the green nailbed infection whitlow’s tumor was abound, and very common to this farming setting. The skin rashes induced by contact with nettles and poison ivy were common, although n one knew where the latter one could be coming from. Stage 2 settlements had more frequent rabies that others, this hydrophobia more prevalent around and within water rich areas.
By 1840, Chicago was a town. Over the next few years it grew at such a rate that this town underwent the physiographic and population based changes to become what Rush referred to as a Stage 3 region. Its farmers were more business savvy and advanced, and entrepreneurial in nature, opting to invest more and more rapidly as time progresses. The waters and flatland nature of the region was still a threat to the local health. The winds could still bring the miasma in. The waters were still capable of becoming miasma-breeding settings rich if effluvium and rotting mud, vegetation and animal matters. The earlier forms of fever and diarrhea remained, and newer ones were added. The typhus was now more popular than ever (actually it was true typhoid than true typhus later. but not yet differentiated). Measles and the pox were still an issue, although domestic habits helped to support the vaccination programs now in place. Whereas what was once called Cynanche Tonsillaris (diphtheria) was still around, it was not a prevalent as before (the vaccination being developed for it was still 5 or 10 years away).
But most importantly, Chicago was now more like a city. Crowded neighborhoods and closely compact living spaces were being established. Rich and poor communities were well defined. The influx of Irish and Germans led to the development of less costly living places, where new neighborhoods were established at times in the least healthiest of places. New industries were now also possible. Factory work and factory workers for example formed an important urban manpower source. The cowboys of rural settings to the south were replaced by the slaughterhouse herders who herded hundreds to thousands of heads of cattle per day to their death. The poorest of the poor were always those working the least cleanliest of settings. Urban people serving the other end of the farming and livestock industries was a disadvantage in itself to becoming the first erysipelas victims. What were living animals when they came to Chicago, were foodstuffs that were packaged processed, sold and/or shipped once they left the warehouse setting.
In the earliest years, livestock came in, were slaughtered, butchered, and then either brined, smoked or kept on ice for sale locally. Only a limited amount of these goods were well prepared and treated enough to be shipped far away from the region. Between 1856 and 1864, this commercial enterprise with beef grew at a phenomenal rate. There was no way of preventing the growing popularity of western Illinois down to Texas grown slaughtered beef shipped out of Chicago to the center of this nation’s largest city.
This image of the Chicago meat market was probably well beyond what Benjamin Rush had imagined when he defined his Stage 3 setting. Rush was still imagining man to be pastoral in nature, not the slave driving, industrial worker specialized in foods not nature’s goods. A change in the urban setting that Rush had imagined was about to commence well beyond his preconceptions of man would become.
Rush gave his famous speech in 1787, a time when urbanization was advanced, buts its technology not always that progressive. During this time we used up our natural resources at record pace. We burned wood like it was felled daily from our back yard. We needed sheep and flax farms to make most of our most basic clothes. Cotton was beginning to be a hit. Hemp still favored over silk due to economics, availability and prices.
Fifty years later, 1847 in Philadelphia near where Rush resided, or in the midwestern young city of Chicago, these natural resources industries were quite different. Wood and coal were perfected means for staying warm and powering up the local industrial settings. Steam power was frequently used. Trains were invented and had just made their way into the core of the midwest a couple of years earlier. So new types of industries could be developed in Chicago, and they were. The problem was, the clear delineation that we have today between what constitutes farming technology and industry versus mechanical industries were not so clearly defined. Thus the corrals of the midwest were replaced by the _________ of Chicago, a landuse and form that it is very well known for, even today.
Chicago could effectively urbanize a part of the farming industry that was too large and of the wrong discipline for farmers to manage, but not too small for industrial urban edge settings. Thus the ________ was born, a use and place quite different from the corral.
By the 1860s, the city of New York was no long a countryside. There was little grass, hay or flax growing in the heart of the city. Any domestic bovine in the heart of such a setting was most likely not there to be in a pet or placed in a zoo, i was there to be slaughtered and butchered. Between 1850 and 1860, this is what farming became in New York. In Chicago, it was this rapid growth of a city that made it the unsafe, highly infectious haven that it began.
.
The first story is about Chicago itself, and how the city came to be. Chicago grew
so rapidly between 1830 and 1860 that diseases like erysipelas were inevitable. Brought on by exceptionally poor sanitation, diseases like erysipelas required a spread by both the environment and the people. The densely packed living spaces of Chicago due to its rate of growth made such diseases seem inevitable. The development of a new industry just outside the urban setting, the combined stockyards, slaughterhous and warehouse settings made diseases like erysipelas due to Streptococcus pyogenes or beta-hemolytic group A streptococci inevitable.
The second story for this page, and of course the reason for this work, is how disease mapping was used to understand the cause and nature of the disease. A few years later, this value of mapping public health became clear when Chicago was struck by another completely different disaster–the 1871 Great Chicago Fire. The Great Chicago Fire burned down almost the entire city, a direct result of the crowding and poor sanitation typical of this fairly young urban setting.
The Great Chicago Fire symbolizes the sterilization needed for this city to start anew with redecorating its landscape. But it two led to the development perhaps of still two more diseases characteristic of this region. A condition commonly known as “Chicago Illness” infected this region due to a local Leptospiridiosis. The rebuilding of homes in Chicago also included the design of homes based upon new beliefs for the time–the notion that sanitation was very important, and so, as a result of this public health concern, the use of lead paints became population as a form of ensuring a sanitary home living environment in the form of whitewashed walls.
When we look back on the history of these four diseases in Chicago, we find it is no geographic coincidence to the fact that the maps of these four health conditions overlap so significantly with each other. This temporal change in disease very much demonstrates the way in which sequent occupany related views of disease patterns can help to define a new way to review spatial epidemiological patterns.
Such is what the new page is about on this site . . . .
.
Introduction
There are many ways that a disease can be spread through a region. For the Chicago region, the typical events in nature we blamed diseases on when we didn’t know its cause were mostly environmental in nature. The early 19th century philosophy was that we “caught cold” by exposing ourselves too much to the local air and temperatures. The likelihood for “catching cold” could be worsened by natural events, such as the strength of the wind blowing or the direction from which it is coming. Whether or not that wind was dry or humid was also a determining factor of how sick we become.
How we react to this environmental cause for illness is also a factor that determines our fate with the wind. By wearing the right cloths, closing the windows of our house, having the right amount of sunlight and artificial heating, we can stem some of the impacts of the environment upon our highly susceptible flesh. How we exercise, where we walk or ride our horse, how we control the air that we breathe in during our stroll to and through a park, and how we make our way through neighborhood on horseback in terms of breathing the air from a putrid swamp are all ways that we can influence our fate with health. Where we work, residing next to a butchery or tanning company exposing you daily to the smell of rotting, decaying flesh and chemicals, placing our outhouse next to another company’s leftover foodstuffs such as rotting cabbage and fishbones, are all ways to make for an even more disease prone setting.
Disease has a habit of not only following people, but also of being a part of the local environment and ecosystem. Some diseases are people bred and born, meaning they can only exist where people are or because people are there–two very different things. Other diseases are truly environmental in nature, and are due to organisms that exist in the vicinity regardless of whether or not there are people there. Somewhere between these two extremes is where most of the diseases lie. Environment and ecology play a role in how we become sick and why some of us are more susceptible than others, but being exposed and becoming sick are two different events. What it is that we expose ourselves to is for the most part the environmental experience needed to make us ill.
For Chicago we can add to this the results of its decades of growth. The filth associated with man’s way of dwelling in cities is what did Chicago in once its population began to rapidly grow. In the city setting there was the problem of crowding that takes place. In the rural setting, the building are less of an influence, and nature takes over.
It was the narrow alleys between recently raised buildings and the rubbish filling them along with nearby shanties that made susceptible to housing vermin and becoming incinerators for the inevitable. Between 1830 and 1850, Chicago developed its maze of streets and buildings offered refuge to people, vermin and pests alike. But it also became the perfect chamber for putrefaction to commence one people became filthy and the normally healthy increasingly ill. By 1855, Chicago was just waiting for a new disease due to poor sanitation. It was no longer the suffering due to the cold, the pox, measles and numerous fevers that they had to contend with. New industries were being developed and with these industries came more disease reservoirs taking the form of cattle.
In 1857, when the beef industry took its first step towards industrialization in a big way for the city, such a chance came and St. Anthony’s Fire or erysipelas struck the city.
When St. Anthony’s Fire was over, there was a subsequent query to how and why it happened. This took place long enough for the findings to be published in 1867. Dr. Robert C. Hamill was the physician who led this query.
Trained in medicine when it was just taught as a short 2 or 3 month program, he had adapted and expanded his skills over the years. At the time he was learning this field, epidemiology never fully existed. Medicine was more a series of different beliefs systems and people engaged in trying to determine why diseases existed. There were the climatologists that believed weather was the main cause for illness, the leading belief for disease ever since pathos was first understood by Hippocrates and all whom followed. There were also topographers who believed the landscape defined certain disease ridden regions and the types of diseases they had. They claimed that illness erupted whenever we could fully protect ourselves from and adapt to the local environment at hand. There were the animalcules theorists in the early 1800s as well, individual who believed the smallest of organism could be making us ill. Their precedents were the worm theories of the late 1700s and very early 1800s. They had since perfected this philosophy of theirs, and found numerous examples of diseases proving they could be right. Finally, there were all these unique metaphysicians who believed in the forces of nature as causes for disease, forces such as sunlight and heat, galvanism and electricity, the earth’s magnetic field and the passing of comets or striking of meteors onto the earth’s surface. Their interpretation of disease as a result of the cosmos was the reason the notion of virus remained a popular belief, and why mankind in general has never completely turned away from the nature of energy and the universe as the reason we sometimes become ill.
In 1847, one of the best example of these philosophies merged into a single system came about when German disease geographer Canstatt published his treatise on this topic. His classification system, mentioned several times before in my writings, puts all of these hypotheses together to form a single theory with its blending of ideologies for the reasons pathogens exist.
The British counterpart to Canstatt’s training was being developed by William Farr. Farr’s teachings included confirmations of Canstatt and other German medical geographer, but also included a new focus on sanitation and the disease factor known as zyme, the science of which was termed zymotics.
Hamill’s training and further development of his understanding of disease took place from about 1825 to 1850, In 185___ he was awarded his second M.D. degree, this time from the medical school in Chicago ______. The new degree was more a reward for what he had already accomplished in the field in general than it was a sign of his return to any classrooms. It was enough of a validation of his skills to secure him a position as Sanitation Officer for the city Chicago area by the late 1850s, just as the beef industry was maturing and the stockyards were becoming well established.
When he began this position, Hamill had been through the teachings of the time, by those who strongly believed in viruses (very minute air born objects) and toxins as causes for certain diseases, as well as topography and its impacts on the miasma. Hamill also believed in the teachings of east coast sanitation experts and soon became as a strong believer as well in the sanitation theory for disease and the environmental theory being professed. Applying this to a Chicago setting, it would not be a surprise if Hamill blames such common events ans the influenza and “colds” on the lake winds and temperatures and the layout of the local land. Other diseases erupting more inland and out of reach of the immediate lake winds he would have blamed on weather and climate once again, but also the crowded living conditions.
When erysipelas hit the city, the only thing new and different for Chicago the millions of pounds of beef making their way into the stockyards. By mapping the disease, Hamill’s goal was to determine if the disease was linked to the slaughterhouses, or to the environment around the Great Lakes.
[]
If we look at the map depicting the spread of Erysipelas throughout the City of Chicago, we see this fair amount of overlap, enough to convince us that the two events are somehow related, but not fully.
Such an observation, making use the shared space for two events to suspect that they may be somehow linked to the same causes, is based on the ecological theory. The ecological theory in public health statistics claims that two events or observations are somehow linked to each other when they seem to demonstrate considerable overlap with each other.
.
The Errors
If we are right with this way of interpreting things, we have therefore learned something by relating the two to each other. Normally, these relationships are made based solely upon numbers, using some form of associative statistical method for analysis such as a correlation, covariance, nearest neighbor measurement, etc. With the map, we make space another aspect to be measures and use to link the two events together. This forms the basis of the use of geographical information systems to design you studies and hypothesis in health today, based on theories and hypothesis being realized for the first time 150 years ago or more when physicians like Seaman, Snow, Farr, Lea, Hamill, and hundreds of others, mapped disease for the first time with the goal of seeing its cause laid before us, as plain as the content of a Renaissance or French Impressionist painting.
If we are wrong with making such an inference due to the use of maps, we have committed one of the most common errors produced in epidemiological work–an ecological error in which we state that the associations between two events, mathematically, are related to each other, when in fact they are not–a Type 2 error at is best for those who are traditionalists.
What made Erysipelas spread from the southwest to northeastern sections of Chicago in 1863 is the same thing that made the Chicago Fire spread from the northern districts southward and across into the western districts in 1871. Buildings and people were too densely packed together, with the alleys between them cluttered with garbage and debris. Be the cause for illness a bacterium like that for Erysipelas trying to spread from people to people, or the intense heat and burning ash from the Great Fire trying to spread from alley to alley, rooftop to rooftop, the paths for each of these ecological terrors were much the same. St. Anthony’s Fire and the Great Chicago Fire each visited the city of Chicago in much the same way.
Erysipelas came by way of rotten flesh and spilled blood littering the ground, water and people residing around the diseased area. The wooden boxes, crates and shanties filling the alleyways made for good feeder fuel for the fires. Both of these problems existed due to the poor political infrastructure and the rapid growth of a population outpacing the local sanitation and public health movements needed to keep the city of Chicago healthy.
The great blame once laid upon O’Leary’s cow was as much a cause for the Erysipelas epidemic as it was for the Great Fire. The filth and contamination of a slaughterhouse gave St. Anthony’s Fire the key to this city. The filth and piling of garbage in alleys between wooden buildings gave the Great Chicago Fire the route it needed to retrace that route in an opposing direction.
What is unique about this review of spatial disease patterns is it illustrates how sometimes a non-sequiter series of events can providing additional clues that become quite valuable in the research. In traditional epidemiological statistics, there are several very frequent outcomes that are produced. The first is a type I error in which an association made between two events is in fact in error. The second is when the researcher concludes there is no association between two events when in fact there should have been one. Finally, there is this kind of fallacy called an ecological fallacy or error, which is when we say two things are related, and show them to be related spatially due to coincidental occurrence spatially, when in fact it is very unlikely the two are in fact associated.
This latter error is the most frequent error generated in modern day studies. Everytime there is a news story that suggests two things are related medically, implying statistical support for this claim, we have to wonder if the association is really true, or is it an ecological fallacy. For example, it makes common sense to say motorcycle-riding is somehow associated with good health. But if in the same study we find that bike-riders are more like to smoke, there is the added association that bike-riding is unhealthy. If in turn we also find that these bike-riders are more apt to have a criminal record and/or engage in violence, it would be an ecological fallacy to suggest that bike-riding causes illegal behavior, or that bike-riding causes smoking, or that smoking causes violent behaviors. None of these relationships are true. They all have to be sharing something else that makes these associations possible, such as income level, upbringing or cultural background.
Medical GIS adds place or space to the analyses being performed and uses place to imply one of two things–either a natural ecological and environmental cause for the relationship, or a human ecology or population behavior and density related association. Sometimes we can try to correlate the natural science perspective with the demographic or human perspective to see how and why the two seem to correlate, spatially and statistically.
The study of the human disease erysipelas has primarily a human component to it that focuses mostly on human ecology. But these human ecological features also relate to the physical make up of the urban environment the people are living in, and so this piece of the epidemic picture relates to how it develops and behaves spatially, and as a result nearly mimics the behavior of the human disease pattern erysipelas. The Great Chicago Fire spatial behavior and the Erysipelas epidemic behavior are so much alike due to an ecological relationship, that replaces the ecological fallacy we might otherwise deduce.
One event did not cause the other, which might be a logical ecological fallacy deduction made with this type of study. But the two events occurred in similar settings, for similar or related reasons, and the spatial and temporal differences each of these two events displayed do reveal to us additional evidence as to how the two did happen for many of the same reasons. The pattern of spread of erysipelas versus the great fire had but a few differences that explain why they diffused throughout the urban regions differently. Wind helped the fire makes it ways through the region, water and people enabled erysipelas to spread through the city. The fire was started by a human behavioral event, not a domestic animal cause. It was spread due to human living patterns, not just due to the winds. Erysipelas was started due to a lack of knowledge of major sanitation concerns and issues, and the rapid, massive growth of a new technology and occupation in the Chicago setting that was not meant to be performed, nor safe to perform, in such a densely populated setting. Both were natural consequences f this unhealthy human ecological setting, one ecologically and biologically (microbiologically) induced, the other physically or physiographically (building density and opportunity) induced.
It ends up that the 1862 Erysipelas epidemic and the Great Chicago Fire of 1871 have some things in common. They are both pubic health events that took place due to poor management of the local public health, and the misdirected focus of disease as a consequence mostly of the environment. Surveillance activities during this time were in their last years of suspected wind and weather to be an environmental cause for many disease patterns. Nutritional illnesses like goiter and beri beri were still misunderstood. Fevers were different because people and places were different, not because their causes were greatly different. Health features like longevity, stamina, and intellect were all pretty much heredity linked. How we responded to the environment was predefined by our family’s history and our personal history of exposure to our surrounding living and settings. For those who moved to the windy city of Chicago, survival was defined by lineage and the abilities to cope and adapt.
whenever and where ever massive urbanization was happening. As a result of the the development of this large city came densely packed neighborhoods and very large business establishments. Because Chicago was quickly becoming the important connection between east coast and midwest commerce, the rapid growth in transportation services by land and water made it possible for disease to spread more quickly from one part of the country to the next. Due to its density, the spread of disease within the urban setting made it possible for epidemics to happen because of human population features, not natural ecological features.
[]
.
Such observations in conjunction with weather and wind records kept for the Chicago area by public health inspectors and physicians familiar with this epidemiological surveillance record, would have realized that the causes for many diseases weren’t as simple as laying the blame on winds from the southwest, or northeast, or the water flowing upstream versus downstream along the Chicago River’s south and north forks.
Without any other cause for disease to focus upon, physicians focused only on people as the cause for the new form of erysipelas striking their city. It was no long a simple case of poor hygiene following a surgery or two of soldiers at the nearby fort that was causing the disease to erupt. Unlike to post-surgical infections infrequent to the military individuals being operated within the fort setting, this version of St. Anthony’s Fire was not at all selective in who it infected, and infected anyone, any home, and any neighborhood in its way as it made its way through the Chicago City.
Chicago’s two Great Fires
When the Great Chicago Fire hit, we can imagine it to be a cleaning or sanitizing of the city of Chicago long overdue. Due to its continued growth from 1850 to 1860, Chicago was quickly becoming the home of many diseases. In its earliest years it housed those common northern latitude, lakeside or shoreline diseases like the fevers, dysentery, influenza and “the cold.”
Ultimately became the main thoroughfare for many diseases still making their way into this country today, all due to urbanization and the underlying sequent occupancy related changes in disease patterns that ensued.
During the 1850s, it was nearly impossible for local governments to keep up with the building of new homes and boarding houses in Chicago. There were massive changes in land use taking place on almost every day of the year, producing what would soon become a future city . The 1850s was also a time when the poor and rich were more steadily growing apart from each other, turning the poorest of the poor into the most susceptible reservoirs for epidemic diseases, and making the richest of the rich even richer and more apathetic to the needs of the poor.
In sequent occupancy terms, we can view Chicago as a progressive industrial setting with combined, overly productive farming, ranching, slaughterhouse factor and warehouse settings. Pig stys and corrals were older names given to the massive _____ and slaughterhouses now being use along the south fork of the Chicago River. Silos filled with grain and compost heaps filled with excellent tilling manure were byproducts of this big business that was booming in the periurban setting. This made it such that in one section of the city we could have fourth and fifth generation homes alongside high level farm and livestock factory settings.
Whittlesey’s Sequent Occupancy theory can be used to defined the following economics and medical history for the Chicago region.
…
The evidence for this rapid growth of Chicago’s version of the “farm” is found in the commercial data. By 1859, the first hogs and cattle more than just occupied nearby stockyards and warehouses, they filled them to the brim turning Chicago into the main providers of western produced steaks, ham and meats for the rich families residing back east. The following report details just how many heads made their way into the limited stockyards and warehouse buildings in Chicago, along with how many steaks, hind quarters and pounds of fat and smoked leftovers they produced for the marketplace. From this table we can see that in just four years, the production of Chicago meat products increased to more than six times the original amount.

By 1859, the industry was pulling in more than 110,000 full grown hogs and 32,500 heads of fat cattle ready for slaughter. If we assumed the season for this industry to be 6 months in length in 1859, that meant there were nearly 20,000 hogs and 5,040 cattle per month on the average. Of course, these are just averages. Chances are that if we assume a May to October season, July, August and September are more than likely the peak months, with the most blood congealed and left to lie the longest by September to October, and the most fermentation and incubation of bacterial in and around the entrails taking place in August and September. October was your sickest time, the aromas the most pungent. September and late August were nothing to feel successful about however, the smell then was crisper and more highly resolved. As a doctor’s point of view, your sickness varied over time from these volatile mass produced stores. Disease might even vary as these smells tended to ripen over time.
But the worst of time in theological tradition are the plague months. And in recent decades, the worst months have been those late fall ,early winter times, like October to February, when you are trapped within you humble abode for much of the time, barely able to maintain your own self-defined quarantine like behaviors, trying to avoid getting sick from others in the house or making others sick whenever you are. The worst events happened these months, and it was the center of this time frame that the erysipelas took its largest tolls on the Chicago residents. With the winter months beginning, the grounds were not cold enough to suppress whatever might be causing the epidemic. Enough time had elapsed for the disease to make its way across the floodplains into new well water settings, as a miasma riding the underground currents. In the form of cadaver parts made its way down the river, replanting itself along the shores, so as to rot some more in the sun once it hit shoreline. In the form of long-brewing, fermented matter giving way to animalcules or viruses (both then believed in for the time as causes), it could finding be the chamber pot that once somebody made contact with at work, at its latrines, and the latrines nearby or next door, that the last contagion passed on by the last sick person in the crowd, also managed to find its way to you, and make you now filthy and infected. Again, this is how the doctors reasoned this wintertime epidemic out.
This lucrative start for a hybridized rural-urban livestock industry pulled in high values for its meats, at a cost that more than doubled over the next year for hogs, and nearly tripled for beef.
In 1861, as the war began, the price of meat had risen another 20% each, resulting in more than 400,000 heads of livestock making their way to the marketplace. This represented a rate of more than 50,000 per month for eight months, 1650 heads per day of both hogs and cattle. The stockyards, slaughterhouses, warehouses, refrigerated or brine-pickling settings were the most productive in the world by now. Even on a bad day, when these properties covered by decaying compost and excrement could be cleaned for once in a long while, several dozen heads made their way past the slaughterers and subsequent butchers. On a good day, the blood of about 150 to 200 cattle being slaughtered flooded the surface of the grounds, per hour. As a consequence, the water of the southfork river often flowed red, like the plague of Egypt’s Nile searching for its next victims.
So why did erysipelas strike Chicago the way it did in 1863? And what does it have to do with the fire that consume this city eight years later?
A Contemporary Diagnosis
It helps to understand exactly what “erysipelas” was back then.
During the 1850s, erysipelas was a disease that produced a reddening of the skin as its chief symptom. Such a symptom could be due to any of a number of problems for the time.
Ergotism was the main example of this form of epidemic, erysipelas another. For each, there was this sense of burning and fire upon the skin. Physicians and scientists knew little about the existence of the two different causes for these two different diseases, and so sometimes had a problem distinguishing between the two without the adequate experience.
Did the doctors in Chicago know about these two forms of the symptom known as St. Anthony’s Fire?

The traditional cause for St. Anthony’s Fire during the century before was wheat contaminated by black grains filled with the fungus ergot. Chicago was a major hub for both crops and meat. Thus the likelihood that fungal infested rye made its way into the silos of this city was there, although not likely.
The major findings that rule out ergot-contaminated wheat was that such a contamination would have been sold by local markets and would probably have been more universal in nature. The disease that struck Chicago, according to Hamill’s map, did not follow the major transportation routes through Chicago so much as it followed the ecology and topography of the river passing through this region, mostly along the south fork. Large portions of the commercial routes along which contaminated flour and grains could have traveled remain untouched, both store to store and house to house.
In addition, flour or grains contaminated with this flour could have also been a major product shipped out of the region. But ergotism did not erupt in nearby cities and towns where Chicago’s products might have been sold. So, grain products probably never caused the epidemic that struck Chicago in 1862., which means that the Chicago version of St. Anthony’s Fire had another cause.
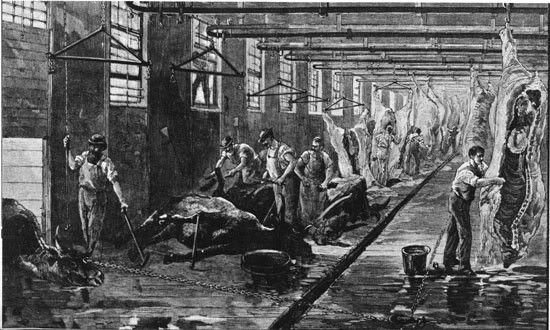
A Slaughterhouse (source).
Imagine 2500 of these per day, more during the peak weeks of a season during the hottest months of late summer. How much blood, entrails and skeletal remains are left behind?
The other cause for this disease was rotting spoilage and blood left over from animal carcasses. Piles of rotting, decaying entrails, spines and rib cages, gallons of blood draining from the floors of slaughterhouses into the culverts below were the source for this epidemic. This source of the disease for the time went from the slaughterhouse downhill and through the culverts into the local Chicago River. Fro there it spread downstream and ultimately made its way into the local underground water supplies and into the city households relying upon well water. In addition, contaminated workers whose hands, clothing and personal belongings were covered with hordes of the effluvium or work/sweat-generated “miasm” could have easily brought the disease back to their home every night. Thus started the migration of erysipelas into the heart of the city of Chicago, and from there elsewhere throughout the local metropolis.
Hamill may have not envisioned this flow pattern for the disease at first. Instead, he and others in the professions were still contending with philosophies left over from generations passed. The older miasma disease was still popular, modified somewhat in terms of the form of this deadly substance, but still with a typical behavior within certain local environmental settings. Another philosophy now popular as well, William Farr’s Zymotic Theory, had many diseases separated into distinct, new categories. Those which had some form of vaccination process related to their control were separate out from the rest.
The location of Erysipelas in this paradigm is uncertain. But since the disease was remaining local, according to Hamill’s observations it must have had a very distinct topographic and demographic pattern. In retrospect, we can conclude from his map that it had to be a surface and water bound condition. But to Hamill it could still be an airborn pattern.

Contemporary images of Chicago, demonstrating the appearance of miasma rolling in from the waterfront, and a garbage-packed alley
.
Sequent Occupance – the History of a Nidus
.

One of the slaughterhouses was recently converted to a hydroponics setting for leafy salad greens and an aquaculture setting for tilapia (see Noah Plaue. An Old Chicago Slaughterhouse Transforms Into A Futuristic Vertical Farm. Business Insider).
.
Today, the following physical, cultural, social and ecological illnesses have their peaks in the Chicago region due to this unique history.
The Chicago Illness is a disease brought on by a fungus that is apparently well adapted to the Chicago setting. Like the climatically and ecologically defined clusters of Cryptosporidium in and around the neotropical latitudes of southern California, the organism responsible for Chicago Illness does show a tendency to gather mostly in its urban setting.

We expect the perilacustrian nature of the Chicago setting and its flat topography to also have influences upon some other basic human diseases such as colds and flus.
The human related parts of Chicago’s public health however can at times seem quite controversial and make us wonder about how effective are the current health care, public health, epidemiological, disease surveillance, antibioterrorist, and homeland security systems.
Chicago has large amounts of child abuse taking place in its various forms.
Just across the Great Lake, Detroit, is the poorest city in the U.S., with the greatest financial industry outside of bank operations employing but a few of the residents, and with the greatest amount of poverty and unoccupied dwelling. It recently became the first to declare bankruptcy. Is there something to the climate, health and human behavior that could be in play here?
In the hotter months of the year, the older population’s health is at risk due to hot spells and urban living conditions akin to trying to survive in an old fashioned apartment, metal housetrailer, station wagon, or toaster oven. (Recall the great heat wave of the early 1990s at such a northern latitude setting).
Hieronymus Bosch. To the left is the St. Anthony’s Fire that struck the city. This particular form of fire-bound epidemic flying over the city like a mal aria or miasm was ergotism.
Hamill’s 1867 Interpretation
At the time of his writing, there were only two major sets theories out there that Hamill could consider–the miasma theory group and the sanitation movement philosophy.
First, there was that ever elusive environmental theory for disease which blamed everything on the environment and its “miasma.” In the 1847 rendering of miasmic diseases by German medical geographer Canstatt, we find that the term miasma had been modified so much that magnetism, electricity, heat, meteor and comet patterns, weather, temperature, humidity, gases, the smell emitted by corpses, could all be considered form of this theoretical substance. The miasm responsible for illness was no longer the simple swamp gas, odor emitted by gangrenous flesh, or smell of rotting seaweed and fish.
For Chicago, miasma could be related to this latitude and longitude or place in the magnetic orb surrounding earth, or it could be a form of electricity generated by the atmosphere and intense storms that occasionally developed, of the electricity that made so many people ill could have been emitted from lakes and rivers, in the form of mist and humidity, made worse by local temperature and humidity. There was also the crowding of the area by people and their debris and waste. Canstatt’s miasma could be formed by human waste, poorly draining septic lines, of sepsis floating about the local river banks, and weak, ailing bodies emitting the odors of a sick person, an effluvium capable of planting itself on people who visited, or whose windows were open just next door to the sick man’s place.
But Chicago was also a city that had closely-packed buildings and living quarters. The sanitary theory of disease in such regions was also quite popular. It became popular in the 1840s when living “dirty” was blamed for many diseases, mostly due to the living conditions of recent immigrants who brought diseases in from foreign countries or were in such a poor state that they became infected quite easily. When Cholera became an epidemic recurring every several years during the 1830s, late 1840s into the 1850s, they were quite susceptible. The third such epidemic that followed in the late 1850s epidemic, made many suspect that filth, poor hygiene and unclean water were its major causes. Hamill had this history to consider when defining his philosophy for the 1863 erysipelas outbreak.
But the miasma theory wasn’t the only proposal out there with considerable support. William Farr of Britain developed his own form of Canstatt’s miasm theory–the zymosis theory. This new term zymosis referred to “zyme”, a theoretical chemical form of disease yet to be identified in any details (kind of familiar? compare this ideology to phlogiston). In Farr’s hypothesis, there were diseases that could be immunized or fought against due to their miasma like entity, like those which could be vaccinated against. But there were also these diseases of uncertain etiology that had unique causes or “zymos”, yet to be determined.
Also floating about were the theories proposed for disease that were focused on the traditional poison or virus, which spoke about invisible stuff infecting us, and the notion of germs and animalcules, which pointed blame at the small, barely noticeable organisms dwelling within nearby waters, old foodstuffs, rotting flesh, decaying granulomatous body surfaces of farm animals and sometimes people.
A major difference between William Farr’s theory about the zymotics, and the simultaneously developed complex miasma theory by Canstatt, was that Canstatt allowed a more metaphysical interpretation of the cause to be considered. Such non-physical items as solar energy, magnetism, electricity, and universal forces were included in Canstatt’s set of hypotheses. Farr however paid less attention to the magnetism and electricity included in Canstatt’s work, focusing more on the zymos, his explanation for the undefinable events potentially creating illness.
Dr. Robert C. Hamill of Illinois learned medicine in 1838. The was the heart of the various climatic and physiographic theories for disease. The germ concept had been around for a while, though not at all defined as what this same term means today. The germ implied filth and poor sanitation, to which bad eating and living habits, poor cleaning and housework practices, bad exercise and work habits, drinking, gambling, and engaging in unethical, immoral forms of additional recreation were all considered ‘cofactors’ to help an illness turn from its milder form to the more aggressive, deadly form.
We can use some of today’s understanding of contagiousness and disease to better understand the opposing logic used back in the mid 1800s with disease patterns. If we assume for a moment that 20 people visit a relative lying in the bed at the local clinic or alms house one day, and that half leave the room and head home and never experience any episodes of illness related to that visit, whereas the other half a day or two later come down with matching symptoms and sooner or later wind up needing much the same care. The theory at the time was that whatever activities those taken ill participated in just before or after their visit caused the disease, such as drinking, participating in too much sports, or the church’s annual gathering one hot Sunday afternoon, or engaged in horse race gambling and staying out late an night. Those who did not become ill, remained health because they had a strong physique, constitution and heredity, and kept themselves, well rested, well fed, clean, and not too experimental with anything beyond the normal healthy living practices.
Today we would say that half got ill because they were of weak constitution, made contact in the wrong way, and did something to bring the disease into their body. The other half managed to avoid it out of luck, lack of contact, and/or aggressive strength, physique and immune defenses.
.
was trained mostly in the zymotic and sanitation theories of disease. He probably had a decent background as well in the older miasmic theory, even with some idea about the much older koino-miasmatic (natural elements producing miasma) and idiomiasmatic (people and rotting flesh causing miasma), but like so many Anglican doctors had limited exposure to Canstatt’s highly successful miasma theory promoted abroad in non-English speaking counties. Like Farr, he perhaps knew little about this because of the language barrier then existing, and the prejudice this country had again these other thinkers east and north of France and Spain.
Whatever the reason, when erysipelas struck Chicago, it was up to Hamill to decide which of these theories was most related to the erysipelas he was witnessing. Chances are the erysipelas came in one simple form prior to this outbreak, and as two very distinctly different forms once the epidemic ensued. Prior to this outbreak, the main form of erysipelas was a post-surgical infection usually linked to the work of the military surgeons performed at the nearby Fort. This could have been due to any of a number of bacterium according to current knowledge and philosophy, but back then no differentiation was possible based on an animalcule or bacterial cause. After the 1863 outbreak occurred, one was able to distinguish the traditional older forms of infection from this new erysipelas, which mostly infected the face and cheeks but occasionally took to the legs and feet.
Chicago’s Welcome for Hygeia
A Spatiotemporal Interpretation
When we look at Hamill’s map, we see he is tending towards some topographic disease theory. The area he defines as the epidemic region follows the south branch shorelines but stabilizes around the confluence of the two branches. If the erysipelas were purely wind born, brought in by the Lake winds, we’d see a similar pattern but with the richest areas close to the lake’s water edge. More over, it might be expected to be seen flowing north and south of where it came on shore. So being purely lake-born wasn’t an option for Hamill.
People-born is very much possible based upon Hamill’s map. We can see that if it began in and around the confluence, that this disease pattern could be dispersed along south fork the way it was, and if the winds are right and their seasonal pattern matching, this would most likely be his theory–the notion that this disease erupted in the center of the city, and spread from house to house due to traffic flow, people behaviors and winds.
[]
There was this coming together of different parts of the country as Chicago grew. What was once a city isolated from the cities back east, except for travel across the Great Lakes by large ships, or slowly in any direction by foot, or to the south and the Mississippi River by small shipping routes, became a city that was the hub of most of the nation’s commerce once the rails were established between 1850 and 1860. This meant that whatever microbe, fluke, intestinal worm, tick, flea, rodent, or whatever, that was is in search for a new home, would also have a new population of people to infect once it made its stay in Chicago. With the coming together of cattle from Iowa and hogs from the lower Mississippi, Fruit and Poultry from the northern states and Canada, it became possible for Chicago to feed much of the northern nation but also become the nest for all diseases wishes to make their way elsewhere into this country as stowaways in handbags, sleeper trains, cattle cars, and heaps products and rubbish loaded onto canal boats. The international commerce portion of Chicago’s history had just begun, meaning there were more diseases to be spread to this city by 1900. All of this began in 1860, when Chicago became the petri dish for bacterial diseases being bred by poor sanitation, poor personal hygiene, and the means which to make all the required steps happen in one place, where by 1862 it had turned the occasional erysipelas cases bred mostly by surgical practices into a disease that was epidemic in nature, uncontrollable and rapidly spreading.
The O’Leary barn was the place where the Great Chicago Fire began in 1871. It ends up this fire was due perhaps to human misbehaviors, although not necessarily those of Mrs. Leary. The fire happened due to old man “Pegleg” going out for a smoke one night and emptying his pipe of dropping his matches on the hay in the barn. This small ignition became the Great Fire about an hour later, and happened due to the same reason Erysipelas years before was able to become so deadly.
The City of Chicago had become unsanitary, very crowded, unrestricted in its growth, unrestricted in how we used its land, untamed when it came to such things as poor sanitation, crowded alleys, garbage ridden side streets, shanties and shacks filled with rubbish and people ready to ignite, ready to burn. There were limited public health concerns for the time, and a total lack of poverty control. With houses so close to each other, connected directly to each other by lines of man made kindling and tinder, the city was waiting for the right flames to strike, which happened in 1871 and burned much of the city down, a large portion of which had taken the lives of people just 8 years before due to erysipelas.
….
Interstingly, that same section of the city so utterly destroyed by this fire overlapped considerable with the epidemic region that struct this same town 9 years before. Thus the erysipelas epidemic was not really a valuable lesson to the people and their unhygienic living behaviors and the Great Chicago Fire became a lesson in the pitfalls of not properly planning you local population growth. Crowding makes it easy for a bacterial disease like Erysipelas to be passed from one household to the next. But crowded buildings and rubbish make for an easier transfer to take place from building to building of the original flames needed to start the right type of fire in this setting.
The irony to this fate was the fact that as a city, some of the people there opted to keep their farms running. You have a city consisting of cement, stone and brick, with wooden beams, plenty of fabric and wooden furniture ready to be torched, place right next door to ample stores of hay, dried cattle feed, and kerosene lanterns lighting the interior of these buildings when milking time arrives. This it was the abode of Mr. and Mrs. Patrick O’Leary that ended up burning the city down. The hybridization of farming and urban life was really not meant to be at the time it existed in the city of Chicago. Horse stalls and cattle barns had to be more watched and attended to, not due to the smell of manure as much as due to the closest of these breeding grounds for disease and other unhealthy things that some people perhaps wanted to remain distant from when they moved to such a fast growing city.
Once more than half of downtown Chicago was “utterly destroyed”, the opportunity was there for rebuilding the city, this time with better land use policies and actions against overcrowding in mind.
[NY Slaughterhouse Pictures]
One of the main consumers of Chicago meats at this time was New York City. New York City was able to learn from Chicago’s mistakes. New York also had a number of dairies and slaughterhouses placed deep in the heart of the city. But more importantly, New York had large several story floors for partaking in its slaughterhouse needs. Spilled blood drains downward no matter where you are when the steer get slaughtered. But for some reason, New Yorkers did not experience the slaughterhouse induced erysipelas epidemic like Chicago did. New York was crowded, with cavities of poor communities placed right behind some of the least healthiest industries for a city to have around this time. Yet New York had other issues to contend with, and so fortunately the large numbers of public health officers watching over New York City were able to prevent a lot of outbreaks from happening.
Both cities would remain high public health threats for years to come. Without knowing the causes for these diseases they were trying to prevent through improved sanitation practices, each of these cities got rid of two of the four causes for outbreaks like erysipelas. They diminished the sanitation problems, they redefined the water supplies a city would received, but they couldn’t remove the poverty and human behaviors required for many diseases to happen. And so today we still have cities like the 1860s and 1870s Chicago and New York today, filled with their unhealthy neighborhoods and places in need of ongoing public health inspection and preventive care. Just how much of this care they really receive can be told by how often the epidemics and outbreaks strike these urban settings.
/

A recent Slaughterhouse in Chicago (source)
.
…..
The epidemic was a consequence of the Great Chicago Stockade and Slaughterhouse industry which began in 1862. Until beef were added to this industry, the primary products were pork. With beef came a much larger industry and marketplace and the immense amount of slaughtering, which at times turned parts of the Chicago River red with animal blood. This very sanguine environment was a sign of the unhealthiness of the workplaces themselves. As people traveled daily to and from their homes and butcheries, this set the stage for the infection of the downtown city nearby. With the mechanics of the slaughterhouse industry and its conveyor belt like processing of livestock, carcasses, and meats to meet the needs back east perfected by 1863, the only thing stopping the industry itself would come to be–an epidemic that could be linked directly to such a disgusting scene in the public’s eyes. Accompanying the discolored waters of the river and its cess pool like shoreline eddies was the smell of decaying flesh, miasma to any old time thinkers about the environment and medicine.
Some of this water passed back under the street in the form of back-drainage induced by upwelling of the river water. Floods were the means for some epidemic related problems to make their way back up the cisterns that directed them out the city setting a day or two before. For this reason, whereas people living alongside the water were usually considered most susceptible to water-related diseases and humid air related problems like the fevers and diarrhea, whenever severe rains fell or the river water rose, causing it to flow back under the city, the opportunities for contamination of neighborhood well waters and tapwaters existed. Indoor water closets and privies were only good when the waste was your own in your personal closet of privy, once the neighbor’s waste and expulsions fed into your own water lines, you were now susceptible to whatever diseases the neighborhood had in store for you. As the local land became saturated with stores of human waste from various homes next door to each other, your family became the potential victim of someone a block or more away. Miasma had its way of getting to you, but need not have to travel the air to make your children sick.
In the world of medicine however, the physicians were slightly ahead of the masses in their thoughts about the eruptions of new diseases. There were still those who believed in the strong effects of climate, temperature, humidity, precipitation, winds and weather on the human body and its healthy state, but there was also a large movement in the field that incorporated beliefs about crowding, lack of hygiene, poor sanitation and the need for safe, healthy water into the people-rich environments associated with towns and cities. When the erysipelas commenced in Chicago in 1863, it was as much a consequence of the people and their lifestyle, their living patterns, as it was a consequence of the stockades and slaughterhouses situated just outside the city of Chicago.
Furthermore, the fire may have sanitized some of the bacterial ridden surfaces of the manmade topography and the podsol of the Chicago City terrain, but in the long run managed to only enabled the city to restructure itself and grow faster.
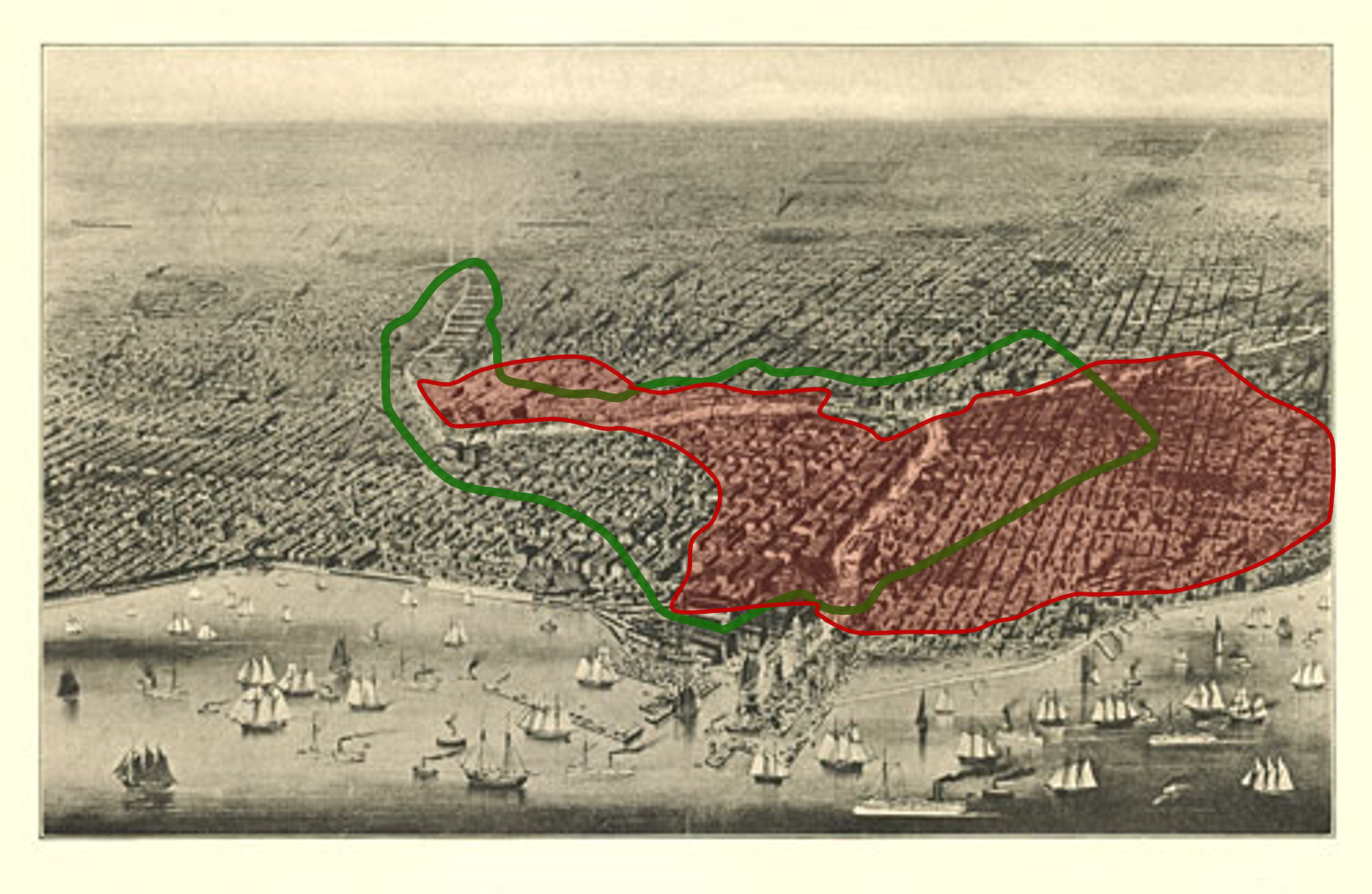
The 1863 Erysipelas Epidemic (green) versus the 1871 Chicago Fire (red) (approximated for each)
Once the erysipelas epidemic was over, there were still the makings of public health disasters in the Chicago urban setting waiting to happen. In 1871, the consequences of crowding and unhealthy living areas again impacted this city, this time by burning down much of the city. The Great Chicago Fire and the Erysipelas have these overlaps in distributions that demonstrate the consequences of rapid urban development that continued inadequately monitored or unchecked in terms of public safety and the likelihoods for disaster.
.
The geographic placement of Chicago on the edge of the Great Lake made it susceptible to diseases brought in by the lake and its windy weather patterns. In the first decades of Chicago’s existence as a city, the main interpretation was that its diseases were very much due to the environment, not its people. The fear of ships coming in from other regions, other countries, laden with goods contaminated by contagion picked up in some far away harbor or countryside was the greatest fear for the time. Otherwise, the only diseases one had to deal with in this fairly detached part of the United States were the endemic disease patterns typical of the Chicago region, such as intestinal worms, fevers, skin infections, and common colds and flus generated by the local ecology and environment.

The Development of Railways (in red) to the Midwest
In western New York, the Genessee Fever had eruptions as well as Lake Fever, both considered consequences of the topography and large water bodies in these regions. These regions served as examples of the health that the people of Chicago probably thought they would experience. When the trains began coming into Chicago first from the south and then the east, the geography of health for its region changed. Diseases from the south came into the region, and those from back east even more so due to the migration of people. The domestic animals that came with the farms that were established here had their own zoonotic conditions which Chicago would soon learn to deal with. The consequences of having you own milk and egg industry in close contact with the urban neighborhoods made it possible for still other illnesses to begin to develop.
Such an urban public health pattern was following the rules for such set decades earlier by Benjamin Rush. The early stages of sequent occupancy as Rush was defining these to be was taking place in the Chicago area. With the establishment of the Railroad industry and the laying of the tracks to Chicago, its rapid economic growth turned it into an industrial center, converting natural resources to metal and woodwares, and any large amounts of herded farm animals into factory produced quartered slabs of flesh and tens of thousands of cuts steak for shipping and sale to the more heavily occupied urban meccas back east. Organisms like Salmonella and Listeria were now having their say in the survivability of people so far out west. Until officials and engineers could learn to tame their urban settings that they watched grow and development, public health was little more an issue than the need for another ship to carry the city;s goods through the Great Lakes to back east. The focus was mainly on railroads and commerce, and very little about the health consequences of anything else in this region.
Changes in Chicago
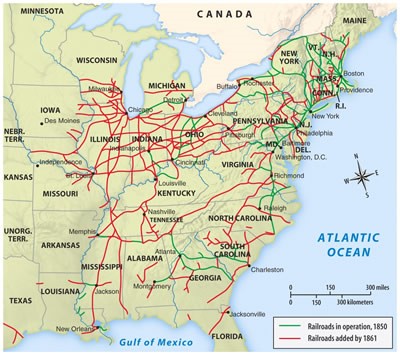
During the 1850s, the midwest developed into a large agricultural and livestock raising region. These products needed a way to be delivered to East Coast cities where they were in high demand. The development of this industry was possible due to the railroads being laid. This turned Chicago into a large financial success for investors, a fast growing city in need of new businesses, and a place for new immigrants to settle.
The beef industry in particular became an economic stronghold for Chicago due to its location on the map. In 1850, there were just a few trains heading to Chicago. All of this was changed in just five years, opening the doors for commerce between Chicago and the cities back east. By 1860, Chicago was the hub for commerce and travel in both directions.

Chicago served as the hub for western steers fresh up from the south and the large amounts of produce grown by local farms that were destined for other states and large cities.
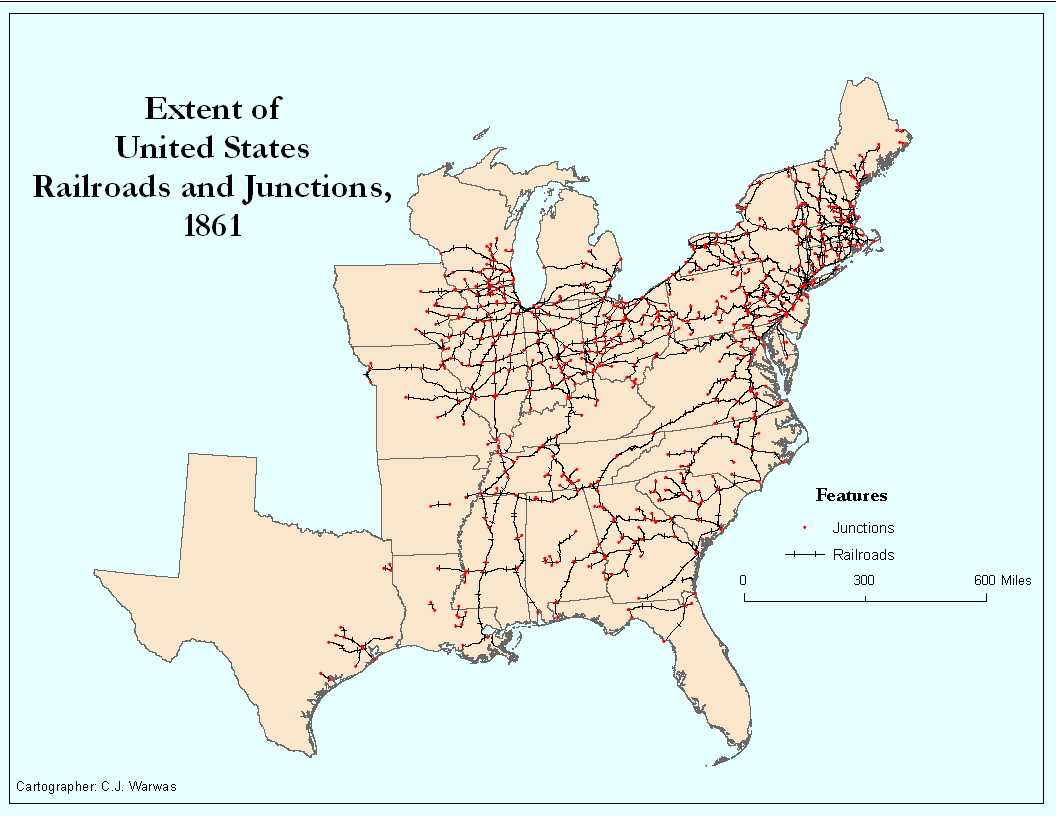
The Chicago route played a major role because the City of Chicago was still fairly underdeveloped in its outskirts. There was plenty of open space where stockyards, slaughterhouses and warehouses could be built, which, because they were so close to the city set the stage for the butcher industry to develop its first diseases.
Prior to this, erysipelas was a disease common with settings alongside infections like abscesses and gangrene. Much of the evidence for erysipelas striking the Chicago area was related to the military hospital established in the region. This hospital took care of many cases of gangrene and the like, and on occasion noted the erysipelas that often followed the operations. At the time, erysipelas was also primarily diagnosed based on its symptoms, the normal red streaking patterns that formed when infectious diseases in general set in, such as tetanus. So even during these earlier pre-epidemic years, the frequency of erysipelas as a public health issue not related to the beef industry is questionable, making its prior cases somewhat disputable.
Whatever the case, what was once a disease typical to small surgical settings, erysipelas became its own recognizable disease state that was different from other kinds of infectious diseases brought on by poor sanitation. The most remarkable symptoms of the erysipelas that developed in 1863 were the somatic and often facial signs of it affliction. Signs which a century earlier may have brought Biblical diseases like the plague to mind, were now not so capable of developing this mass hysteria or fears of G-d’s Vengeance. Doctors were experienced and educated enough to look for natural history and human related causes, not metaphysical causes.
Dr. Robert C. Hamill’s work and map show us how this disease came to be recognized as a product of people, not just nature. But Hamill is working at a time when he has to work through the possibilities of local environmental causes versus human related sanitation causes.
Hamill tries to show us that erysipelas could be a product of the great Chicago winds. Their chill and direction was very much a cause for other diseases like “the cold” and influenza. But the different spatial behavior and flow of erysipelas across the earth’s surface in and around the Chicago setting shows us how much we sometimes “humanize” or “subjectify” natural events, making them fit our theories or hypotheses in how we describe them and how we demonstrate them to other readers.
Erysipelas could have come into Chicago from the lakes, or from the inland flats west of the city. We brought it in it seemed by developing these slaughterhouses in a place where stench and blood filled the river and infected the city downstream a mile or two. But the fact is, population density alone helped to spread erysipelas into and throughout the heart of the city once it took hold of its first victims. Poor sanitation and the closeness of buildings made it possible for neighbors to turn this into an epidemic. We would never realize that this epidemic was simply a consequence of unhealthy crowded living conditions.
A few years later, the same crowded conditions led to the Great Chicago Fire, symbolically sterilizing much the same roads, streets, alleys and building where erysipelas once resided. The relationships between each of these two events and city crowding separately became important traits of any rapidly growing settlement in need of control and ongoing public inspection. Dr. Hamill’s role was as the inspector of this Great City, and his work on its disease patterns not only made erysipelas a disease of its own need for surveillance and review, but diseases in general in need of monitoring whenever and where ever a rapid change in population and land use patterns takes place as this nation develops.
We will see this effect of urbanization on public health repeat many times throughout the 19th century. Until physicians know the differences between similar disease patterns, and the different ecological and spatial patterns related to their outbreaks and causes, this uncertainty as to the reasons for epidemics will remain the focus of disease mappers. Together, the mapping of disease and its principle areas of outbreaks, and the focus more and more on knowing the exact cause for each disease, make for the sudden transition in disease mapping that surfaces soon after this event. The next stage in disease mapping is the production of small area maps, with a focus on land use, building placement, neighborhood layouts, placement of industries, water bodies, people, privies and garbage sites.
The 1870s was defined by the focus on producing sanitation maps, with the City of New York taking the lead in much of this form of disease mapping within the United States. Parts of London took control of the same skills in epidemiology back in Western Europe. By the end of that decade, the microbial theory prevailed, the immediate precursor to what we refer to as the bacterial theory for disease developed in the late 1880s.
During the 1890s, the value and meaning of medical maps changed to fit this new paradigm on the causes for disease. Those to which no cause could be assigned remained environmental and miasmatic in spatial distribution and dispersal patterns. Those with microscopically or chemically defined causes had specific places they came from or were developed due to. The types of maps that were developed also changed due to this interpretation of diseases. Hamill’s map is an example of one of the diffuse miasma like maps that was produced with the intent to match or infer a cause for disease. These same types of maps later would depict areas of infection and migration of the disease pattern, focused less upon cause and diffusion processes in the accompanying text. By the end of the 19th century, true causes for disease were found, these claims supported by the use of a map.

One of the Earliest Maps of the Chicago Area
.
Stages of Settlement
The history of the development of the Chicago area of Illinois is a nice sequent occupancy depicting story about diseases. Sequent occupancy theory states that events occur in sequence for each new, developing region. The original intent of this theory was to infer that there was some sort of predefined social evolution of people taking place where ever mankind moves to and opts to settle. But cultures are very different from one region to the next, so this absolute definition of how land uses would change due to occupation followed by growth remained very much an ethnocentric interpretation of how people behave with land.
Sequent Occupancy was also riddled with that problem of timing. Exactly when a place was first “settled” defined what the various statges of settlement were going to look like, what kinds of homes would be built, what kinds of transportation needs would develop, what kinds of natural resources would be sought out and removed from the environment. The settlement of a place in the 17th century is very different from the same for a century later, or two centuries later (1800s). Were a place to be discovered and settled for the first time in the late 1800s, or even the early 1900s, the settlement behaviors that ensued in some ways appear similar, but in so many other ways might seem to be quite different from each other. Whereas in the 1600s through to the early 1800s, the earliest settlements were traditional native American and early colonial wooden or bark-branch homestead like settings, in the late 1800s and early 1900s, the lack of traditional loghomes would be replaced by well planned buildings made from lumber and brick. Add another 50 or 75 years to this and some of your first homes may have had water, or kerosene lamps, or even electricity in some form. By the end of the 19th century, the decade of first development defined the technological roots of your place of stay, and in turn helped to define the safety and livability of these settings.
The ways the home were built were accompanied by changes and tends in workplace settings and occupations. The earliest years most certainly had a different set of living requirements and set of survival skills needed that would be different from later periods of time. Occupations changed due these changes in survival requirements. Foodways was also a fact of life that changes with time. The distance we travelled per day was modified due to changes in transportation. The kinds of clothes we wore and how we protected our self from the surrounding environment had its impacts upon our means for living and surviving.
Essential to good survival is good health, and this is how sequent occupancy can play a role in how we look at the progress of disease as a product of the progress in local and domestic development of lifestyle and occupations. Even though the sequent occupancy theory at times seems to narrow-minded, western society focused, or even ethnocentric at times, it does provide us with the method by which to look at disease patterns in a place, over space and over time, and to use this means for outlining disease studies, to better understand what took place in places early on in their history. Relatively speaking, the Chicago region developed so quickly during early United States history, and with sequent occupancy used to evaluate its growth and changes, we can make sense of what public health related events occurred in this region as time passed.
Chicago is a very nice area to learn sequent occupancy with, but not the sequenct occupancy of trade, traffic and lifestyles as much as the sequent occupancy disease patterns. This view of Chicago tells us much about the erysipelas that struck the Chicago area, as to what its cause was and why it occurred where and when it did in Chicago history.
Pre-Chicago
Throughout the 18th century, the area known today as Chicago was barely occupied. It was first settled by Native Americans and had a number of small communal settings raised there during the years. A small part of was inhabited or claimed as well by French pioneers, some of the earliest creole families perhaps, as well as missionaries, trappers, explorers, metis, Scots passing through on their way to the early trapping settle farther north. Practically every other culture possible for developed this region was there, except for the British.
Claims to this property back then were attempted by British and French leaders, but ultimately it was the United States that would win with this claim, when in 1787 the boundaries of the western territory were better defined.

It was about this time that a character known as Jean Baptiste Point du Sable resided here. Point du Sable, as he was commonly known, is described as an immigrant from Saint Marc, Haiti or perhaps Santo Domingo. Where ever he came from, he decided to live close to the Great Lakes area. It was here where he met and married a Potowatomie woman.
Due to the time he had spent in France years earlier he was educated. He was also fairly well off for someone living in the pioneer setting of what would later be called Chicago. He owned a large plot of land and upon it built a house. His house was followed by two barns, a horse run mill of sorts, a bakehouse, a poultry house, a dairy barn, and a smokehouse.
In 1783, this portion of North America had its borders redetermined as part of a discussion about land claims between the United States and Great Britain. The French surprisingly had minimal input into this discussion, even though French culture had dominated this region for quite some time and played a role in its heritage and now its fate as the English lay claim to the St. Lawrence-Great Lakes area. For a short while, the eastern Atlantic states tried to lay claim to this new region by extending the latitude lines in their original claims as far west as the Mississippi River. This made the region west of New York’s settlements, out by the Finger Lakes and Lake Erie, the first “Great Northwest.” One new industries began to take on the perception of the being the new Northwest United States, they enhanced their plans to establish markets out west and become the first commercial ventures in this unsettled region.
The first two decades of settlement in this area are what we expect, with Point du Sable residing there in what was pretty much a pioneer and wilderness setting, engaged in personal farming, some lumberjack duties, and in regular contact with the nearby fort. Much of the land out west was prairie land, but there were woodlands to the north in and around this part of the country. A region rich in woodlands meant that buildings could be constructed quite early.
Woodlands areas mixed with prairies lands, lakes, marshlands, and barren fields made for an environment easily converted to crop lands. But only a few parts of the Great Northwest seemed manageable as prairie home settings, those located mostly to the south. The Canadian border region bore large areas ridden with mixed evergreen deciduous forests. A fairly long, roundabout navigation route connected this heart of the Midwest with the south and eastern shoreline settings of the well established oceanside states. There were but very few ways to effectively cross over the vast lands, so plans for canals and railways to be built were made. Chicago was once a part of a long sinuous circular path passing through and around this part of the country. With increases in transportation, it came to serve as a pass-through for many long distance traveler. Once commercial lines arrived, it became the hub for much of the older parts of this country.
Earliest building in the Chicago area, according to most historians — the house of Jean Baptiste Point du Sable and wife
Chicago was one of the first major combined pioneer-Fort settings for the Great Northwest. Being adjacent to British owned lands to the north, it served to guard the lands to the south from being reclaimed by British Royalty. Fort Dearborn was built in this region to way off any problems that might ensue with local Native American groups and potential French and English claimants. All of this took place as a major industry for this period of time in early United States history took its toll on the local ecology and economy. The lumber industry was accompanied by the fur trade industry, probably Point du Sable’s reason for being in this vicinity in the first place. With time, the market was reduced greatly, but other natural products industries took hold. The farming industry remained the primary domestic-controlled industry of this setting. Situated fairly far to the north, the growing fields were limited in use by the relatively shorter growing season, but were established enough to keep this region growing and producing for a short while, just enough for other prospects to make their way into this part of the Great Northwest.
.
Fort Dearborn and surroundings
From 1803 to 1812, Fort Dearborn was in operation. In 1812, it was destroyed when the pioneer families and military residents were attacked and murdered by Native Americans residing nearby. In August 1812, what has become known as the Chicago Massacre occurred, in which the Potawatomie Indians living there took the lives of the others residing nearby.

During the War of 1812, this area became one of the major battlefields established to define United States borderlands. Following this War, this area remained unsettled for a short while, about 9 years, and did not not initiate any major resettlement plans until about 1823, when another series of battles between American military and local Native Americans ensued, and by 1825, possession of this region was duly re-established by the Euro-American settlers.

Chicago in 1820, consisting mostly of open-space. In 25 years, the bend in the south fork will turned into large gathering places for incoming produce, turning most of this land into large stockyards and highly productive slaughterhouse settings. The potability of the river water and the health and safety of its communities, not yet built according to the above map, would change.
Over the next 15 years, pioneer settlements were re-established followed by some early homestead farms. In time, a sizable town setting was established named Chicago. This means that in just 15 years, Chicago evolved from being little more than just a pioneer town to a place where neighborhoods were developing at a record pace. Houses were built next to the river, very close to each other, using the lessons from what engineers in New York City learned about construction of heavily populated settings.
In both New York and Chicago, marshy areas and swamps were often a deterrent to settling certain areas. For Chicago, landfill was one solution to this problem like New York had used, avoidance of these unhealthy places was the other.
Relatively few trees existed in this region, and at the bend in the Chicago River’s south fork all of these trees were leveled. This open space allowed for larger buildings to be built. Over time, Chicago also became the places for incoming wagons to stop and let off merchandise and people. To the south and west of Chicago were farming regions bearing products that could be sold to residents within the center of Chicago.

Chicago in 1830 (Wikipedia-“History of Chicago”)
North is to the Right
Link to animated map serie of this population growth
By the late 1830s, this hamlet of Chicago was a village and its residents ready more than ever for more industries to be developed. The railroad industry began the construction of rails in 1837, and plenty of land had been set aside for building canals as well. Trains ultimately were able to make their way from the eastern state of Pennsylvania and Ohio to Chicago in 1842. The link to Philadelphia made it possible for northern and southern coastline communities to benefit from these commercial lines. New York also had its connection with Ohio, meaning that Chicago products possible had two ways to impact New York, from the south and from the north. New York City it would end up, became its most important source for revenue, a relationship that remained for decades to come, well into the next century.
The 1840s and 1850s changes in Chicago turned it into a city. As a city, it began with mostly local markets and local businesses serving the outskirts of the urban area. But its ability to communicate with the East by newspaper and train opened the door for new opportunities back East. The traditional countryside to Eastern urbanites was now the farmlands in the Midwest. Eastern urban settings obtained their eggs, milk and cheaper meats from slaughterhouses in the city and just outside their urban core, but the best products came from the west. At least this was the marketing plan established by western beef industry entrepreneurs.
The first urbanization and industrial planning for this commercial hub turned to supply meats in 1857. This plan to industrialize beef in such a grandiose fashion set the stage for new disease problems to develop. Where in years prior, diseases like bovine tuberculosis and Texas Fever were infecting the potential marketplace, not the public health problem had become one that was sanitation related. Massive slaughters and the spillage of blood, entrails and waste onto the factory or dirt-ridden slaughterhouse floor made for some of the worst unhealthy conditions in this country. The economic changes in the beef-steak slaughterhouse industry detail the time frame leading up to this first of its kind epidemic in Chicago in 1863.

Chicago Populations, ca. 1840 or 1850
Chicago’s main role as a hub for west-to-east trade and commerce related to the numerous farmlands of the midwest. With the establishment of railways, most leading to Chicago, its development into a city was at first primarily oriented to the traditional farm goods related to crops. But hog and cattle industries soon became the primary focus of this. In just five years, the production of these two industries increased sixfold, as noted in the following review by Blodget in 1864.
.
It was the above population growth and economic development that led to the epidemic in Chicago in 1863.
Erysipelas struck this setting, spreading across its most heavily populated region, impacting people in such a way that its cause had to be very different from the same disease of years prior. During the first years of any town setting, erysipelas is possible. This epidemic occurred as a result of contamination during surgery, and is that famous infection that can set in whenever someone has a deep gash, an open fracture with the bone showing, or is in need of amputation. In the Chicago setting, the erysipelas seemed to be mostly a disease of the surgical wards associated with the military hospital next to the heart of the city. But the lay out of the city by this time made it possible for epidemics to develop outside to fort setting, for reasons other than human patient involvement. The filthy trade of animal slaughtering for the meat market made for a very healthy setting for the Erysipelas-producing staphylococcus bacterium to grow and impact many people. In addition, the rapid growth of this urban setting outpaced the infrastructure needed to maintain its healthy status as a place to reside within. Health regulations, although present in theory and on paper, failed to materialize much in a way so as to make this urban setting a safe domestic, work, play and commerce environment. Dr. Robert Hamill moved here just as this transition into an unhealthy urban setting took place.
In the following ca. 1850 drawing of Chicago’s eastern border on Lake Michigan, we see a fairly closely packed living area established, with dwellings continuing in the westward direction well beyond the Chicago River’s south branch. Based on the appearances of the jetty in the Lake, with just one major section bearing the lighthouse, this illustration is well before the 1860s but most likely post-1840.

Chicago, ca. 1850
.
The next drawing of Chicago extends this view of the port a little further into the southern region (south is to the left). Most important to note are the parallel ports seen on the bend in the south branch inland. These are the major ports for ship bearing import-export goods, including farming and livestock goods destined for other regions. The large buildings are mostly warehouse settings. Trains come into this setting with farm goods including beef. It was in these warehouse settings that cattle were slaughtered and prepared into processed sides, quarters and steaks for shipment to other locations. At times, according to some accounts of this setting written by later inspectors, the condition of the river water was intolerable due to its discoloration, stench and animal parts strewn about downstream.

ca. 1860 – 1870
.
By 1862, the following railroads were established to supply the country with produce distributed out of the Chicago setting, and with time were extended considerably in each and every direction. The main eastward route took passengers and products through Pittsburgh and Philadelphia up into New York City. The westward route headed to Minnesota’s eastern border town of Minneapolis-St. Paul.
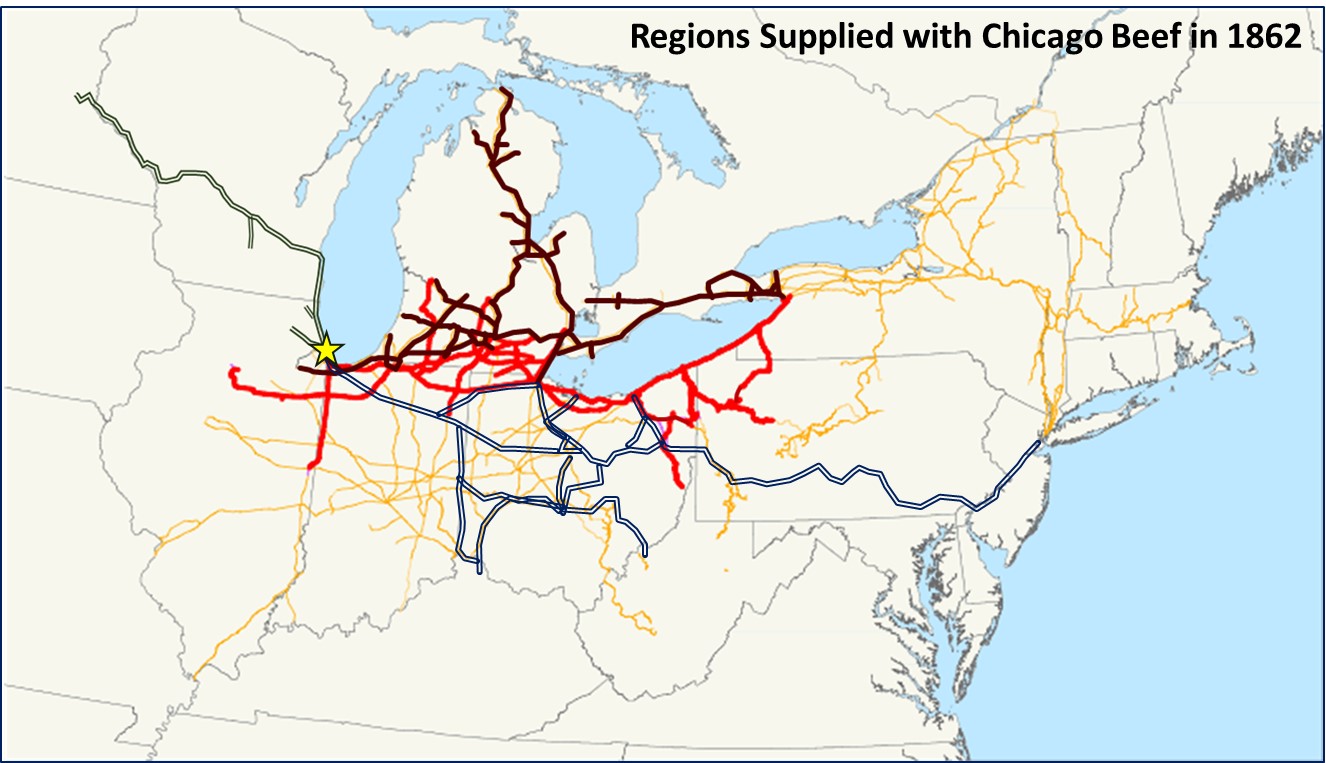
Four railways supplied much of the Northern United States with Chicago Beef. The Chicago Milwaukee RR (Slate Green), Michigan Central RR (Brown), Michigan Southern RR (Red) and Pittsburg-Fort Wayne-Chicago RR, connecting to Pennsylvania RR to NYC (it was later bought by Pennsylvania RR). Yellow routes are extended or local trains.
The primary products carried along these routes for the time were as follows.
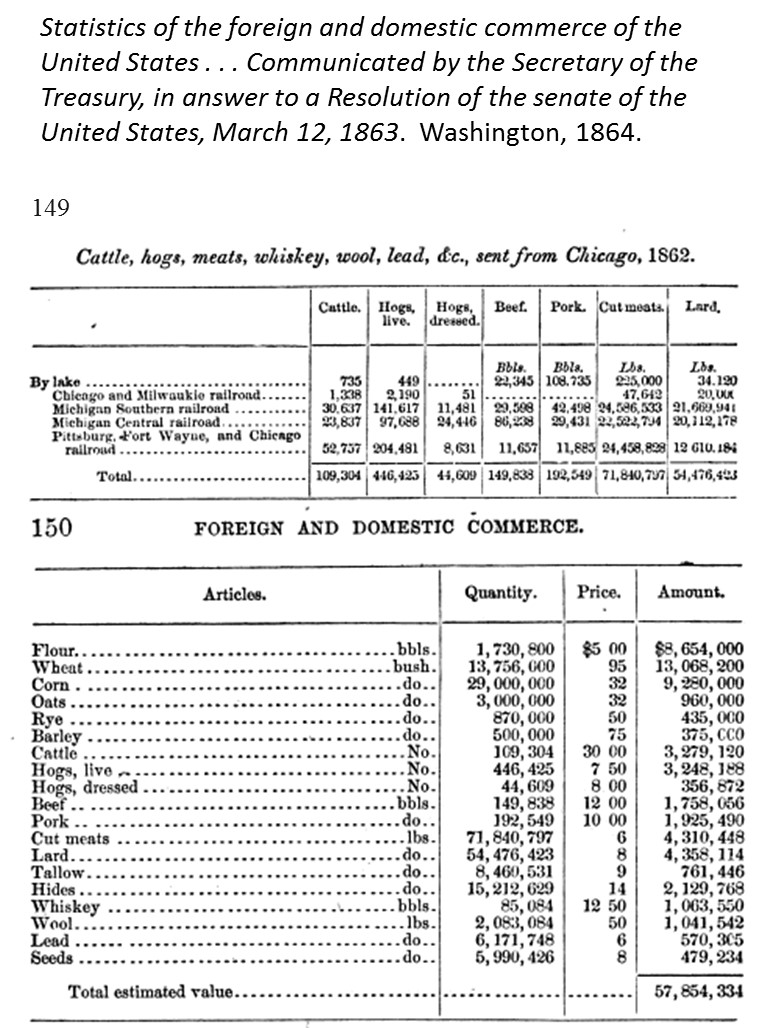
Of the more than 70 million pounds of cut meat supplied by Chicago, approximately one-fifth of this or 14 million tons were cut beef. Source: Statistics of the Foreign and Domestic Commerce of the United States. . . March 12, 1863. Washington, D.C. 1864.
Sequent Occupancy in Chicago
During the first decades of Chicago’s history, we see the disease patterns we’d expect to see for this region. In the minds of doctors for the time, this region was going through several changes as it went from wilderness, to fort, to pioneer community, to hamlet, village and farmlands community, before becoming an early industrial center. This sequent occupancy view of the region tells us a little about the diseases at hand in this setting as well. In the earliest years, we expect people to be taken ill due to their way of living and their interactions with nature and with each other. Accidents, injuries, unexpected work related events, intercultural disputes, all led to the typical fatalities seen for any wilderness setting. When the fort was erect in 1806, sanitation problems were sometimes a problem, and due to crowding a certain amount of diarrhea and dysentery prevailed. Due to the nature of the local environment, cold seasons and winds prevailed, sometimes leading to catarrh (the cold), or worse yet pneumonia and influenza. People with rheumatism experienced joint pains at times in this setting. Those with or without consumption in them on the day that they moved here were more likely to develop such a state either anew, or as a result of the worsening of its state in their body due to local climate and humdity.
In any region, as commercial enterprises cause the villages to grow into cities, sometimes new infectious diseases make their way into the region. Chicago was fortunate in that it bypassed much of the yellow fever history by being so far inland. There was some evidence suggesting this epidemic brought to the United States from afar may have made it way to certain inland settings, but nearly all of these seemed to be directed towards the towns being raised along the eastern half of the Great Lakes setting, like Genesee on over the Toronto and Quebec. For the next series of epidemics, the Asiatic Cholera events, Chicago again seemed to be spared, but places very close by were not, such as the numerous towns and cities in Ohio, Iowa, Illinois, and even the fort settings in Wisconsin, on over to the Dakotas, as late as 1837. When the next epidemic of Asiatic cholera made its way into the country, Chicago was ready, and took a huge number of deaths due to this disease, but not enough to cancel any future plans entrepreneurs had with its setting and location.
The building of canals in this area were at their best by the late 1830s into 1840s. The railroads were high productive by 1842, but hadn’t yet developed an industrial relationship with any other places until 1850. By the mid-1850s, all of the commerce for the area had vastly improved in just five years.
Now one particular feature about the diseases of Chicago was about to change. Chicago turned from being a place for diseases to develop due to commerce and opportunity, to a place able to harbor and raise its own types of pathogens. The first such pathogen responsible for Chicago’s great epidemics were probably the typhus. Any densely inhabited city has problems with sanitation and vermin. The typhoid that came to be in this setting would have been first due to the rodents frequenting the streets. But this typhus, diagnosed as a typhus, wouldn’t compare with its similar or counterpart, typhoid fever. Usually these two conditions were lumped together as a single public health problem during this perid in American history. The two however were very different from each other, in terms of how they are spread, their seasonality, and their long term impacts of population health. As Chicago matured through its sanitation related onset of new diseases, one more new disease would strike this region, the erysipelas that in prior years was fairly rare to the setting, and a product of certain communal settings like forts and hospitals where injuries were frequent, fractures in need of skin closure, limbs in need of amputation, places where surgery was regular performed.
Between 1859 and 1864, the rates of travel and amount of shipments increased substantially, setting the stage for the development of an epidemic. There were two features of Chicago now supporting and leading to the onset of a new disease: increased population size and density and increased travel rates and amounts. In sequent occupancy theory, we might also take into account the changes made in the living environment. Just a decades or two before, as Ohio was being settled, the philosophy was that by transforming the landscape into settled property, we got rid of the worst of all natural causes for many of a regions diseases–the fevers and related diarrhea and catarrh (colds and influenza). Chicago was already a fairly flat, level land capable of promoting rapid overflow of air and climate, and thus lacked some of the problems previously noted for Ohio’s terrains, where trees shielded and slowed down the winds, keeping miasma settled in these small pioneer-developed domestic settings and able to perpetuate diseases as endemic medical conditions.
Once the fort of Chicago was replaced by a hamlet and then a village, and the removal of trees took place, fears of this problem dissipated. Yet the openness and flatness of the regional landscape was now enabling strong winter winds to blow into the settled areas during the coldest months of the year. Already a region susceptible to fevers and catarrh, the most common fear was that Chicago would soon to suffer diseases brought on by land use changes. This ‘change in disease type theory’ became a popular belief published in the medical journals. Once pioneer settlements were replaced by small towns and hamlets, diarrhea events worsened into dysentery and at times simple cholera. Such events further supported the change in disease type theory being promoted, a follow-up on the works of Thomas Sydenham from the late 1600s which then pertained mostly to fevers.
Continuing along this sequent occupancy paradigm, we find that Chicago quickly passed through its farming community phase, becoming a more industrial young urban setting with higher population density sometime between 1850 and 1860. This industrialization of the early agricultural industry setting made for even more substantial disease change. With such changes came the in-migration of the worst form of diarrhea yet–Asiatic cholera–followed by a new disease type-Erysipelas.
Delving deeper into this sequent occupancy related philosophy of disease for the time, until Chicago became a city, climate setting and latitude had everything to do with its rapid settlement. Previous epidemics in United States such as yellow fever and cholera were taking their toll on the cities back east. Yellow fever was thought to be ocean based in its origins, and Asiatic cholera a scourge more common to well settled big city settings. Chicago, like other towns back east, was expected to have some common diseases being it was a rapidly growing areas, diseases like diarrhea and dysentery, measles and scarlet fever. And there were always these geographic diseases from the East that could prevail out West as well, such as like Lake fevers common to Genesee Lake and the Finger Lakes in NY.
Likewise, latitude still played an important role in defining how we interpreted the health of a given setting. Fevers were considered endemic to the south, epidemic to the north. Southern or tropical fevers like the dengue and typhus were common to the north, but mostly during the warmer months. Intermittent and remittent fevers were also climatically controlled in the north, with their appearances considered most likely to ensue in the late summer months. Ague seemed to follow similar routes of epidemic travel, and often was identical to most of the fevers we today might diagnose as true malaria (this work was not yet an official diagnoses then). Typhus fever was not yet fully differentiated into Typhoid and what we today consider to be Typhus, and so the typhus also tended to be reported in the colder to early winter months, a consequence of its passage by rodents as true typhus, not mosquitoes in the form of what was soon to be called typhoid.
So, the effects of the Great Lakes as a whole were considered to be very influential upon the Chicago area. One of the major impacts of the lakes as a local health concern was its assistance in the generation of common or non-cyclic fevers. The influenza and catarrh (today’s “common cold”) behaved as expected, being primarily wintertime illnesses.
To a medical geographer from Robert C. Hamill’s time, Chicago was too far north to suffer much of any tropical diseases problems, except during just a few summer months. But it had humidity for us to deal with due to the lake. The winds were also quite a concern for certain kinds of health conditions or predispositions to illness linked to the catarrh, continuous fever, and influenza, especially during the winters. Someone with a weakened “stature” or constitution for example would not be able to tolerate living in this region. Someone who moved there healthy and later came down with catarrh, then a cough, then fever, and finally a weakened constitution, was considered to have a disease pattern that preceded the onset of consumption or phthisis, thereby making him/her prone to such an outcome and a future examples of fatality due to this horrible disease (known today as tuberculosis). Consider for example the clinical presentation of such a person. His/Her production of a prolonged cough began as one mostly phlegmatic in nature, followed by spell of green and greyish matter, then finally granular black debris of the lung being excavated from the inner chest walls, could only mean that consumption or phthisis had set in and taken hold. This represented the full-fledged consumption experience that such a person might experience had she/he resided in a region susceptible to such a disease. It was not a good sign for anyone’s future longevity, and is why many people removed from the eastern states to the drier, hotter and less afflicted western states. In the beginning, Chicago was a less afflicted region.
We can also see how the notion that since Chicago was waterside and filled with strong winds, one might easily consider how healthy it could be to live in this setting. It lacked bad pestilence history due to its recent developments and population growth, and seemed very attractive to those residing on the more densely population, repeatedly fever stricken east coast region. Such thoughts resulted in very little condemnation of the Chicago setting during its initial years, and because Chicago lacked much of a heavy population history, it also lacked much of the epidemic history prevailing back East from 1825 to 1845.
Commerce and transportation made it possible for this very healthy place like Chicago to be converted into one of the worst of places to live due to future disease potential. Sanitation became a problem with rapid growth, inadequate bathing facilities and poorly placed privies making for some questionable unhealthy community settings. The greatest houses at risk for disease were those down by the water.
The 1862 to 1863 period in Chicago history was extremely active both financially and economically. The influx of new settlers into this setting was in part due to the opening of numerous markets. This made Chicago the place for comparison of the two main theories for disease then prevailing. The old-fashioned miasmists, many of whom were the oldest members of the profession, were at offs against the sanitationists, whose philosophy and theories linked disease to filthy habits and living conditions, and the production of the virus, poison, gas, due to these settings. Take for example the following note, published in the Medical Times and Gazette about Chicago’s filthy work settings.

The Medical Times and Gazette (Chicago), Volume 1, p. 540. May 1864.
.

The Mortality of Chicago. The Medical Examiner. Volume 5, Issue 12, pp. 709-712. Quote from p. 710.
.
Meanwhile, the zymotic theory was also developing within the medical profession. Used mostly to classify diseases, the zymotic theory did not explain how and why diseases happened, and so left open the possibility for miasma and viruses and animalcules to be included, along with some unique hypotheses out there about the role of magnetic and electrical events of nature on disease patterns. The main premise for zymotic theory was first determining if these disease was zymotic or not, and then defining its cause. This theory impacting disease philosophy the most beginning in the late 1850s, just before Chicago experienced its erysipelas outbreak.
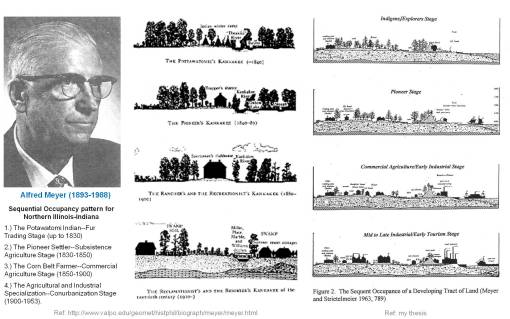
Some of the first Sequent Occupancy theory writings in contemporary journals included Meyer’s use of this theory to explain the living patterns of Ohio-Illinois, parts of which are demonstrated above. The third representation of the right is from my thesis.
Stage 1. Wilderness/Early Pioneer. Common fevers.
Stage 2. Pioneer. Remittent and Intermittent fevers (brought in by ships, but considered local; “lake fever”). Simple diarrhea.
Stage 3. Early Farming. Fevers worsen into Ague types (Malaria) and Yellow Fever. Opportunistic dysentery and various forms of non-fatal “cholera” such as infant cholera and cholera morbus.
Stage 4. Farming and Industrial, peri-urban and pre-urban. All types of fever, with the addition of typhoid fever. Dysentery, and cholera maturing into Asiatic cholera. Increases in poor sanitation related diseases and health issues as well.
Stage 5. Urbanization. Tight living quarters and the constant winds enable influenza epidemics to prevail during the winter. Rheumatism can also set in and phthisis be spread. Accidents and Fire become a public health issue.
Stage 6. Post-Modernism. Ecology is stabilized into a human urban ecology. Sociological, sociocultural and socioeconomic diseases begin to match the diseases prevalent during an early urbanizing natural history setting. Poverty, ghettos, contagious pet or domestic animals become a risk. Environmental chemistry is a threat in a way that is quite different from each the early urbanization period (1970s pollution), or the industrial to pre-urban period (Erysipelas and the Great Chicago Fire), or the Early Farming Period (natural farming chemical, occupational, livestock, farmer’s diseases).

Chicago Skyline and Local Topography, photographed by Robert Elves.
The same disease or diagnosis can impact two very different settings, displaying itself differently in each of these two settings. This may in part be due to the nature of the illness itself. Whereas the presentation of the condition may be similar, its cause is different.
With historical medical writings, there is always this problem of terminology. nomenclature and interpretation impacting the results of your analysis. With the Oregon Trail cholera epidemic for example, “cholera” is not a very specific disease term, it is a word that refers to a kind of event in medicine–the development of severe, debilitating and sometimes deadly diarrhea. The term itself, its roots based upon the word “chole” for bile, infers either black or yellow bile, and perhaps even stool color. In either case, the old humours adage is brought up, implying there is this imbalance in the four humours within your body that is the cause for this condition. Such a philosophy was rarely follwed that closely by the mid-1800s, although the terms used to defined the diseases it referred to remained pretty much unimpacted by the philosophy change.
Erysipelas is an interesting example of how a single disease pattern or diagnosis can prevail in two distinctly different ways in two distinctly different settings. The Fort versions of erysipelas and the urban setting version have very different presentations, pre-diagnosis histories and etiologies. Once again, these etiologies in turn bring us back to the questions related to where this disease first happened, and why it came to be.
Land use and development in the Chicago area defined the erysipelas epidemics that struck this region. From 1810 to 1860, Chicago transformed from a Pioneer/Wilderness setting to an agricultural and agri-industry setting, and with each of these two settings came two forms of erysipelas.
This most common form of erysipelas referred to today is a systemic infection, the tendency for an infection to travel from its site of origin into the rest of the body. The causes for this form are numerous, but in later years were found to be most prevalent when certain bacteria were involved such as Streptococcus that were in contemporary terms, “positive testing”. This form could exist in the blood, spread through the rest of the body and present itself in any of a variety of ways. The epidemic form expressed itself mostly through facial reddening. In the Chicago setting, this form of erysipelas prevailed in the fort surgical setting, and is noted as a complication of post-surgical patients. In fact similar events leading to its onset occurred in numerous if not all fort settings.
.
Early “Erysipelas” was generally wound infection. It was very prevalent in the magazines and journal of the early 1860s due to its recognition, the economic state of development the country was in naturally led to more cases. The improved knowledge base of physicians during this time regarding sanitation theory and disease would ultimately lead up to the development of adequate sanitation procedures during surgery by the end of the 1860s.
The second form of erysipelas came about due to the development of the slaughterhouse industry and poor sanitation practices. This is the form of this disease that struck Chicago in 1863. It presented itself in a different way, and is the disease Hamill refers to in his writing.

Traditional “Erysipelas”, as we refer to it today
.
It is best to interpret this disease in the context and wisdom of a mid-19th century doctor, who had no concept of bacteria and how they infected the body, no knowledge of a difference between a virus and a poison, and only a broad understanding of the fact that unhygienic water contained not only detritus and other smelly, disease-linked materials, but also produced an environment that helped give rise to animalcules that could become pathogenic.
With the increased population of Chicago and resulting crowding came reductions in sanitary living conditions. The following was the cause for the Staphylococcus or Strep A bacterial infection that struck the Chicago setting.
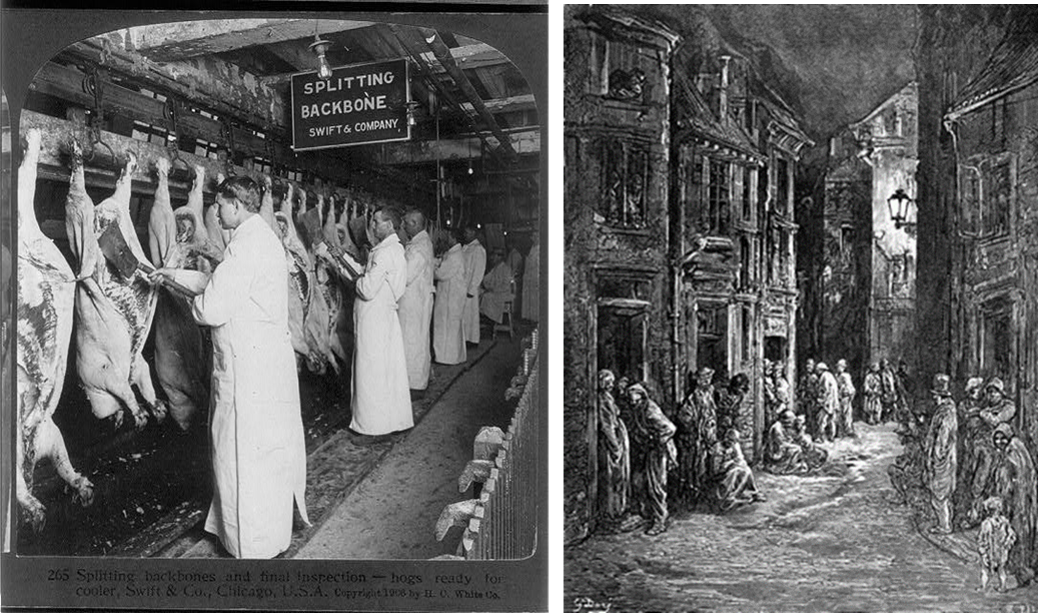
The two primary causes for the 1863 Erysipelas–Poor Slaughterhouse Sanitation (an 1890s-early 1900s photo is displayed), and Crowding in a Newly Established Downtown Urban Setting
The spatial attributes of how this infection spread through the city, depicted in Hamill’s map, provide us with additional insights into the cause of this epidemic. In fact, it demonstrates a pattern of disease spread that helps to define the slaughterhouse industry as its cause. The path its follows is related to the riverside, not a single point such as a surgical site where the cases might have arisen doe to poor hospital or surgical unit sanitation practices. The following are two sets of overlays of Hamill’s infected region over a contemporary image of the Chicago setting.
.

Three views of the Epidemic Area, based on Hamill’s map, with area polygon overlain (approximated) on two aerial photos
.

Overlain, to demonstrate land use pattern relationship to events. No specific slaughterhouse, rail station, or port was defined as a cause for the epidemic during this review. On Hamill’s map, and on recent aerial images, note how the parts of Chicago closest to the identified nidus remain industrial to this day. The layout of dwellings and people have changed very little in the downtown portion of this urban setting. If we assume population density, landuse, building events are fairly equally distributed, we can see the relationship between land use patterns and causes for the observed disease pattern. The assumption made here is although urban settings tend to go in various directions, at various rates in terms of small area/community related changes, that overall, as a “system”, there is a fairly stable rise in height and density over time with different areas varying on rates of growth for short periods of time. The filling of gaps is mostly what ensues as Hamill draws his conclusions from such a map, based on having to differentiate between a sanitation-human contact theory and a miasmatic theory.
.
Referring back to the chronology of this disease pattern at the beginning of this page, the major reason I end it with the 1871 Chicago Fire is that the geography or spatial distribution of the Chicago fire provides important clues to the cause for the erysipelas epidemic eight years earlier.
There was a strange set of parallels being drawn by the medical professionals and their associates with the life insurance industries, the employees and specialists of which included doctors. When the Chicago Fire struck this city in 1873, it became apparent to insurance underwriters that urban density played a major role on one’s morbidity and mortality rates. This interest in the statistical probabilities of life and death was developed by none other than the famous disease and population health geographer and epidemiologist William Farr.
William Farr of London demonstrated that a few feet difference in height above a water surface could either save you or result in your death the next time an epidemic like Asiatic cholera passed through the region. Therefore, in a traditional sense, physicians came to believe that the topography of a region, its flatness, told them a lot about how to interpret an environment and its potential for disease threats. The topography of Chicago, due to its relative lack of an undulating surface, meant that winds could easily pass over the region in very short time; but it also meant that whatever pathogens this wind carriedcould sequester in the small pockets, depressions or eddies formed by the land surface in the form of ruts, ditches, valleys,ravines, etc.. Since these were also places where water could accumulate and water bodies form, these are the places where detritus, decaying debris, stench, and vapours may form and be released to the neighboring communities for disease to develop. This philosophy also related quite closely to the writings of (This also sounds a lot like where mosquitos could be found.)
In general, this perspective of local topography is very much human in that it exaggerated the true physical shape of a landscape, to which we assigned a certain perspective of things that happen (in other words we exaggerate). When Chicago was first settled in relatively ‘great numbers’ (by the dozens) from 1803 to 1812, and again 1825 to 1835, the effects that these surface features had on these people were related to wind, temperature, and humidity patterns, and the effects of these were the fevers, diarrhea and catarrh (later called “colds”) that prevailed. The importance of this interpretation is that it was used to define the healthiest places to settle. It also made us aware of the fact that small area differences were important to take into account. We used this philosophy to identify places that were far away from a water mass to avoid the stench of the swamp, and not be impacted by seasonal flooding, the results of which could be fevers and diarrhea. This philosophy retained its value in the community when it was used to explain the autumn fever, catarrhs and influenza that developed during the pioneer years, and was used to explain why having “the Cold” was a common feature of this high latitude region.

Under the assumption that the Erysipelas was spread by people, one possible route of infection is via an employee carrying with him/her the “contagion”. This individual lived close to the area, and brought the disease into the western edge of the city, from where the disease migrated into the downtown location mostly due to population density features. There are very few inhabitants in the western section of the urban center during the 1860s, and very few west of the peak at the edge of the polygon depicting the disease area. Hamill would have filled in the empty spaces with his concept of how that disease travelled–aerially, or by water, and so imagined it to be river-related. This hypothesis considers it to be employee related, with a direct migration to the nidus, followed by a more general diffusion into the urban core based on social behavior patterns.
Applying this to the Chicago area, when someone lived too close to a large water body like the Great Lakes, bay or ocean, he/she felt the effects of such a setting–in the form of humidity, being taken cold, or developing apoplexy or faint due the unbearable moist heat striking your face and skin. Mist would pass through the city and you home each time the local winds were right. For much of the year, this wind traveled a considerable difference, and at some point lost its pathogenicity–disease no longer struck in spite of its passing. In some settings, the smell of the air and local climate change revealed by pains in our joints told us if and when to expect the next endemic to strike. For new settlers in the Chicago region during the mid-1800s, if one had fever as a kid, he/she could be experiencing arthritis of the knees (a sign specific to rheumatic fever) during his/her mature adult years. By moving to Chicago in search of a healthier living setting, he/she might have hoped to prevent this problem from getting worse, but instead only experienced these problems in a different way, like knowing it was going to rain due to your rheumatic knee or experiencing apoplexy, fatigue and dropsy due to failure of your heart (rheumatic heart disease, related to long term heart valve failure generated by the organism).
For many regions, there was also this problem that the size of the natural events which take place at times didn’t always confer with the geographic model of disease patterns being portrayed about an area. For example, in the Chicago area we can argue that a disease may be due to the wind flowing off the Great Lakes, thereby transferring the humidity, temperatures and miasma of the lakes’ surface into the heavily populated downtown setting along the eastern city edge and from there deep into the interior. For disease to be restricted to this area, the ‘miasma” responsible has to suddenly develop a very restricted flow pattern. It accomplished this by becoming dense and much harder to transport, or somehow, due to the earth’s surface, diffused only along a well-defined ridge or valley. Such is the inference of Hamill’s map of this disease flow pattern. Hamill appears to have considered erysipelas to be a consequence of the environment in one part of its history, when it is infecting the area well upstream from the Great Lake, but very much demographically defined in its diffusion pattern once it struck the more heavily settled parts of Chicago.
Finally, the context of how different forms of diseases develop, if you were a true believer in the miasma theory, had to take into consideration the different definition for miasma that then existed. These different forms of miasma are defined quite precisely in the German writings of Canstatt (which I translated and posted on another page). Canstatt’s take on miasma is that there were those forms we typically imagine, related to the dense air, smells, mist, humidity and the like (“malaria” in its truest sense), and there are these other forms, taking on the behaviors of larger events such as lightning, the cloud of vapours released by a passing comet or meteor (a source speculated for the virus, even back then), the cloud of magnetic energy flowing across the earth’s surface (telluric miasma), the ash and plumes spewed out by volcanoes, the gases sealed within the earth’s crust that get released by earthquakes.
It is easy to conceptualize air, temperatures and humidity flowing great distances across a land surface, but not always easy to conceptualize how these other forms of miasma behave. Observations of these features across land gave doctors insights into disease patterns in spite of their limited knowledge of animalcules, fungi, viruses, anything smaller than the worm. Between 1845 and 1860, this definition of miasma was perfected and the zymotic theory was developed. Many geographers were steadfast believers in anything written about meteorology, climate, topography and disease. But there were also those who believed in energy, electricity, magnetism, galvanism, and the like as the cause for disease, the “telluric miasma” theory which stated that these pathogens erupts or are released from the earth substratum and core, something as imaginative as the phlogistons evolved separately during the 17 and 18-19th centuries, or something as non-visual and non-sensory as causes for earthquakes, tornadoes, volcanoes and other forms of disease producers.
.
The Great Chicago Fire, 1871.
The 1863 Erysipelas Epidemic (Green) versus the 1871 Chicago Fire (1871) (approximated for each)
.

The Erysipelas Epidemic region, 1863 (green), versus the famous Chicago Fire, 1871 (red)
The above maps present the Chicago urban setting, and the two major events related to its demographic history–the erysipelas epidemic mapped by Haviland in 1863 and the Great Chicago Fire of 1871. Together these show us how migration of each of these public health related events was due mostly to population density, but had a non population density factor displayed on this map as well, detailing for us its possible origins. To physicians then practicing, the land surface, buildings and low lying river edges suggested that windflow patterns along the waterway may have assisted in their travels.
This both the epidemic and the fire have remarkable similar behaviors at times, even overlapping to some degree with regard to the reason population density and land use patterns helped to define both of their behaviors. In other words, Catherine O’Leary’s cow or the poor sanitation thereof, may have had as much to do with the erysipelas events of 1863 as it did with the fire of 1871.
By reviewing the two maps, we see there is a significant overlap in the areas depicting the Erysipelas region and the Chicago Fire region. This is because people and population density are the major determinants for the spatial distribution of each. Upon first inspection of the erysipelas epidemic, we might conclude that the water and winds had everything to do with its diffusion pattern. But a part of the logic for this map drawn up by Hamill is very much subjective in nature, like many historical epidemiology maps. The borders defined for erysipelas are based on point distributions and the interpretation of these places by Hamill. The borders for those areas impacted by the Chicago Fire are true continuous surfaces along which various influences took place. According to most geographers, erysipelas was probably spread by miasma, winds and topography, more so than people and their movement. The disease diffused from place to place, impacted people along the way based on distance features. The fire was spread, however, due to the direct contact between neighboring places, the precedent to what we today call the nearest neighbor relationship.
The feature that each of these two natural events shared was then by following the bend in the south fork of the river to the left of the inlet, both of these health problems have overlapping migration routes, each impacting area of significant population density. The major difference that exist between the two pertains to how the northern half of Chicago was impacted. Winds had less of an influence on the ways in which the fire was spread, buildings not people determined the flow pattern for the Great Fire.
.
.
Also important to note here is that Hamill’s mapping of Erysipelas is quite different from other diseases commonly mapped and remapped during the mid 19th century.
In the 1860s, there was more to disease mapping than just using maps to analyze severe bouts of fever and diarrhea. Another disease aside from cholera and fevers had struck some of the urban centers–Erysipelas. Like fever and diarrhea, the name erysipelas at first referred more to the symptom of the disease, which primarily presented as a skin affliction accompanied by . . .
Streptococcus pyogenes or Group A Streptococcus.
In a modern day evaluation of erysipelas, there are three ways this disease usually infects the body. The first is the result of a serious bacterium – — the second is due to the contamination of a food stuff with an organism capable of eliciting the same responses in the body, but often associated with flour and grain related foodstuffs like bread. The third is more common in modern times . . . and is related to . . .
The disease Erysipelas was also commonly known as Saint Anthony’s Fire. The other form of Saint Anthony’s Fire that existed in medical history was brought about by a fungus infecting the grain stores.
The most historical example of this condition is the infection brought on by grains containing a fungus, resulting in the famous ergot due to Claviceps purpurea, with its epidemics of . . .
. The second popular cause, which by the mid-1800s was perhaps more common in developing settings like towns and cities, was the erysipelas which probably resulted in these cases that Hamill discusses. This form of the disease and symptoms is an organism that develops in unsanitary living conditions, occurs due to a fungal growing in these living spaces, follows the population by way of its density patterns, and is highly influenced in where it migrates to due to human travel behaviors and the natural water edge ecological settings closely linked to human travel.
A third cause for a disease much like Erysipelas was Erysipelothrix rhusiopathiae. Associated with livestock, this livestock related cause was very much possible, as evidence by the cause for the Chicago Fire a few years later (Aunt Bessy’s cow kicked over a kerosene lantern into the hay filled barn adjacent to the immediate downtown area.) However, the likelihood that a unique species of Erysipelothrix then existed that could infect humans seems unlikely. Currently, no such species or subspecies has been found to exist, and in general, time and bacterial evolution does progress more in a forward direction, thereby increasing diversity and enable cross-organismal genetic chages (like the vibrio protein transfer into E coli)
Of the two manners in which this diagnoses could have been made, the most likely cause is considered to be the non-foodways related means for passage of this disease. This in part is a very hard to argue line of reasoning, but at first seems obvious. A foodways affliction requires contaminated food, usually grain stores, and based upon the may, we have to wonder how a version of a disease that we might normally associate with silos and grain storage bins could make its way into the heart of the city and apparently spread from the inner core of an urban area southward from its center along the southern branch of the river. (However, the fact that the fire linked to it spatially also started close to the center reduces the strength of this argument.) The fact that this disease is well contained, without isolate points at considerable distance suggests that the purchase of contaminated food is unlikely; although again we don’t know with certain how people purchased and transported their foods back to their home setting, or why the southern homes were stricken much more than any of the northern homesteads up by the 12th and 13th ward. (Recall as well the population density maps for this time, which also don’t demonstrate much difference in north versus south distributions for these two suburban settings; so again, this infers the question — why south greater than north?)
The following map of displays its distribution in Chicago.

[ —> Remember, for the above map, the north arrow points right —> ]
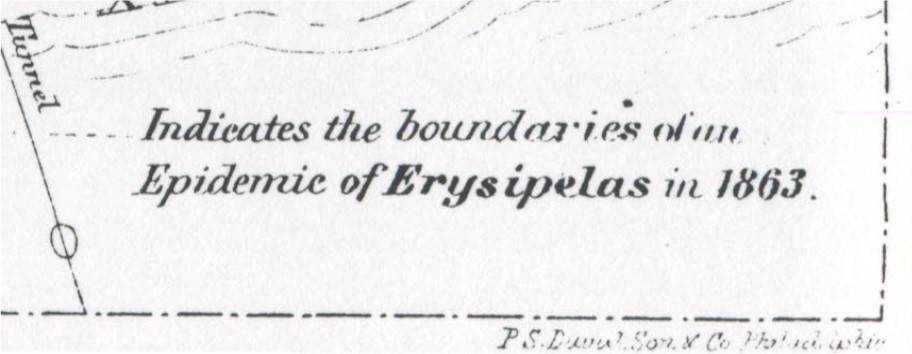
Important features to note about the above map include the tendency for the dashed line indicating the edge of the disease zone to be following the inland river edge, but ceasing before the equally humid, moist lands and airs over the shorelines of Lake Michigan were reached. This meant that people and habitation had more to do with the disease than simple hydrologic effects. In addition, unlike the yellow fever that was so extensively mapped, there is no indicator of a lake edge effect on this distribution pattern. This lack of a lake edge radial diffusion pattern suggests that lake effects, including wind patterns (Chicago is after all Wind City), had a minimal impact on the migration of this disease inland from the lakes. Finally, taking a look at the first photograph of Chicago on this page, we see that the land in this region is very flat. This means that any topography in the forms of mounds, hills and small mountains had a minimal effect upon the disease diffusion process.
These observations about the Chicago region make us to wonder about the following possible geographic features that might have contributed to the riverside flow of this disease pattern (verbalized more in a philosophical sense, in par with the times–the 1860s):
- climate and lakeside/river edge climate and weather (humidity) effects;
- miasma or the like following the surface of the river or being released from the waters below;
- the tendency for riverside related alluvium to be different in form and content, thereby producing a unique pathogen;
- riverside ecological organisms, plants, animals, animalcules, germs and viruses tending to prevail along this region;
- the impacts of solar or telluric energy and the like on the nearby lands due to sunlight and earth’s magnetism, electric energy effects, such as fog tending to form above the river surface and maybe even storm clouds tagging along the river itself;
- the tendency for people to form a population that matches this river pattern due to feasibility of raising dwellings in these locations and government related decisions and restrictions related to such land use patterns.
Most of the spatial features of the early Chicago setting suggest that topography did have an effect on the health of the region in general, due to winds and humidity, but that the river itself and the human migration patterns related to that river pretty much defined the behaviors we see for erysipelas when it struck this city in 1863. Population density is the primary spatial feature defining its path of diffusion, with land use and travel routes playing important roles in further defining these diffusion behaviors. Strongly supporting this observation is another very unique map to be looked at for comparison with the erysipelas map for this time–the map of the Chicago Fire Disaster in 1873.
Both the Chicago Fire and Erysipelas struck Chicago the way they did due to urbanization and population density problems. These two health related events devastated a lot of the same regions with this city setting, with the Chicago Fire spreading more effectively towards the lake edge. This suggests that the primary factor linked to the Erysipelas that struck Chicago in 1867, and related to the spread of the Chicago Fire, had to be something dependent first upon dense population living settings, and then transportation routes. This observation is noted due to the nature of the cause for Erysipelas.
During the 1800s, Erysipelas was a disease mostly of two forms–a result of contaminated grains or ergotism, or a result of an infectious bacterial disease spread directly from people to people, or by contact with a recently contaminated surface or object. The geography of this disease within the urban setting helps us rule out the former possible cause. Were this erysipelas a result of contaminated grains and ergotism, we would expect it to demonstrate a route of diffusion dependent upon commerce, following shipping and horse wagon routes, including routes heading in all directions, including towards the lake edges and/or initiating at some central station for docked commercial goods or farmer-generated goods ready to be transported into the city for distribution.
The 1863 Erysipelas Epidemic (Green) versus the 1871 Chicago Fire (1871) (approximate for each)
The City of Chicago
.
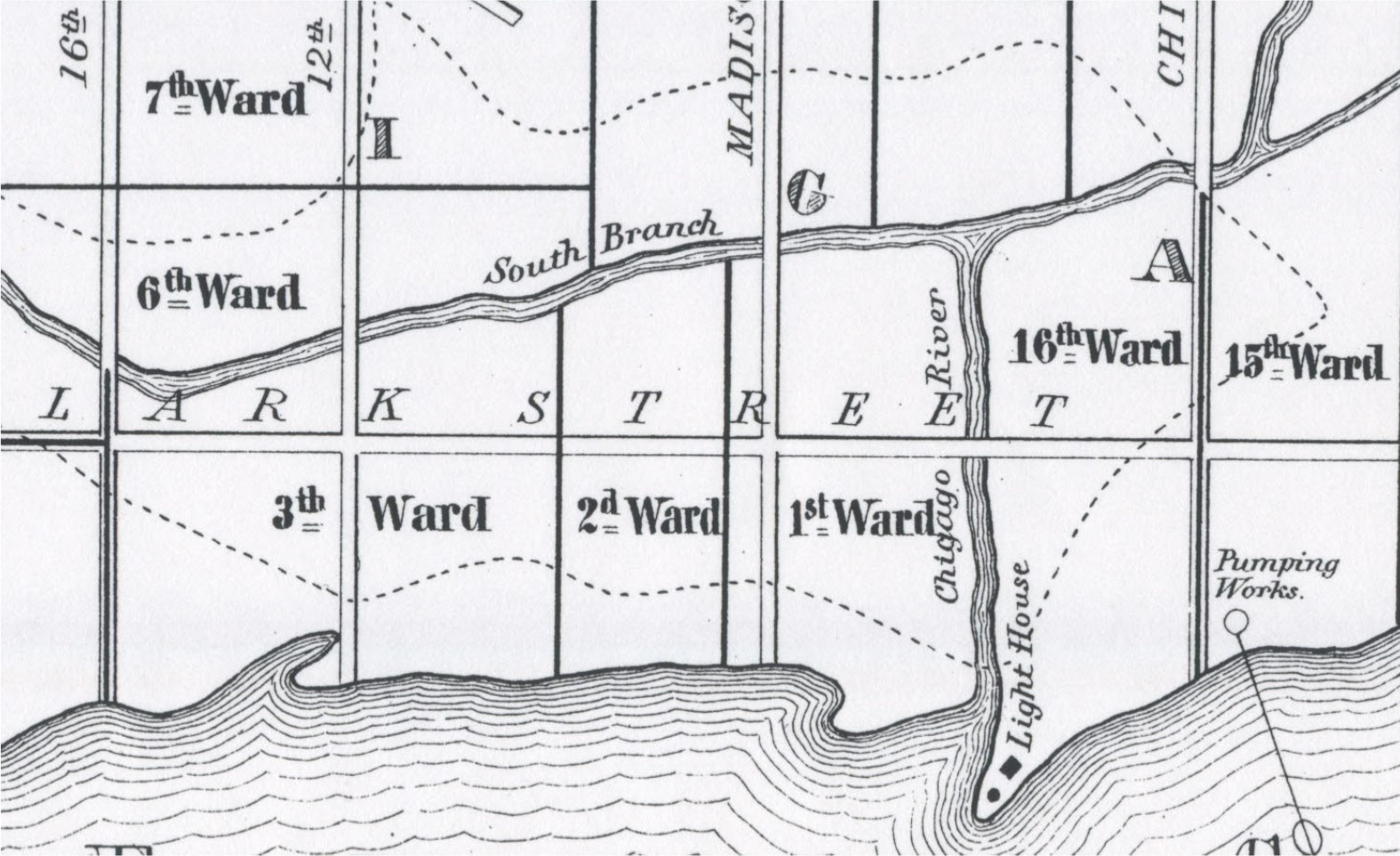
.
Disease Ecology Theory and Erysipelas
Erysipelas. The Erysipelas of Chicago was one of two forms–an ergotism developed from the grain industry that Chicago had taken strong control of, or the result of an infection by Streptococcus bacteria, S. pyogens in particular, a species capable of producing large abscesses along with most of the symptoms of other forms of St. Anthony’s Fire. To understand ergotism, it helps to understand its cause.
Contaminated grains cause ergotism. Since grains are used to make foodstuffs, this is how the disease is spread. Due to the nature of these epidemics, many sequential events clustered spatially do infer some cause related to a group-related behavior in relation to the pathogen. This allows for either cause to be possible. However, the isolated causes occurring throughout close quarters setting like military hospitals suggests the cause to be more along the line of a traditional bacterium or other communicable pathogen. At the time, the bacterium was unknown, but doctors were familiar with the animalcule theory and the various subsets of William Farr’s zymotic theory, a direct predecessor of the bacterial theory. In theory, an understanding of the bacterial theory was possible, and with the exception of the use of the term bacterium, physicians heavily engaged in this work and practice were all too familiar with the possible presence of an unknown, yet-to-be-discovered substance responsible for certain kinds of diseases. The Erysipelas produced by a bacterium very much fit this paradigm in the medical world. The numerous notes of isolated cases, regardless of time of the year, hinting at the lack of any association with any particular grain harvesting period, further supports this hypothesis that this disease was of direct bacterial origin, not an indirect, fungal induced disease of ergot origin.
The fact that most cases are bound by building structures, without evidence for an tendency for certain agricultural products workers or food manufactory settings further supports this philosophy. It conclusion, it seems as though the Erysipelas that struck Chicago quite heavily in 1863 was probably related to hospital, domestic and other crowded indoor settings, where contagion could be easily passed on from one individual to the next either directly due to human contact, or indirectly due to improper sanitation practices involving medical supplies and equipment.
Streptococcus Ecology. If we review the natural and human ecology of the Chicago area, we find it has all of the physiographic and demographic requirements for the production of an Erysipelas epidemic. Applying some retrospective analysis to the history of this region, which I don’t recommend be done too often, we find some contemporary disease patterns behaving in such a way that we are provided insights into how the Erysipelas became such a problem in this setting.
At first we want to simply blame it on a common bacterial disease produced by Strep A positive, which was spread directly and indirectly from one individual to the next. This suggests the most important spatial delimiter to this disease to be population density, transportation routes and people. Still this doesn’t explain why Chicago was so susceptible to the disease. For this susceptibility, we turn to the local disease ecology features of this region.
Even now, with population density at its maximum for the area, the heart of Wind City, the potential physiographic and climatic causes for the disease are eluded to by the city’s fame for its winds and weather. In the winter, the temperates are very cold, and there is a lake effect with the winds that force people into their abodes whenever they need not be in the outdoors. Even during the warmers times of the year, these winds continue to prevail and have the effect of carrying humidity, clouds and precipitation into the city setting. This adds humidity to the air, surfaces and even soil of the region. This the longevity of any microbe in general is assisted to some extent by these environmental features. The Leptosporidioisis or “Chicago Illness” related diagnosis of modern times provides a very good example of this unique ecological and physiographic relationship some microbial diseases have with region first, people second.
Within the non-Chicago setting of southern California, we see a similar biological-ecological reason for infectious disease prevail for the Cryptosporidiosis fungal organism and contagion. For this particular organism, with its widespread distribution north and south of the equatorial belt, but less so within the equatorial belt in those regions where temperatures are at a peak, we see a disease distribution that is very much latitude defined, with the related elevation-latitude temperature relationship defining its places of infection in the hot climate settings. Cryptosporidiosis is a lot like the Chicago Illness, with the exception that the two have very different latitude requirements, and so what se see as a result are two non-connected disease distribution patterns for these two conditions.
The same is true for yet another environmentally linked infectious disease pattern, Rhinosporidioisis, which demonstrates two very specific peaks in places where outbreaks are highly likely, one in the Rhode Island area and the other along the Gulf Coast of Florida. Such a spatial behavior suggests that in this case, the oceanedge environment is very important for the two, implying a role of humidity, but less so for annual temperature patterns. This doesn’t exclude warm weather from having any relationship however. A review of the months or weeks of the year when this epidemic strikes each region would tell us more about whether or not temperatures, or nighttime-daytime high-low temperature fluzxes have any impact on the diseases outbreak behaviors.
Leptosporidioidosis is assigned the common name “Chicago Illness.” It has very
Relating all of this back to Erysipelas, the microbe responsible for this condition is not of the very environmentally linked fungal kingdom of pathogenic microbes. This bacterial nature has attached to it a different extracorporeal ecology, meaning that the human body does play an important role in its continued existence as a disease agent and the potential for future outbreaks happening. Whereas with Crptosporidium we see the organism’s distribution primarily defined by the earth’s physical features, the comparison of this with erysipelas spatial distributions ultimately suggest human population growth and density are the primary factors determining its behaviors, with environmental features, especially temperatures, defining its local nidus formation features. Once the organism responsible for the disease is developed, multiplied into large numbers, either within a human setting or some natural non-human setting, we see human behaviors and presence defining its diffusion pattern, not as an organism, but as a human body-dependent pathogen. This helps to explain the reason why we see this condition in Chicago tend towards following the lower elevation river edge communities, but not so extensively as to make its way into the outskirts of the urban center. Even though river and floodplain settings continue along the two major streams displayed on the map, the migration of this disease ceases at some point inland.
We can relate this to another disease diffusion pattern I covered pertaining to the “jock itch” that Thomas Jefferson’s slaves experienced. Also a population density-dominated disease pattern, this James River Ringworm disease behaved opposite of the Chicago born Erysipelas. The Ringworm epidemic favored very far inland settings, away from the population core, due mostly to sanitation and sanitary living conditions playing a role in its spatial diffusion process. Also, the rural settings, being linked to slavery practices, gave way to the development of less or poorly managed living settings, with the susceptible people residing in very close proximity to each other within filthy living settings or quarters. This setting is very different from the Chicago setting, where the cultural behaviors were different (and of course the time frame 1700 versus 1875 also very different).
The Chicago born erysipelas has the possibility of behaving and transmitting much like it has in the history of the USSR epidemics involving this disease. Contaminate grains used to produce bread to feed the towns was the cause for some of the most famous St. Anthony’s Fire epidemics in that country’s history. Evidence for grainery related Erysipelas in the early colonial years of North American history are also demonstrate in some colonial documents, like the Colonial Doctor’s work I reviewed for another very humid living setting–the Hudson Valley.
Humidity played a major role in the development of the Erysipelas documented in this essay of Dr. Robert Hamill. Stream or river beds defined its distribution physiographically, and in accordance with William Farr’s theory of elevation and disease behaviors within populated areas adjacent to waterways, we see this feature possible also defining why Erysipelas was so effective at hugging the wateredges in Chicago in 1873. Poverty of course may have also played a role here, for as detailed in many of the cholera spatial epidemic studies, we find the lower income communities tending to reside in poorer living quarters, some placed next to the industrial and shipping settings such as ports, low elevation river edges, etc. This led to the infection of communities of Irish and Germans with cholera in Cincinnati, Ohio, around 1850-2, a could very well be the case demographically for Chicago as well in 1873, when the Erysipelas made its way into the city.
So the behavior of Erysipelas in Chicago tells us a lot about the behavior of disease at the time in relation to physiography, climate and demographics. This is what makes Hamill’s work so important to learning the theory of medical geography for this particular period in the history of the profession, and provides us with some very useful insights into how to look at disease spatially, with much of the more people-focused, less-environmentally-focused teachings being distributed today.
.
.
.
 Notice in this part of the map the disconnect between the Erysipelas region and the Pumping House. This implies the water-pumping house activities had little or nothing to do with the epidemic, a spatial feature that dominated the mapping of cholera epidemics by epidemiologists like John Snow.
Notice in this part of the map the disconnect between the Erysipelas region and the Pumping House. This implies the water-pumping house activities had little or nothing to do with the epidemic, a spatial feature that dominated the mapping of cholera epidemics by epidemiologists like John Snow.
The T-junction of the rivers could be very well interpreted as a place where water tends to become briefly turbulent and/or stagnant, enabling the disease causing factors to be released from the waters into the local air. This suggests a downhill behavior of the disease, meaning it may begin forming its miasmatic cause upstream, but it isn’t until it is near the end of the waterflow, near the heavily populated areas, that the disease actually manifests itself. This implies three requirements for Erysipelas: build up of pathogen in the water, release of this causative agent from the water due to slowing of waterflow and such, the presence of large amounts of people in the vicinity so that an epidemic can form, erupt and be rapidly spread.
Erysipelas (green) and the Chicago Fire (red). The two polygons were developed on separate maps, with the yellow rectangle indicated by four major streets produced on each map; this yellow rectangle was used to indicate the boundary locations found on each map for subsequent overlays.
St. Anthony’s Fire and the Great Chicago Fire
Urban fires have been a problem to urban health for centuries. In New York State, urban fires disrupted city life in upstate New York one major town after another, impacting Troy and Albany at nearly the same time in the state’s new history around 1800s. The crowding of homes and placement of homes so close to each other is what enabled these patterns to develop. In Chicago, this crowding was developed to an extreme. First settled around 1800-1810 by people from the same setting in New York, the first few decades gave this region the time it needed to transform quickly from a very rural fort setting into a village, town and then finally city setting, complete with some of the best cultural features for the Midwest and some of the most unique lifestyle habits of any sophisticated multicultural setting being developed in the multiethnic United States population then forming.
It is perhaps no coincidence that the fire that strike Chicago in 1871 impacted many of the same communities stricken by Erysipelas in 1863. This spatial overlap of the two very unrelated social problems has a message attached to it about urban life. The message is that crowded living conditions and rapid development of these settings without appropriate management often has its impacts on the social setting or society at large. In the case of Chicago, increased population density made it possible for a disease not normally considered high risk for the area to evolve into a form that is high risk, and if given enough time to naturalize to the new environment, becomes more permanent and endemic in nature. Likewise, the conditions needed for a building fire to rapidly spread across such a large region have attached to them similar living arrangement settings and behaviors or features considered high risk. The poor sanitation of a crowded urban environment, when flammable materials are added to the scene followed by the technology and sparks needed to generate such a threat to public health in the form of a fire. It was the crowding of people that enabled Erysipelas to spread across the core of the city in 1863. In 1871, the crowded homes and perfect climatic conditions made it possible for an entire city to be burned to the ground.

An early Chicago Street Map (date?) demonstrating primary residential districts. The Chicago Fire, 1871
Could the farming communities have set the stage for the bacterium responsible to Erysipelas to take hold of certain regions?
It is very possible that the characteristics of land use by farmers did help make for a more environmentally supporting setting for the Streptococcus responsible for this disease to develop. The lack of adequate sanitation, in combination with close dwellings, with bacteria rich farming communities residing right next, made it possible for the human ecology requirements for erysipelas to be met. Therefore, Saint Anthony Fire made its way into this setting.
The symbolism underlying these two histories of the area never really came to mind on behalf of local worshippers. The local priests and reverends failed to see this parallel that they could have used to cite yet another controversy by claiming God’s Hands were behind such an epidemic.

Impacts of the 1871 Chicago Fire
There is this uniqueness to the behavior of disease and health after the Chicago fire. The environment was changed dramatically by the fire, but set the stage for new diseases to develop. A common consequence of such tragedies include poor sanitation practices and environmental exposure to new pathogens and particulate-ridden air. During the 1890s and 1900s, the growth of the population in northern Chicago was much greater than that of the southern half of the city.
Plumbum Oxide and Sanitation
The effects of overcrowding, densely packed buildings and other physical features on public health didn’t stop with the Great Chicago Fire. Once the fire was over, the city had to be rebuilt. The paint and chemical industry was in its infancy when this city was first built in the mid 19th century. The paint industry was on its way to maturing in the 1870s. By 1880, chemical industries in general were becoming well established. With the start of the 1890s, chemical producers were split between producing products from scratch or remaining completely dependent upon natural resources. The biggest chemical industries were now making the chemistry lab a standard in education. The American Chemical Society developed industrial chemistry into a specialty. In the late 1880s, Germany produce four to five times as many chemical products as any other country. Within fifteen years, we were fully engaged in the same and by 1900 we were almost caught up.
Now, it had become more than just an industry specialized in the use of natural resources. Chemical manufacturing had progressed and substances not well researched were being invented.
Nearly simultaneously, in 1891, the bacterial theory of disease by the ten years old, had developed a stable following. The massive public health movement after the Chicago Fire led to the rebirth of an older adage, the belief that whitewashed walls could be kept cleaner and made more healthy. Plumbum oxide or whitelead had been around for centuries. The used of plumbum recipes to “whitewash” walls was practiced on and off for centuries. The esthetic values of whitewalls soon led to scientific values regarding pests and disease.
With the sanitation movement of the 1870s having irs influences, the idea of keeping a clean looking home with whitewalls became a standard. Whitewash allowed us to see when and where molds began to form, and enabled us to keep a cleaner more sterile surface. Ultimately this led to the belief that twhite lead “paint” or whitewashed walls helped eliminate and prevent diseases caused by bacteria. Still later, it was believed that the lead oxide prevented bacteria and mold from setting in on the walls.
When the Spanish Flu Epidemic came to this country in 1918,we were more engaged in this line of reasoning as the need to sanitize everything came to be. By the 1920s, Federal requirements were developed requiring that lead paint be used to paint over the coarse surface wallpaper found in the interiors of older homes. From that point on, many of the newer homes being built also had lead paint applied to their interior. We wouldn’t really recognize the impact this had on children until a few decades later.
The peak years in the use of Lead Paint extend from about 1920 to 1940. Lead paint use for interior decorating continued for decades to come, but some very popular substitution products for paints were also being developed by the petroleum originated latex industry. With time, the use of lead paint decreased, and was finally eliminated in 1977 when Federal Regulations were developed preventing it from being used for interior household settings due to the documented impacts of lead on children’s health and learning abilities. Evidence for lead exposure could be documented due to another technological development, the Xray was improved in sensitivity and detection ranges, enabling the detection of lead exposure through the solid line formed on a long bone’s epiphyseal plate, in particular the humerus and femur. (see “Understanding Lead Pigment Litigation” for more details on this history.)
.
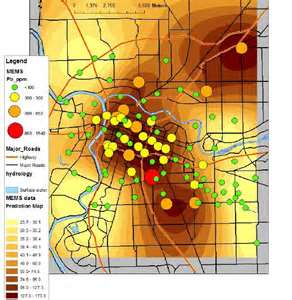
So, what began as a study of the diffusion of wind, weather and disease over the city of Chicago progressed into a more effective public health use for maps.
.
.
.
ROBERT C. HAMILL’s BIOGRAPHY (Transactions. Illinois State Medical Society)

.

.
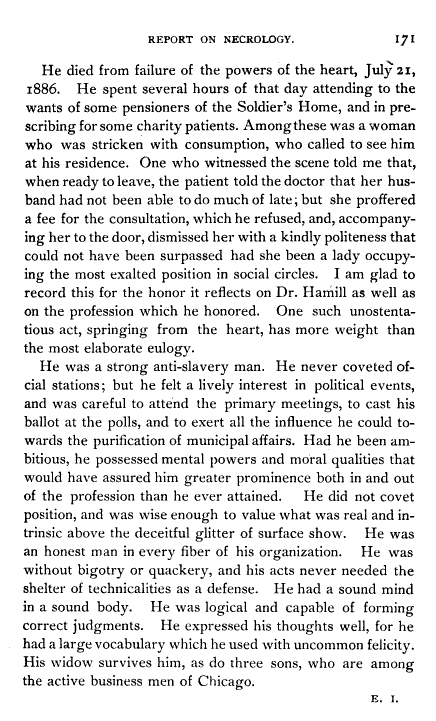
.
The following chronological events are a merging of information pulled in part from the above notes and from Wikipedia page on Chicago history:
Chicago History in Relation to Medical Cartography History
| YEAR | EVENTS |
| 1720 | >Homann’s Dissertation on medicinische geographische is published, in text form (no map) |
| Pioneer….1781….. | >Jean Baptiste Point du Sable settles in Chicago |
| 1790s | >Leonard Fuch’s world “map” is produced; in text form, it describes the diseases of the most populated parts of the northern half of the world |
| 1803 | >Fort Dearborn is erected |
| 1797/1804…. | >Valentine Seaman’s map of yellow fever in New York Port region of NYC |
| 1806/7 | >Fort Dearborn massacre occurs |
| 1812 | >British defeat the Fort; survivors leave and are massacred by British forces. |
| 1813-1819 | >Friedrich Schnurrer’s world regional geography books developed (no maps) |
| 1816 | >Potawatomi Treaty of St. Louis results in a reacquisition of Chicago |
| 1818 | >a Fort is rebuilt in the Chicago area |
| 1827-1831 | >Friedrich Schnurrer’s depiction of diseases on the globe gets developed into a map by a publisher, with handwritten notes added |
| Agriculture… 1829…. | >Chicago population is less than 100; the first canal is built in the area |
| 1830 | >August 4–there is official recognition of a municipality known as Chicago |
|
1832
|
>General Winfield Scott bring troops to Chicago, along with cholera; Chief Black Hawk is defeated, freeing up Chicago for safe settlement. |
| 1832-4 | >Numerous books are published on cholera epidemic geography; Cincinatti is a focus. |
| 1833 | >August 12, 1833, the Town of Chicago was incorporated, with a population of 350 |
| 1834 | >July 12, 1834, the Illinois becomes the first ship to arrive in Chicago, sailing from Sackets Harbor, NY |
| 1837 | >State of Illinois on March 4, gives Chicago a city charter; the county and region around it are referred to as the 9 mile swamp. |
| Agriindustry….1840….. | >A map of cholera in London is produced and published, depicting miasma as the cause; zymotic theory is just 3 years old. |
| 1840 | >Chicago population surpasses 4000 |
| 1842-1849 | >Irish Potato Famine leads to a massive migration from Ireland to the US, incl. Chicago |
| 1847 | >Harvester Factory built; a German Miasma based nosology is published and becomes very popular in certain parts of the world |
| 1848 | >Illinois-Michigan Canal completed; Heinrich Berghaus’s Global Disease map published |
| 1849 | >Asiatic Cholera written about again; William Farr’s zymotic theory becomes popular; other theories begin to surface and prevail. |
| Industrial….1850….. | >Chicago population is 29,963; different medical geography theories for cholera now exist and are abundant |
| 1850s | >A number of railways make their way into Chicago; 50 by the end of this decade. This converts the southern end of Chicago into a major industrial, agri-industrial/meat processing center. |
| 1852 | >Asiatic Cholera epidemic is continuing but is near an end |
| 1856 | >The City of Chicago is elevated 4-5 feet to deal with soggy lands; Adolph Muhry and Andrew Keith Johnson publish their Global Disease maps. |
| 1860 | >Chicago population is 109,260 |
| mid-1860s | >The Civil War began in 1861; zymotic theory prevailed; British medical geographer Wm. Aitken and global disease mapper John C. Peters become important contributors to the United States medical geography/sanitation philosophy of disease |
| 1863 (1867) | >Erysipelas epidemic strikes Chicago in 1863; a geographic interpretation of it is published in 1867 as part of a regular report to the state. |
| 1870 | >Chicago population is 298,977 |
| 1871 | >The Chicago Fire strikes the city |
.
.
HISTORY OF MEDICAL GEOGRAPHY MAPPING NOTES.
Background History
Prior to the 1860s, the following develops in disease mapping took place:
- 1720. “World Disease Mapping” (in thought and theory). Atlas writer and cartographer Homann, following in his family’s footsteps as an Atlas publisher and cartographer, published his dissertation of “medicinische geographische”. No maps were attached to this work, only the theory of disease distribution in relation to culture and lifestyle around the earth.
- 1787. World “Map” (ditto). Leonard Fuchs “map” was developed, but described only in text; this book led us to an understanding the details of health and disease for the most settled parts of the world. Some consider this work a follow up to the military mapping of places and health as the health of soldiers related to places of stay. Fuchs work focused mostly on the most inhabited regions of the world and as the title reveals, diseases typical of well populated settings. Fuchs reviewed health and diseases by continent and large countries, and for the most part focused only on the northern hemisphere, its temperate zone regions and a few southern portions of the Arctic . Fuchs’ work pretty much ignored the southern hemisphere and tropical settings.
- 1797, 1804. Local Mapping. Valentine Seaman’s map, a true disease map (not left up to the reader to imagine from a text description), was produced depicting the yellow fever which impacted the southern end of Manhattan Island, New York. Only a few cases are mapped. Two very local maps were produced and published for the southsoutheast and southeasteast shipping docks. This is the first detailed map depicting places and cases in reference to the spatial relationship of disease and land features or use. The controversy for the time was whether the yellow fever that struck was imported by ship, or of local origins. Cases set inland anf far from the ports inferred a local miasmatic cause.
- 1813, 1815, 1827,1831. World and Regional Mapping. Friedrich Schnurrer, an expert in Asiatic history and culture, visited China due to the growing publicity about the cholera epidemic in this country. The interest in China and its diseases became very popular due to the traditional crowding and disease spread often seen due to the annual migrations to Mecca. Schnurrer later wrote a book about his observations on the geography of disease, followed by another book on the nosology of disease as it related to the different parts of the world. In 1827, Schnurrer’s first maps were focused on global disease patterns for both northern and southern hemispheres. To produce these maps he essentially added lines and notes about specific places on a standard basemap. In 1831, two of these maps were published in a popular periodical, one of which was about the recent Asiatic cholera epidemic, the other depicted the distribution of “diseases” worldwide, although these “diseases” were two to five letter phrases describing mostly the details and descriptions about signs and symptoms.
- 1830-1835. This second pandemic of cholera made its way through Europe and over to the Americas, resulting in the publication of numerous books with maps on cholera and a few on yellow fever. Miasma was a common theme, with an emphasis on filth and sanitation practices. However, a geologic theory was developed by a group who called themselves “Wernerians”. A number of variations on natural sciences theories then developed based on climate, weather, soil, water, telluric energy, gas, poisons, animalcules, virus, germs, etc.
- 1837,1846. A local disease map was produced in England. This map depicted cholera due to “miasma” in London, defining diffusely where the miasma that produced this epidemic lie; the focus was on rich versus poor living communities. Political goals and issues related to social inequality were linked to this map.
- 1848. Heinrich Berghaus produced his global disease map. The first world map of disease, according to most writers.
- 1846 – 1854. Numerous maps, local, regional and global were published about the cholera epidemic. This is perhaps the first epidemic and pandemic disease that struck the world which had fairly complete coverage of its events, often published with maps. The miasma theory for diseases and attached nosology were perfected by German writer Canstatt and published in 1847. In England and neighboring countries William Farr’s zymotic theory was introduced and became popular. The disease concepts most popular by this tome were the traditional miasma theory, Canstatt’s miasma theory, Werner’s geologic theory, the filth-sanitation theory, and Farr’s zymotic theory. These was considerable overlap between these concepts.
- 1857 – 1869. Disease mapping developed into a specialty and had to be reported by regional, state and county medical topographers and epidemiologists. Berghaus’s map led Alexander Keith Johnston to produce his own version of this map in 1856, which wad developed further by William Aitkin in 1863. In German speaking parts of Europe, Schnurrer’s method remained popular followed by a climate-isolines method for mapping disease behavior developed by Adolph Muhry, published as part of his book on Medical Geography. In the U.S., John C. Peters, a combination allopath-climopath-homeopath physician, was introduced to medical topography and climatology and slowly turned to the sanitary theory for describing disease causes. He ceased the practice of homeopathy completely by 1862/4, and resigned as Editor of a national homeopathy magazine. The zymotic theory for disease became the replacement for the miasma theory.
- 1863-7. Erysipelas struck Chicago in 1863. Hamill produced and then published his Chicago map of this disease.
- 1871. The Chicago Fire struck the city, leveling much of the city’s interior built using local lumber.
.
SEARCH
ARTICLES & BOOKS
http://www02.us.archive.org/stream/annualreportofpr01pres/annualreportofpr01pres_djvu.txt
LINKS for more info/readings:
Transactions of the American Medical Association. Volume 18. This article.
H. Nance. A Paper on Epidemics. Chicago Medical Examiner, vol. 8. 1867. Note: Henry County is underlain by a coal bed. The author defines this as the cause. This explanation for epidemics was also reported for cancer in England.
E. Andrews. Lectures on Military Surgery. The Chicago Medical Examiner. October 1861. 2(10):513-520. Gangrene and wounds is the focus, with erysipelas as a result.
(Chicago). The Medical Examiner. Volume 5. December 1864. Editorial.
Camp Misery and the Erysipelas
.
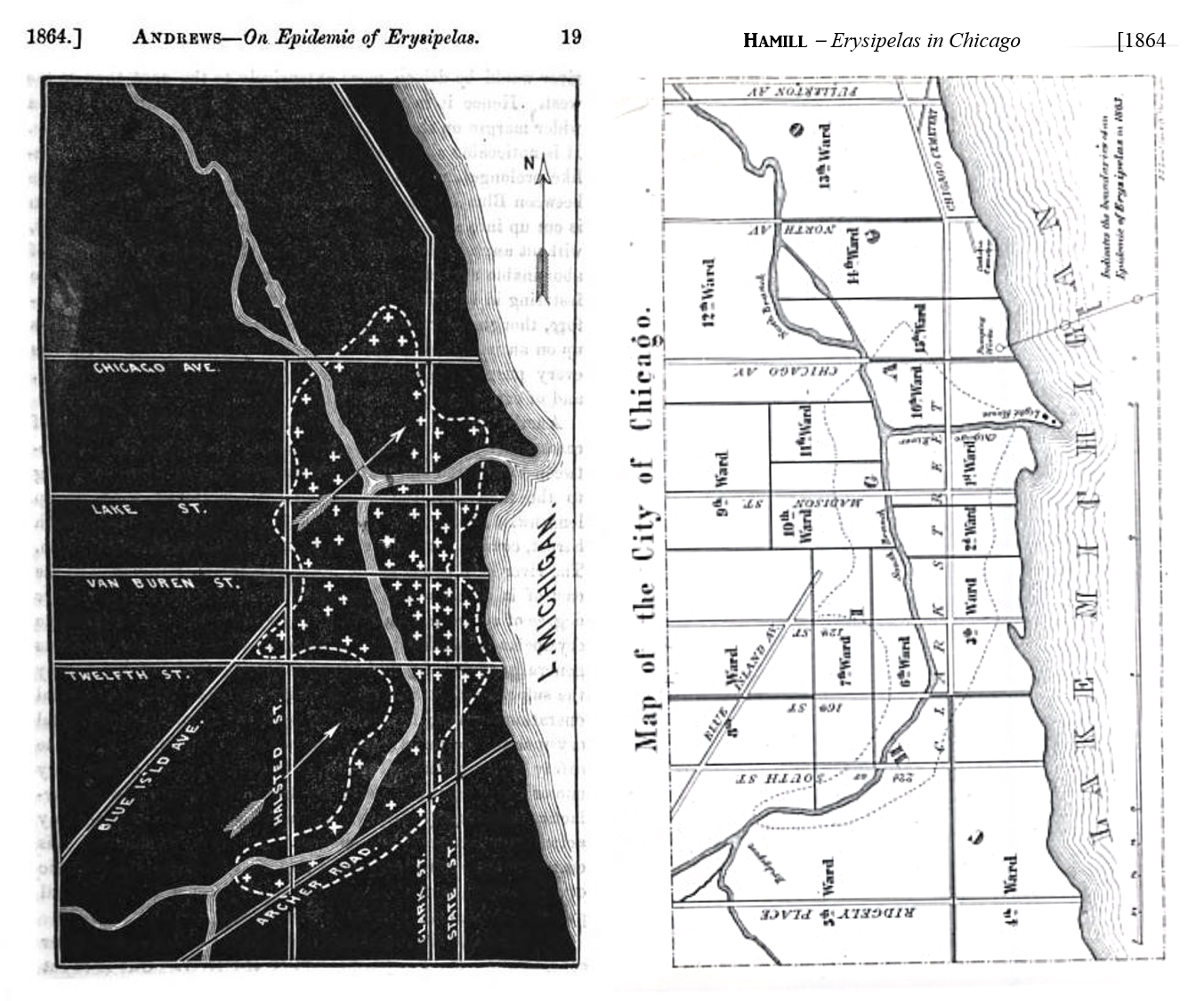

Leave a comment