





![]()
Transcription
![]()
![]()
![]()
………………………………………………………………………………..
Understanding the concept of ‘dysentery’ as a part of colonial medical history is perhaps one of the most underestimated tasks the historian needs to engage in. The first few times I underwent my reviews of Osborn’s vade mecum(ca. 1981-1995), I was very much focused on what modern medicine defined as dysentery–a severe bout of diarrhea brought on by particular microorganisms residing in the intestinal tract. At the time, my conceptualiztion of dysentery and Osborn’s familiarity with this condition included the assumption that Osborn knew about two types of conditions involving the intestinal tract and, as he might have termed it, ‘the purging of our lower parts’.
We can safely assume that Osborn knew about regular stool formation, constipation induced by the application of opium to a patient, diarrhea or liquidy stools, and dysentery stools, which can contain phlegm, blood and/or black bile as their chief diagnostic indicators.
Before reviewing Osborn’s formulas, it helps to understand the nature of a physician’s understanding of dysentery for the time. In a general sense, the term dysentery is derived from dys and enteri. The prefix ‘dys’ refers to something that is “abnormal” or “bad.” The main body of the word-enteri-refers to the enteric or digestive system and tract. The most common definition applied to this term refers to the flux or bloody flux, a case of diarrhea with large amounts of mucilage and blood.
During the colonial period of 1650 to 1750 approximately, there were several forms of dysentery and its associated diseases noted. There was a mostly biliary form of this condition referred to a “cholera”, for which diarrhea was often just one of the symptoms of the disorder. The discharge or irregularity of the chole or bile in the blood was often considered a major cause for these conditions. Since there were various forms of “cholera” afflicting people in all age groups during this time in history, it is often difficult to distinguish the much older descriptions of diarrhea-releated diseases and disorders. Severe deadly diarrhea in infants may be termed “infantile cholera” or ‘cholera infantus’. A form of deadly cholera with black bile as a chief stool and somatic health indicator termed “cholera morbus” (deadly cholera, with black considered a sign of potential fatality). Sydenham reviewed the history and geography of cholera in a fairly detailed fashion in his work, enabling him to be the first to mention the difference between traditional types of deadly cholera with black stools, versus another new form of deadly cholera occasionally impacting Western Europeans–a form of this disease that is found mostly in the Orient in and around what is now India (which we today refer to as Asiatic Cholera).
This review of cholera is important because like Gout, “Cholera” is not at all well discussed by Dr. Osborn. Yet, this is a very well documented disease, with an immediately recognizable cause and humoural namesake. More than likely, because Osborn’s theories for the cholera and dysentery seemed to him to be very similar to one another, his vade mecum mentions just the dysentery. Another possibiliy for this exclusion of cholera from his vade mecum is that Osborn simply did not see any cases developing in the immediate vicinity. It is possible that the bulk of enteric diseases for the valley were mostly simple diarrhea and the expect dysentery-like conditions with bloody, mucus-ridden stools.
Diarrheal disorders tend to have some features that are strongly related to the immediate environmental, economic, and population density features. Simple diarrhea can be brought on by unhealthy water, overly salty water, bad foods, and even certain bacterial infected foods. Someone imbibing too much salt-enriched waters, in particular mineral based concoctions like Epsom and Glauber’s salts (both of which Osborn used), will have a hydragoguic expulsion (expulsion of stools so liquid that this process resembles water sprayed by a hose). The most common forms of diarrhea expected for the Colonial setting in Fishkill include cases brought on by human borne microbes capable of inducing simple diarrhea such as certain E. coli and Staphylococcus bacteria.
Simple diarrhea can also be a consequence of intestinal worms. Interestingly, Osborn nbever really mentions any of these possble causes however. This suggests once again that Osborn’s mind and medical philosophy is primarily extracorporeal in nature, related to the body and its appearances in an outward fashion, not internally or inwardly. [African tapeworm, the most common tapeworm disease now globally, was discovered about 1350, so the association of worms and diarrhea/intestinal problems due to certain creatures had already been documented, though not made too popular.]
Moderate to severe diarrhea, in the Fishkill colonial setting, would be due mostly to opportunistic bacterial infections of the gut brought on by Staphylococi and Listeria bacteria. There are also a number of much more severe forms of microbial induced diarrhea, brought about by such pathogens as entamoeba (amoebic dysentery), shigella (shigellic dysentery) and even asiatic cholera (vibrio cholerae). The problem with these causes possibly inducing epidemics in and around the Hudson Valley is that the required population density features are not there, and the likelihood of a carrier making his/her way from the foreign source of this pathogen unlikely, unless the disease maintains itself by continuously infecting nd reinfecting livestock and humans on board.
For these reasons, it is safe to say that only a few select causes for dysentery existed during the pre-War years of Hudson Valley/Fishkill history: staph, listeria, occasional E. coli, and finally, opportunistic bacteria induced diarrhea/dysentery.
Opportunistic bacteria are microoganisms that are normally non-pathogenic to humans, but which are capable of becoming pathogenic whenever a person is malnourished or for some other reason too weak to surmount a natural defense against their disease causing activities and nature. There are several climatic and weather features that help this disease to recur and progress–like warm weather periods resulting in warmer water for them to inhabit, or periods of drought, which reduce food supply, cause malnourishment in people, resulting in their increased susceptibility to becoming susceptible. Another feature that helps produce more likely pre-dysenteric states pertains to livestock, in particular cattle and horses. Salmonella intermedia and other livestock-related bacterial strains, normally non-contagious to healthy humans, become contagious once malnourishment ensue and natural defenses are down within the intestinal tract. [For more, see my Asiatic cholera thesis work.]
As local population density and size increase, so to do the chances for more rapid disease migration processes to take place. One of the most unique geographical features of military related events is the incredibly rapid nature by which diseases can be transferred from one human population to the next, regardless of distance between the two populations, and regardless of other normally disease preventing features such as cold climates and lack of adequate water supply. Making use of a more recent example, the study of asiatic cholera migration across the Ural mountains in Russia was possible due to the rapid marches the Russian troops undertook even after a few members became infected with this disease spread only by human-to-human contact in such a setting. The abilit of asiatic cholera to makes it was across the Atlantic and Pacific oceans as a human-to-human fecal-mouth contact disease was facilitated by the much higher travel speeds engaged in by American military ships. Likewise, with the onset of the Revolutionary war, some of the above topographic limitations to certain forms of disease onset of spread were removed.
At the time Osborn wrote his vade mecum, his reference to dysentery related to the most common forms of this disease, including the opportunistic form. Once the war began, the travel of troops to America from Britain, in association with land travel between different colonies by inner roadways, made it possible for more severe forms of dysentery to prevail, and even the least opportunistic of disease forms to take advantage of malnourished, fatigues, immunologically compromised troops, residing in crowded barrack conditions.
Taking all of the above into account, it seems most likely that Osborn’s recipes for dysentery refer to his experiences treating both the expected forms of bacterial dysentery (non-amoebic, non-shigellic, non-vibrio), and a few possible forms of opportunistic dysentery. The causes for these cases would have been primarily poor sanitation and contaminated waters, due to poorly placed privies, and infected livestock waste infecting cleaning and drinking waters.
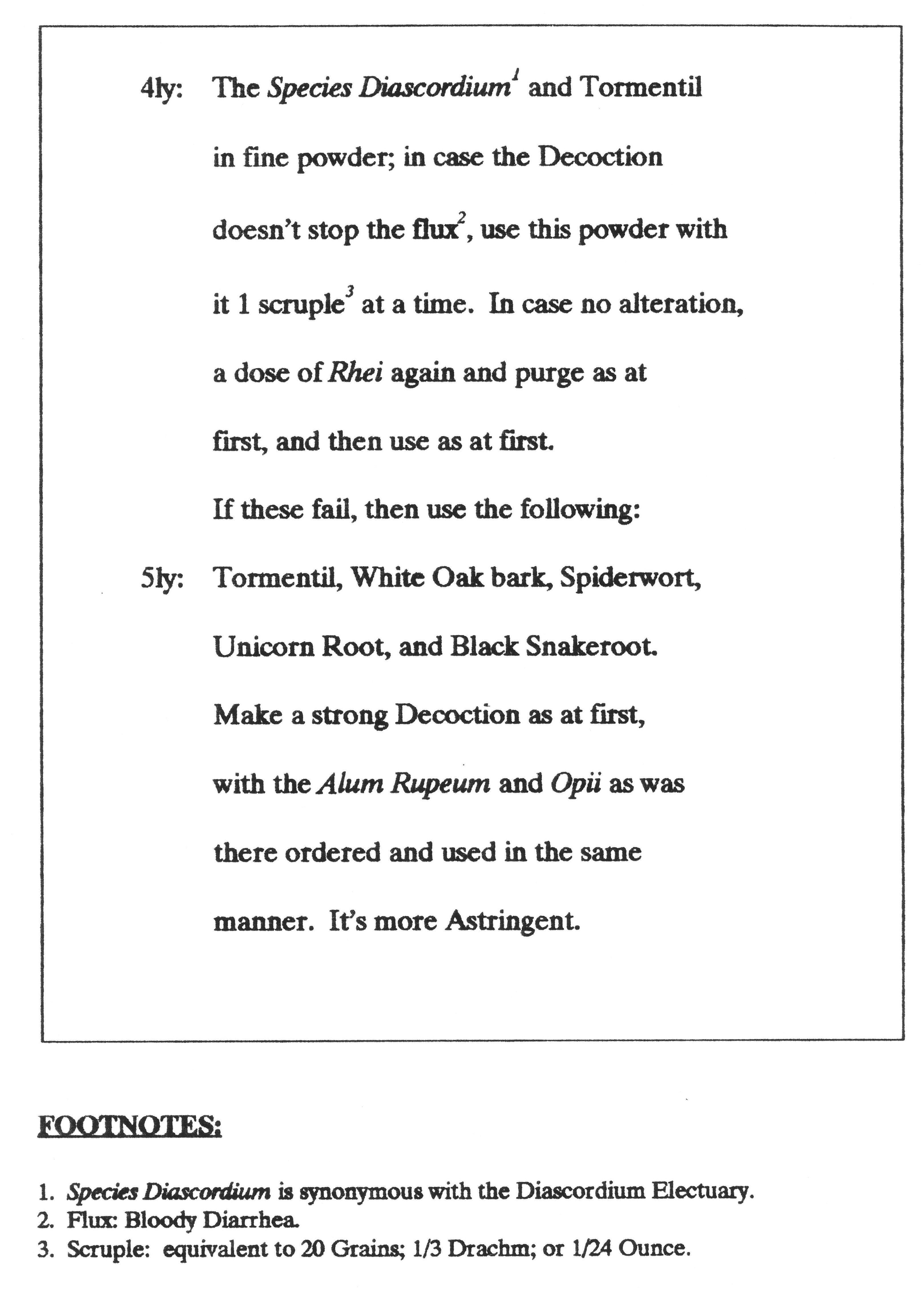
Osborn’s regimens for treating dysentery focused on reducing the water content of the stools being passed. Opium was the primary “cure” for dysentery and severe diarrhea during this period in American history. This was due to the impact of opium on the intestinal wall musculature–it stops intestinal flow by ceasing the contraction of the smooth muscles. Accompanying this therapeutic effect would be the administration of medicines designed to close up the intestinal tract lining, preventing water from flowing from the blood and abdomen into the intestinal tract. Nearly all of the herb and mineral ingredients found in Osborn’s formulas serve such a purpose. The only laxative he gave to his patients for treating this condition was Rhubarb (Rheum or Rhei).
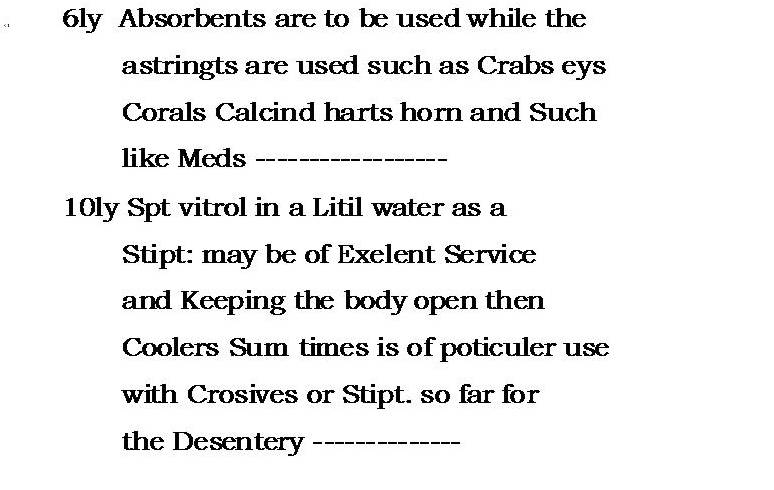
Notice how one of Osborn’s first recommendations is to bleed the patient, in order to reduce the excess volume of blood being eliminated through the intestine by way of bloody dysentery stools. Absorbents such as Crab’s Eyes, Corals and Hartshorn are century old remedies for this problem, the idea being that their rich, dry powdery nature, along with chemical observations made regarding their uses in the lab, suggested they would serve as excellent absorbants of the excessive amounts of water causing the dysentery. If Osborn thought that the body was hot and producing a dysentery, he prescribed a “cooler.” His “Stipt.” (Styptics) served to shrink the openings through which water flowed or percolated. The mechanisms by which he felt his corrosives may have worked remains uncertain (unless he is trying to corrode away some cause for the disease contained in the intestinal tract).
There is also a locally important plant that needs to be mentioned for Osborn’s dysentery recipes. Black Snake Root is a plant with local uses introduced to the world by Cadwallader Colden of Coldengham (near Newburgh), the Governor of New York about the time Osborn wrote his vade mecum. Colden’s writings about this plant acheived worldwide fame, due to the metaphysical philosophy he attached to the folklore use of this plant pertaining to the Balck Snake common to corn fields. None of this metaphysical heritage seems to exist in Osborn’s recipe, once philosophical reasoning is considered. Osborn perhaps used the Black Snake Root (Cimicifuga sp.) due to its Black Bile related physiognomics (though these too are lacking in the field), alongside two other very important plants locally–Unicorn root (Aletris farinosa) and Tormentil (a local Potentilla).

{kind=link}
{kind=link}