Contagious Lung Plague

.

Map Showing the States and Counties in which Contagious Pleuro-Pneumonia of Cattle Exists, By Dr. Chas. P. Lyman, V.S.
Preface
The previous essay on livestock disease reviewed the possible introduction of a cattle born disease from the Dutch or Prussian part of Europe during the early 1800s. If this disease was Contagious Lung Plague or Pleuro-pneumonia due to a Mycobacterium (essentially a cattle-born tuberculosis or consumption), then this introduction noted in the early Medical Repository article is the first such import that is documented in writing. It is possible that several other events with an identical public health history and activity took place in the young United States as well. We typically learn about the first important implant of a disease into a population once it is capable of infecting more than one or just a few of its victims. This limitation in how the disease behaves once it reaches previously unifected territories and populations is an important public health topic that has a direct relationship with the teachings of medical geography.
The reason a disease doesn’t always immediately take hold of a new region has much to do with the sequent occupancy theory taught by cultural and population geographers. The Medical Repository event is possibly a case of contagious lung plague incapable of transmitting much to other cattle due to transportation limitations in terms of time and distance, and due to the nature of the farm and livestock raiser during this time. Large businesses were not well established as of yet. The best source for cattle or cow products was the typical family farm, not the entrepreneureal farm setting more typical of mid to late 19th century farming businesses.
By 1840, the requirements and makings of a cattle industry were now established, and it was possible for large herds to be present when a new disease gets introduced. The early 1840s farms were often more than a family business in the areas immediately around the rapidly growing cities along the Atlantic shores.
Introduction
The initial introduction of the lung plague of cattle into this country was through Brooklyn, N.Y. in 1843, from Peter Dunn’s herd of cattle out of England on the ship Washington. The cattle were kept in a stable in South Ferry. The disease they subsequently went eastward across the western third to one-half of Long Island. Little more is mentioned or known about this particular entry of the Lung Plague.

The second entry of lung plague came by way of New Jersey just four years later in 1847. This is the epidemic that would later plague the New York-New Jersey region and result in the diffusion of lung plague as noted on Lyman’s map.
The Edinburgh Veterinary Journal of 1863 notes a possible introduction of lung plague via New York in 1850. This sole carrier was purchased by a farmer in Brooklyn and placed in a herd, all forty of which subsequently died.
The next entry of Lung Plague into this country came by way of Belmont, just 6 miles out of Boston then (now a part of the city) on May 23, 1858. The spread of the disease took place into 1859, about which time this disease was also noted in New Jersey. Three calves from these dead cows were sold to a farmer in North Brookfield, thus initiating the spread.

May 31, 1860 note
The main hub for imported products is from abroad. As the introduction of this originally foreign disease into the New York area on the following map demonstrates, the New York-New Jersey events are separate from the Boston events, which fail to appear on Charles Lyman’s map of this disease when he first began investigating it.
Many of the products that came in via Brooklyn served the population in New York City, but a number of major industrially-based goods and resources came in by way of these harbors as well. The major import companies in this setting distributed their goods to other investors, and were the first hands many of these goods passed through, individuals who were responsible for their inspection. Brooklyn served as a hub for farming products due to the extensive used of much of Long Island for farming and agriculture during this time. Brooklyn provided the most direct route for transporting livestock eastward on Long Island by way of train, but it was the inland routes by train that managed to infect this country, mostly due to hierarchical diffusion processes.

Possible diffusion process
Without yet reviewing the local transportation history, the map Lyman produced demonstrates possible routes of introduction for the Lung Plague, first by way of the New York Harbor (solid lines) and also perhaps by Chesapeake Bay (dashed lines) if a secondary water route was possible. The lack of cases in the county immediately north of Delaware Bay [dotted line, with ‘?‘] suggests that if any cases did come in by way of this route, they disembarked well inland and were shipped by railway westward, southward and eastward towards New York, and not directly towards the southeast. Likewise, notice how the Brooklyn shipments served the east side of the Hudson River, missing Rockland and Orange Counties along the western shores of the Hudson.
The following is a detailed sketch on how this disease penetrated the inner parts of the country. This is mostly for the initial introduction in Massachusetts, but details about the routes from Massachusetts to New Jersey and New York are also provided.
 .
.
.
.
.
.
.
History
By land, the in-migration of diseases like pleuropneumonia can continue their migration naturally to new regions. Their introduction can be due to poor public health-related trade practices, or even in the form of bioterrorism.
The extensive use of the western half of New York State for farming and agriculture, and during the earlier years in American history, the upper half of the Hudson Valley, made this region one of the more important parts of the nation in terms of farming. We normally do not think of any part of New York State with this important part of its history in mind. However, it is important to remember that the Hudson Valley is where some of the first fruit trees were imported, planted and developed as a part of the local ecology of naturalized plants. The Hudson Valley is also a major route by which a number of crop diseases made their way into this country during the colonial and early post-colonial period in New World-United States history. The first examples of special breeds of cattle were produced in these farming communities long before the lands of some of the more recent states of the continental proper were laid claimed to in the Far West. The first examples of unique forms of equine, porcine, murine, poultry, and piscine products were developed in this part of the continent well before the Civil War erupted.
Such a history of New York is due to its importance as a economic leader and the role of its major routes into the Interior of the United States. It was along these numerous routes utilized by horse wagons, canal boats, trains, steamers, and the first coal and petroleum powered vehicles that many of the initiating causes for epidemic diseases and naturalizing pathogens existed. Like any economically related political and sociocultural change, these changes in history travelled along specific kinds of routes into this country. Like the fruit tree, weeds and farmed products now well adapted to this region, diseases followed the most economically important routes into the countryside, making them an important part of American history.
Some of the major geographically related questions reviewed and answered about the migration of diseases into the interior, at times by way of the valley, include:
- What defines the path, their form, etc.
- Are they based on simple diffusion behavrios or hierarchical diffusion behaviors.
- With these two questions answered, what are the geographical requirements for these diseases to take hold of new regions and new environmental settings?
We get better insights into the answers to these questions by observing the spatial behaviors of these diseases in the past, developing a more concise model of what defined these diffusion patterns, and then use this information to develop new methods for modeling their diffusion behaviors in this country should these epidemics of the past return.

Boston, 1855
..

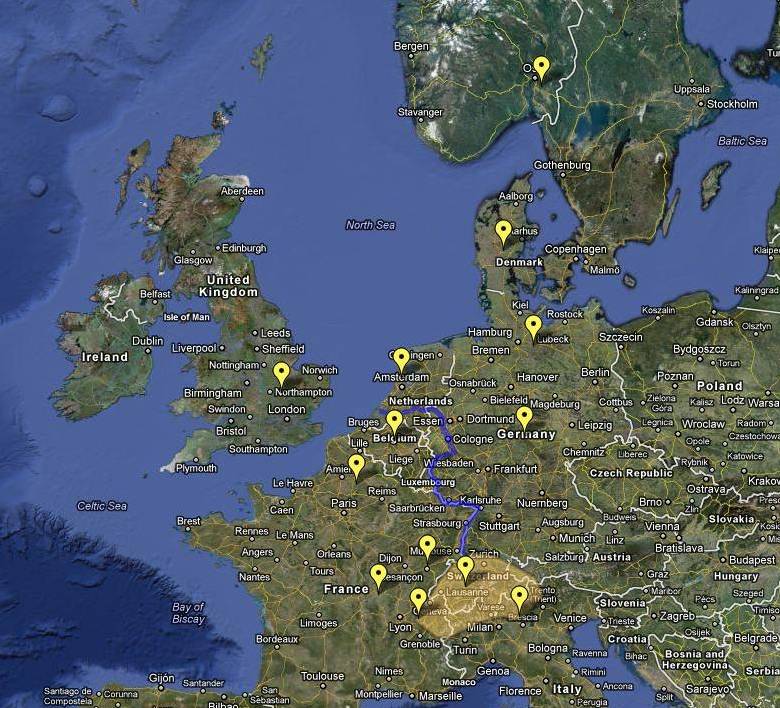
Some of the earliest Western European cases of Contagious Lung Plague infecting Cattle.
The original nidus or source for this disease was possibly somewhere near the boundary of France and Switzerland. (The Rhine River linking the inner parts to the ports in Netherlands is indicated by the blue line)
.
.

The initial migration of this disease to the US was by way of ports in Boston, Brooklyn, and northern New Jersey
The relationship between people and animals is responsible for a certain category of diseases that are both epizootic, meaning they are diseases experienced by animals, and anthropozootic, diseases experienced by animals and then people. Historically, medicine has interpreted human health in relation to animal health and vice versa. There was even a time when both people and animals experiencing the same kind of disease also received nearly identical recipes and medicines. The doctor not only bled his patients, he also bled his horse, his livestock, and when his neighbor trusted his selection of this way of providing care, his neighbors horse, cattle and sheep as well.

The possible source for the American epidemic of 1843 to the late 1850s, possibly to around 1880
Diffusion patterns
The Map
Charles P. Lyman’s Map of Contagious Lung Plague of Cattle in the United States, 1860
.
Close-up of the Point of Entry . . . The Infected Counties are Tinted Darker Salmon or Red.
Based on the review of the first epidemic in Boston, two routes of entry are inferred from this map of the the region below the nidus in Brooklyn, N.Y. As noted on Thursday, May 31, 1860 (see second figure at the beginning of this page), contagious pleuropneumonia made its way into New York by way of Brooklyn. It then diffused throughout this portion of lower New York State before making its way southward into the states of New Jersey, Pennsylvania, Delaware, Maryland and Washington, D.C. The diffusion southward could have been by overland routes, but also apparently involved a water route involving the ports in Chesapeake Bay. This is based on the lack of contagious pleuropneumonia in the county of Salem, New Jersey, situated immediately north and east of the Delaware Bay estuary, forming the three southern most counties in New Jersey. Another possibility for this lack of the disease in southern New Jersey is the lack of sufficient settlements in this region affiliated with the growing cattle industry. A combination of cattle ships and trains was required for this disease to make its way into regions situated well inland from the bays and harbors. The westernmost migration had reached Cumberland County, Pennsylvania by the end of this first diffusion process. Notice as well that the southernmost bay in Virginia does not display this disease in its seaport towns. The southernmost county is Howard, Maryland.
.

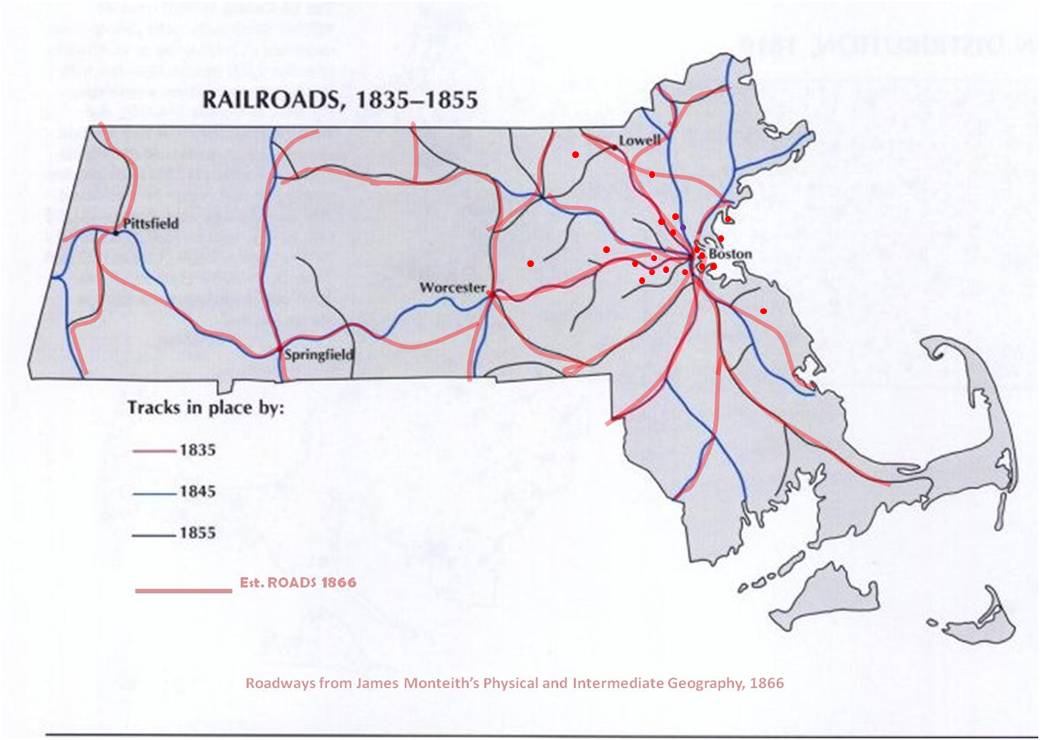
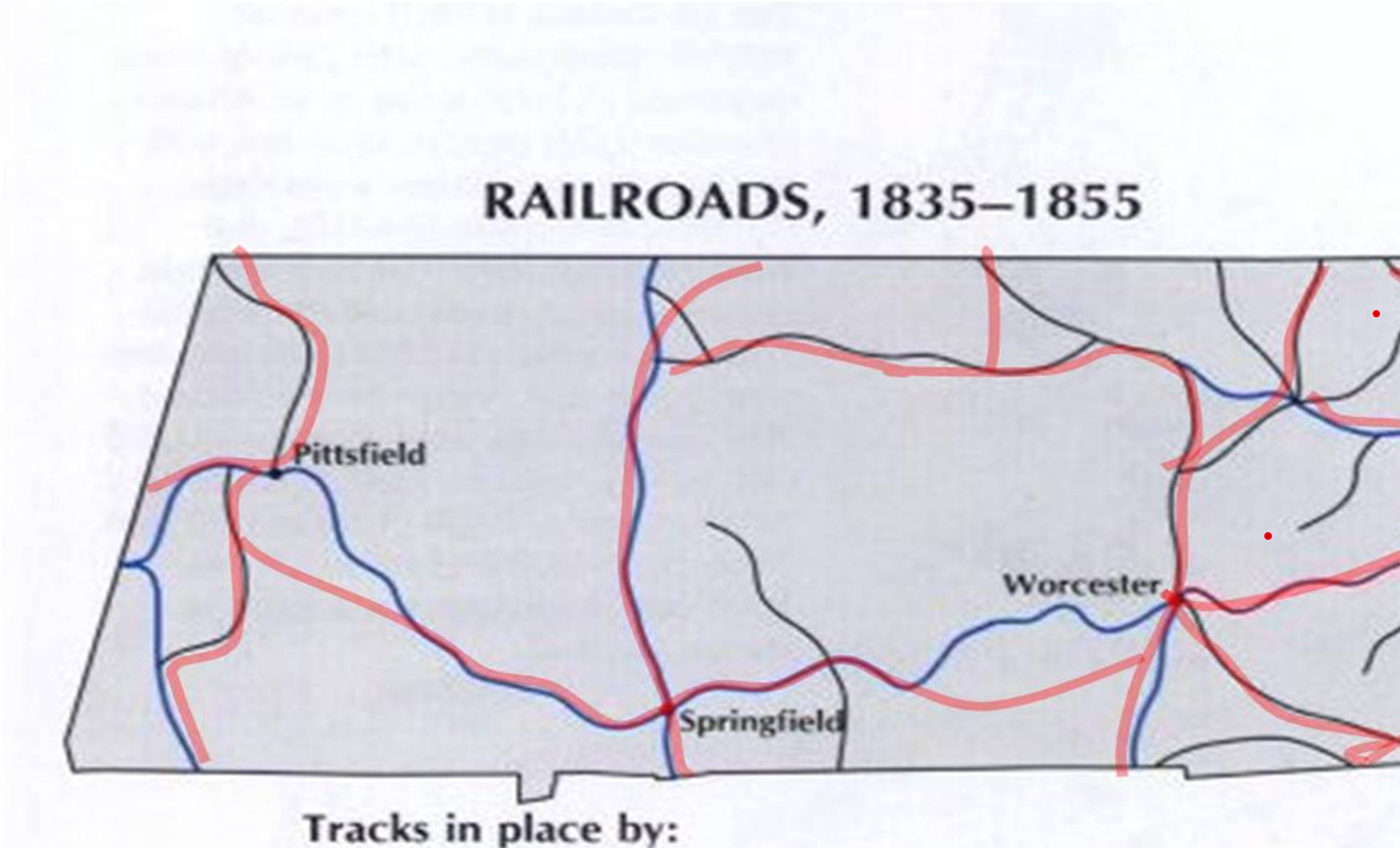
Population maps for 1810 and 1860; Railroads 1835-1855; Contemporary road map
Reviewing this map for the data provided in a history of this disease, we can get a better understanding of the diffusion behavior of this epidemic. Economic Geographer Pyle provided three models for disease in-migration and diffusion processes. He defined the simple Type I diffusion process, in which the disease appears to migrate along well defined routes, for the most part heading radially outward from its nidus in all direction.
The data provided in the following map, drawn from the data on the Boston epidemic, demonstrates the initial nidus for the disease–this is where following its importation, the infected animal was shipped to by way of land routes before the disease symptoms began to display (initial case is indicated by the red pin. All subsequent cases illustrated on this map follow a simple radial diffusion pattern, with the major transportation routes leading the way.

Contagious Lung Plague cases, 1843 – 1850 — the initial diffusion process (is this possibly along two or three railways?)
For these cases a nidus is defined, where the initial case took place. A second and possibly third nidus are defined based on temporal features. These are the first three sites where the cases developed. Applying Pyle’s hierarchical diffusion model to this, this is a Type I or non-hierarchical diffusion process.

Rough overlay of 1843 to 1850 cases and major roadways on railroad (no GIS here)
It is possible that this disease continued westward through Massachusetts, but the historical writings do no mention this. This may be due to the type of relationship between major urban center and its satellite towns, a behavior already well defined at this time by German geographers.
The above image represents what appears to be a simple diffusion process radiating outward along transportation routes for the first nidus. Since this information provided lacks dates, we can assume that travel routes, distance and time are the main determinants. We can also assume for the moment that the major routes of transportation are partially represented by the major route that exist in the above modern map of this region.
Applying Pyle’s models to these findings, we see a Type I diffusion pattern, a fairly circular radial dispersal along important travel routes. The opposite behavior according to Pyles models would be to see three clusters over time developing–that of the original nidus and two others involving the other with the two other very early cases produced by the nidus serving as starting points.
In sequent occupancy terms, this is the result of a disease capable of impacting Level 3 and 4 type setting, but predominantly attacking the most appropriate location–the Stage 2 farming lands located just outside the Boston town or young city perimeter. Livestock industry is essential for this disease to develop into an epidemic, due to its spread within groups of potential victims. Such is less likely to be the case for pioneer community settings.

Transportation History
The following maps are overlays of the infected counties noted on Lyman’s map above, and on the first figure below. This infected area is overlain, and then boundaries slightly corrected according to the text in Lyman’s book in order to better fit the topographic or physiographic boundaries and other boundaries defined by Lyman.
![]()
![]()
![]() note: sw linear boundary was checked and is accurate
note: sw linear boundary was checked and is accurate
![]() note: sw linear boundary was checked and is accurate
note: sw linear boundary was checked and is accurate
.
..

.
The Spatial Diffusion of Animal-born Disease
Farming and agriculture are related to medicine due to the ever-changing technology of the food and agricultural industries. In the most basic sense we are all pastoralists, tending to our crops in and out of the natural environmental setting, either as farmers producing the best crops and livestock, technicians producing the best farming equipment, scientists trying to make the best sense of how these products are made and their values to people, consumers making the best use of these products, economists producing a more efficient financially-minded marketplace, and finally the physicians, epidemiologists and environmental health specialists trying to determine which of these practices and behaviors are good for the people and health promoting, and which of these are bad for the people and dangerous to people, plants and animals.
Health and longevity are the natural consequences of these preventive health activities. Successful monitoring programs serve to reduce any public and environmental health problems that exist, and prevent new problems from developing. This combined and more integrated focus on disease and health human, animal and ecological is a natural product of the application of medical geography teachings to the study of animal-borne disease patterns.
From the end of the 19th century onward, the utilization of the map for reviewing diseases has been significantly limited by the focus on the miraculous discovery of the bacterium and the subsequent shift of focus from disease and the environment to the microrganisn and the human body. This epidemiological approach to studying disease patterns placed too little emphasis on the role of nature in the design and implementation of new disease patterns and behaviors. New diseases develop because of changes in human living behaviors and patterns and changes in environmental patterns. New diseases are often the consequence of what people consciously and subconsciously do. Old recurring diseases are a result of repeated unhealthy relationships people often have temporally and spatially to the causes for disease. The causes are not only animal or microorganismal in nature. They don’t only require man and nature’s various pathogens. Diseases are also a result of environmentally-related decisions that are made, and the effect these decision have on the potential for exposure to new climates and weather, new plants, new animals, new soils, rocks and other strata related features, and how as pastoralists we attempt to modify these natural settings that we did not originally develop within.
There are a number of fundamental rules that can be used to better understand disease diffusion behaviors.

The type of diffusion process is important to understand. Hierarchical diffusion is the flow of knowledge, material gains, money from large populations to small populations. It has been related mostly to the economy and marketplace, and is often monitored and measured in order to better understand the human and biological-ecological behaviors of a given region. Non-hierarchical diffusion usually relates to a some sort of simple linear flow, be it radial in nature resembling the spokes on a bicycle tire, or purely linear representing some sort of straight migration route or the bending of a travelling object as it makes its way laterally from high elevations to low elevations, or from north to south across the surface of the earth, demonstrating some sort of coriolis effect.
With disease, predictions are made based on understanding these paths of travel enough to apply them to new scenarios, making predictions or projections of how a disease might travel. Animal born diseases have the movements of their carriers–the disease animals–to help define these routes, as well as man and the industry which they are a part of. Diseases carried by these food or food product sources usually travel wherever they do. Some are ecological, others simply dependent upon just the animal itself. Tick and other arthropod-vectored diseases depend on the ecology of the vector as well as its animal victim. Bacterial and fungal diseases are usually more dependent upon the animal and environment, and whether it is too hot, too cold, too dry, or too wet for the pathogen to survive between infected animals.
Viral diseases are kind of in between these two, demonstrating diffusion behavior that may be dependent mostly upon the animal some times, and the environment and its other potential carriers other times. The mosquito viral disseminated west nile disease makes use of animal carriers to remain alive and part of the environment, but isn’t a disease really until it strikes a human, then it becomes a public health risk. In a recent review of emerging zoonotic diseases, quite a few were identified:
[insert list, ref, link]
.
It is for this reason that animal diseases are one of the most under-represented risks to people health in many studies, and too often the first to be cut from local government expenses and the least aggressively researched. It often takes events like the deaths of several children due to foods tainted with the pathogenic E. coli and a case or two of elderly citizens dying due to a mosquito bite to initiate a surveillance program for preventing other cases from developing. We can learn as well from past events of animal-borne disease when planning to improve uponthe growing need for animal and animal-human disease surveillance.
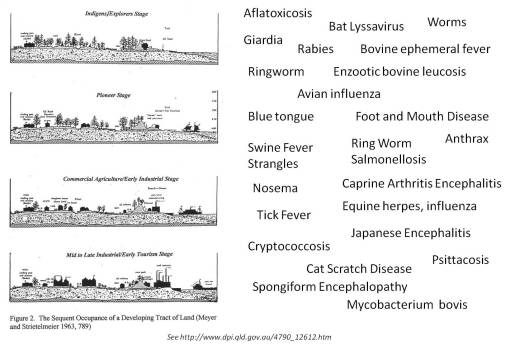
To research these past events, past geographers developed a way to conceptualize population growth over time in the same region, as well as between regions existing in different stages of regional economic development. The Sequent Occupance model enables us to study and interpret disease patterns over time and space in such a way as to develop a better understanding of first the progress of a disease, in particular a known epidemic disease pattern and some recurring endemic disease patterns, followed by applications of this philosophy to understanding the relationships that exist as well in neighboring districts. Whether or not a disease can pass from low to high population areas of vice versa is a product of the nature of the disease itself, its biological or non-biological cause, and the make up of its environment and potential victims.
.
You cannot go back in time, but you can go back in temporal disease pattern types. Applying Meyer’s rendering of Sequent Occupancy to this, we can look at a disease and try to determine how it and its similars change over time. A simple skin infection for example can progress from basic ubiquitous forms linked to salmonella and the like to more specific forms linked to livestock area-enriched microorganisms, like the herpetic nails (whitlows) produced in people who are in contact with bovine organisms, infected or not. This demonstrates how occupational disease and sequent occupancy are closely correlated, and provides a reason for time and place related disease changes. Scrotal cancer was found to be a consequence of coal dust collected on the skin of chimney sweeps. Pneumoconiosis, in a Stage 1 or 2 type of Sequent Occupancy stage, would be primarily a problem experienced by asbestos mine workers, their relatives, and the closest neighbors of these mines, whereas in Stages 3 and 4 it is the average citizen living in a household being remodelled and with a partially exposed inner wall who is most likely to experience the same disease.
.

Sequent Occupancy
.
.
Applications to modern disease surveillance
There are two aspects of Contagious Lung Plague or Pleuropneumonia induced by Mycoplasma mycoides var. mycoides or var. capri worthy of special attention. The first is that this disease played an important role in American medical and veterinary medical history during the nineteeth century due to its behavior spatially and its relationship to a growing world economy. The second is that the history of this disease is important due to its relationship to current events related to medical geography, national security and the world’s agricultural and livestock industries.
Lung plague is an example of an epidemic disease that has the potential of returning to the United States. More importantly, it has the potential for having a devastating impact on the world and national economy and national food supplies. Lung plague has the ability to not only infect livestock, it can also infect humans.
There are a number of possible routes this disease could take if it were re-introduced into this country and managed to evolve into some untreatable, unpreventable form of mycobacterium. These routes incldue a number of waterway routes important to the economic history of the United States, as well as a number of inland routes with minimal involvement of the much easier to map waterways.
When this disease first came to this country it appear as though Boston, New York and New Jersey had the first ports for entry of this disease .
The Hudson Valley is one of several major routes into the countryside and the heart of the northeastern quadrant of the United States that this disease could take. As indicated by historical routes and by recent in-migration routes for numerous other foreign-born diseases, even though New York City and the neighboring burrough of Brooklyn are rarely associated much with farming and agriculture, this part of New York state is one of the primary means by which numerous other foreign diseases even those of zoonotic nature seem to enter this country. For the state of New York, the two other primary migration routes for diseases into the interior parts of the States and the western half of New York, include the international, intercontinental migration and commercial route involving the waterways of the St. Lawrence Seaway and related Great Lakes shipping routes, and much longer the Mississippi River-Ohio River transportation route into western New York.
But waterways aren’t the only way many diseases can be introduced into the interior parts of this country. Whereas water routes are the primary means of introducing livestock diseases into this country, overland routes are responsible for facilitating the diffusion of the disease into more inland regions less dependent upon frequently travelled waterways. A review of foreign born disease paths also demonstrates several overland routes of migration. One of the most important inland migration routes leads from the southern tip of Texas inland towards the southwest US interior, by way of Northnortheast and westsouthwest routes heading away from the central Tex-Mex border. There is also a potential route that proceeds directly northward from the southern tip of Texas, in a direct northerly direction, but this is infrequently travelled suggesting there to be some sort of environmental, topographic or low human population density barrier that reduced the potential for disease migration.
Yet another series of routes applicable to the in-migration of foreign diseases are positioned at several corners of the US shore. The Pacific Northwest border has Portland and Seattle as major sites for diseases to arrive by ships. The southwestern corner in California has an oceanway Pacific coastline point of entry, and a southern land-water route that is primarily overland, but may involve Baja as well, leading diseases into this country either via the southwestern Texas edge proceeding in a northwestern direction into the US, or via an indirect route from western Mexico, across the water to the Baja peninsula, and from both sides of this region northward directly into the US.
Another ocean/bay route is seen in Florida as well. This route suggests possible entry either from the Carribean and Bermuda, or from Mexico, or perhaps Central America and parts of South America.
One of the interesting features of these parts of the country where disease can enter is the form of the 3D maps of disease distributions in these regions. Niduses and points of entry are easily defined by these shapes for the nidus regions. A typical effective point of entry displays a center or core where, relatively speaking, high numbers of diseases are reported. This is surrounded by a series of lower count areas which serve as supporting regions for this type of disease behavior. At times, these regions take on a target like appearance on disease history maps. These diseases demonstrate what may be referred to as a reversed hierarchical mode, a term introduced in my thesis on cholera disease migration and the Oregon trail.
In reversed hierarchical disease in-migration habits, the disease comes in and infects borderland regions, but due to the nature of the disease to become increasingly epidemic in nature thereby infecting larger numbers of people, it tends to migrate into the core of the local population area, from where it then takes a more aggressive route outwards, either as a Type I migration pattern spreading spatially in all directions, or as a Type II pattern following principal transportation routes and setting up new niduses each time it comes in contact with a new high population density region. A third type of disease diffusion or migration pattern, Type III, is a combination of these two events–usually beginning as a type I and then progressing into a type II, but sometimes vice versa.
.
.
Zoonotic Diseases
Almost every domestic animal in the United States came from another part of the world. This is particularly true for most of the commonly bred and marketed farm animals. When Chancellor Livingston began developing his lands in and around Clermont to its fullest economic potential during the 1790s, he engaged in large amounts of fruit tree and vegetable farming and raised livestock. He added to the value of the farm setting by introducing sheep farming to the Hudson Valley region of New York around 1795. He also developed the first research and experimental livestock farms engaging in breeding practices and research and to the first formal experiments on the development of new crops and animal breeds. Livingston was the first President of the region’s agricultural society, its purpose was to monitor animal and crop productivity and at times oversee any legal decisions or changes that were made in this young industry in New York State.

The first diseases reviewed during these early years of livestock farming were those specific to animals. The journal in which the majority of these findings were published was the Medical Repository published out of New York City by Samuel Mitchell.
.

see http://science.howstuffworks.com/anthrax1.htm
The first important enzootic disease in the Hudson Valley was the horned cattle disease known as Anthrax. This disease had minimal effect on people during much of its history as a disease. It did however have a major effect upon the economy. For this reason, counties which are major diary products providers considered this disease one of the most important public health issues for the time.

Sequent Occupancy
We can apply some of the more popular medical geography concepts to studying veterinary diseases by using the basic time-space relationship defined by sequent occupancy theory. Sequent occupancy is used primarily to define land use changes over time for a specific region or community setting. Whereas industrial and domestic related features are often the focus of this way of interpreting land use patterns, extending these applications to include public health and epidemiology issues results in some very useful applications of this geographical concept. In terms of analyzing the place-time relationship between disease, people and the environment regarding animal disease in relation to people’s health, sequent occupancy works very well with improving our understanding of zoonotic and anthroponotic health.
Once again, sequent occupancy plays a very important role in understanding animal health, applying human epidemiological theories to zoonotic studies.

Epidemiological Transition
Epidemiological transition differences from the sequent occupancy philosophy in that it includes some very broad-based assumptions and observations. Features specific to space are not brought into perspective in any human ecological way other that through a focus on the basic demographics and most sociological definitions for people, populations and health. Epidemiological transition theory does take into account income and certain other census-related data such as life expectancy, birth and death rates, fertility and maternal statistics, but the interactions of people with their environment is limited in its review. One can state that people within a given population are more likely to experience certain kinds of diseases associated with a specific income and economic development setting. The epidemiological statistician employing the contemporary manner in which this theory is reviewed does little to relate exact cause and effect in many cases. Such a researcher can provide details about how epidemiological transitions processes impact morbidity and mortality, such as obesity and diabetes anf the urban setting related asthma and autoimmune diseases.
When it comes to providing a detailed human ecological and environmental health perspective on similar diseases and the numerous diseases that are propagated within these environmental settings, one needs to involve a more detailed environmental health, sequent occupancy type of approach to reviewing disease history and patterns for a a given place. Sequent occupancy tells the research when a where certain illnesses and medical, events occur, and why they occur. Epidemiological transition is more a broad theory used to define overall population health related features with little consideration of the detailed make up of that populations and its own internal stages of economic development and transition that result in most of these human population settings.
.

Much of our understanding of animal-related disease behaviors has been a product of western European medical thinking. This changed during the 1980s when Mikhael Gorbachev took office and in time converted the USSR into a more democratic-like country. These changes enabled bilingual English-Russian speaking scholars to begin researching and discussing regularly with scholars of the Socialists Republic about their knowledge and intellectual property. This led to improvements in our understanding of a very well known method of interpreting disease ecological patterns that was created and first promoted by Evgenus Pavlovsky.
Pavlovsky’s method of reviewing diseases spatially were utilized by Voronov during the latter decade of Pavlovsky’s life in the university setting. This enabled Voronov to further improve upon Pavlovsky’s methods for modeling disease ecology in relation to surface topography and weather. In essence the accomplishments made by Voronov consisted of a number of substanital improvements upon the turn of the century way of visualizing disease and man published by Pavlovksy. Voronov was to Pavlovsky like Carl Jung was to Sigmund Freud. Voronov put Pavlovsky’s perspective on disease geography into the more modern perspective needed by conteporary GIS-savvy spatial epidemiologists and medical geographers.
Bioterrorism
The most important application of this analysis of the historical map is its relevance to the current concerns related to bioterrorism. One of the most common threats considered with bioterrorism pertains to the introduction of foreign domestic animal diseases and the impacts of these diseases on the food chain. For decades, we have traditionally reported on livestock deaths and typically required that physical autopsies and numerous laboratory tests be performed in order to avoid the develop of a crisis. The contagious lung plague of cattle is one of many diseases that pertain to this particular zoonotic epidemiological GIS topic. This topic as it relates to bioterrorism is covered further on another page.
END NOTES & RELATED TOPICS
Pavlovski and Voronov
http://www.zin.ru/contributions/N06/index.html
http://eurekamag.com/keyword/i/151/interepizootic.php
Epidemic=Epizoonotic in that zoo infers animals, demos infers people.
Endemic=Enzoonotic (ditto)
Axenotic=without foreign (esp. zoonotic) influence (zoo~xeno, in that xenos~foreign)
Metaxenotic=with foreign influence and change. Foreign implies outside the central ecological setting for the disease, or its direct cause. Foreign influences can be carriers and vectors with spatial distributions extended into other territories, where the pathogen or organism directly responsible may be absent.
…
Related research questions for New York Hudson Valley history:
how did Livingston’s plan with Clermont affect local zoonotic disease patterns, ESP those related to Sheep? Agriculture? Horn Disease?
Rat-induced Plague – Typhus?
Vector born diseases?
Mosquitoes and Flies–Malaria, Yellow Fever and Cholera?
.
From Chamber’s Encyclopedia, vol. 11 (Plattsburg to The Ten Persecutions)
PLEURO-PNEUMONIA (ante). Prof, James Law, of Cornell university, in a recent work gives much valuable information on the pleuro-pneumonia of cattle, or, as he thinks it should be called, contagious lung plague of cattle, which answers to the German name lungenseuelle. He gives as a definition of the malady, a specific contagious disease, peculiar to cattle, and manifested by a long period of incubation—ten days to three months—by a slow, insidious onset, by a low type of fever, and by the occurrence of inllammation in the air passages, lungs, and their coverings, with an extensive exudation into the lungs and pleura. He says that the nature of the disease has been misapprehended by many authorities, especially among English veterinarians, and that there is no proof that, like other inflammations of the organs within the chest, it is caused by exposure, inclement weather, changes of climate and season, imperfect ventilation, overcrowding, etc. He says that the malady “is always and only the result of contagion or infection,” therefore he proposes the name above given. He has, however, no objection to the old name, pulmonary murrain, giving an account of the disease as it has appeared on the eastern continent, in which he makes the statement that Great Britain alone has, since 1842, lost not less than $10,000,000 per annum by the ravages of the disease, he gives a brief notice of its introduction into the United States. It was brought into Brooklyn in 1843, by means of a ship cow, bought by Peter Dunn of the capt. of an English vessel. From this cow it spread rapidly over the whole west end of Long Island. The plague was introduced into Massachusetts in 1859, by four Dutch cows, imported by Mr. Chenery, of Belmont, near Boston. They were brought from the infected port of Rotterdam, and were forty-seven days at sea, during the last twenty of which they were sick, one of them being unable to stand. On landing, two walked to the farm, while the other two lied to be carried. One recovered, and three died, the last one the 10th of June. On August 20, another cow of the herd took the disease and died in a few days. Several others followed in rapid succession. Then Mr. Chenery became convinced that be was dealing with the bovine plague of Europe. He lief unfortunately sold some calves to a neighbor on the 23d of June. The disease spread, and during the next four years infected many counties. In 1860 a state act was passed to provide for the extirpation of the disease, which empowered the commissioners to cause all cattle in herds where the disease was known or suspected to exist to be killed. The commission was kept in existence six years, when the last member resigned, the disease having been exterminated. The malady was imported into New Jersey in 1847, by Mr. Richardson, who, as soon as he ascertained the fact, had his whole herd, valued at $10,000, slaughtered. But others who had diseased cattle were not so public-spirited. and the pest was carried into Pennsylvania and Delaware, spreading into Maryland and Virginia, where it still prevails. The disease may be communicated by immediate contact, through the atmosphere for a considerable distance, by the inhalation of pulmonary exudation when placed in the nostrils, from the impregnated clothing of attendants, infected buildings, infected manure, pastures, fodder, etc. Pastures grazed three mouths previously have communicated the infection, and it has been spread by the flesh of diseased animals. In buildings which contain piles of lumber, litter, and hay, the virus may be preserved some considerable time. The distance through which the infection will pass between separated cattle varies. Herds separated not more than 15 yards, with a tight board fence 7 ft. high between them, have been known to be unaffected for over six months, while the infection has been conveyed much greater distances. The disease is confined to the bovine genus, and all its members, irrespective of age or sex, appear to be equally liable to its attacks, and, as in many other contagions diseases, those animals which have once had the disease are exempt from future attacks. The period of incubation is variable, ranging, according to authorities, from five days to three months; and it is this insidiousness which renders the disease so dangerous. It, however, develops much more rapidly in hot than in cool weather, and in the south than in the north. The work of exterminating the disease in New York by Gen. Patrick and Prof. Law was, at the commencement of 1880. as follows: Ill the preceding ten months the inspectors in New York had examined 40,000 head of cattle, many of them several times. They had paid the owners for 500 head of slaughtered cattle, which nearly eradicated the disease from seven counties. At that time the center of the plague was in Kings county, and the adjacent borders of Queens county. In all the country districts where the cattle were kept on inclosed farms, the work of exterminating the disease was comparatively easy. In the suburbs of cities, where cattle were allowed to graze on open lots, the greatest difficulties were met. More difficulty was found in Brooklyn than in New York, because of the greater opposition to the work of the inspectors. In Putnam co., where the disease had been smoldering for more than a year, the county authorities authorized the extermination of every herd known to be infected.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave a comment