Posted by Brian Altonen, MPH, MS under Uncategorized Comments Off on 2023
There are several innovations in my research approaches worth reblogging here. In particular, the numbers of people citing my work in their various fields are quite gratifying. Mind you, some of these mentions involve work that is over 20 years old. But that’s fine. Better late than never, so they say.
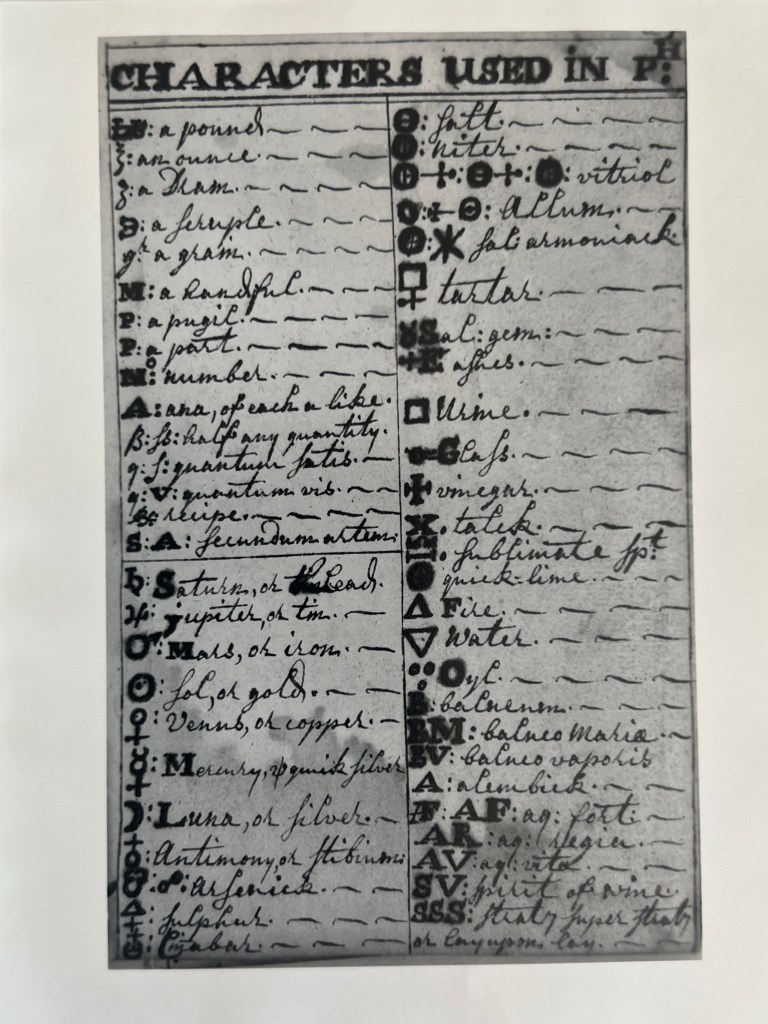
The study of Colonial Medicine is the theme for these items posted.
The first document comes from an original copy of a thesis that I purchased in 1990. It is the work of a MD program student from Yale, on a document found at Mystic Seaport museum. It explored an original document kept by an apothecary-physician from England, dated 1720, four pictures from which are posted here.
The second item is a slide presentation on physicians of the Hudson Valley, prior to the Revolutionary War.
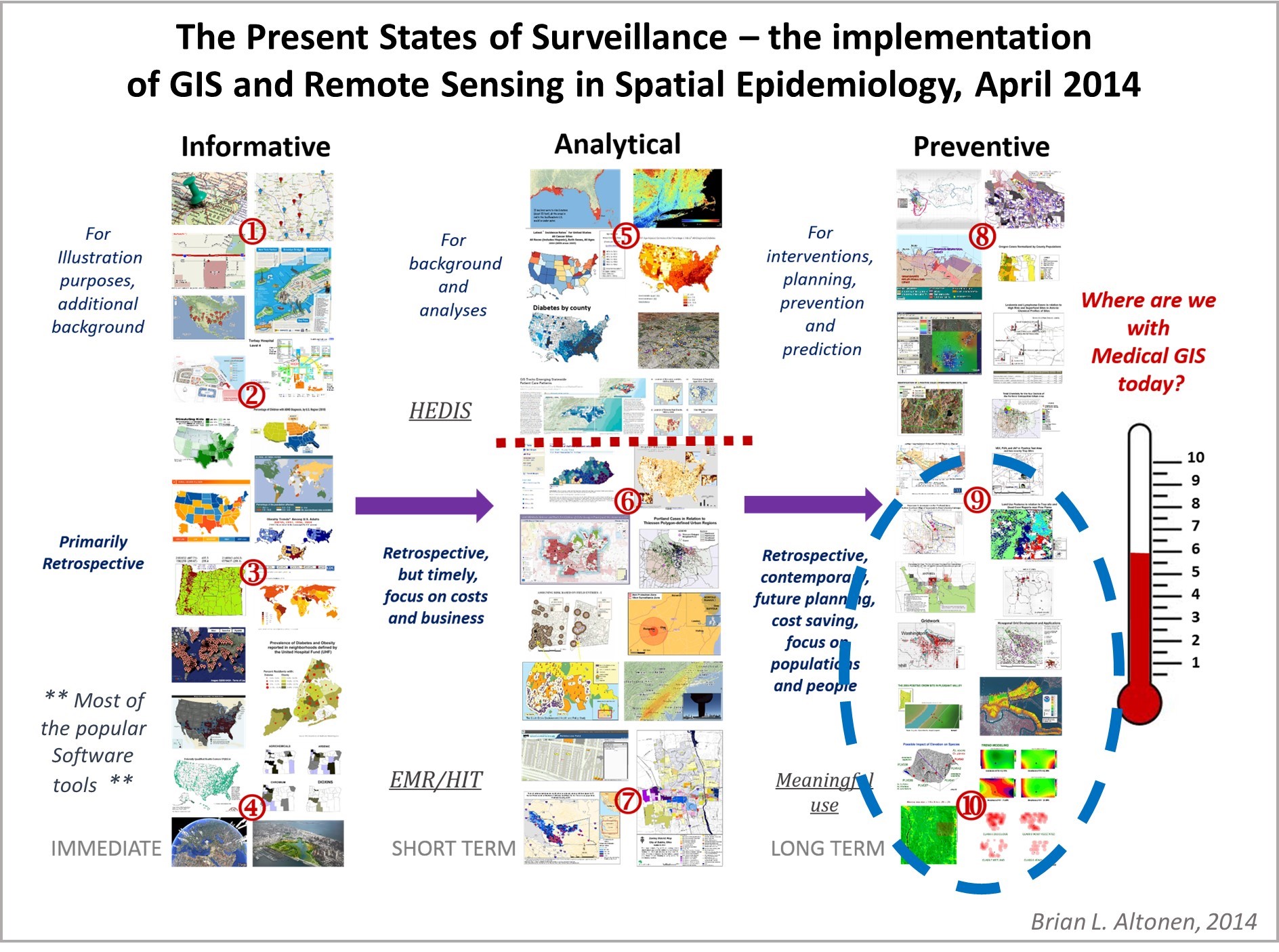
I designed a way to score health care programs for their GIS savviness using this scoring process, which evaluated the different spatial modeling software tools, methods of analyses, mapping processes, applications of GIS use, types of GIS (point, raster, vector) employed for surveillance and public health monitoring. This survey ran from 2015-2019 and focused on the use of GIS by Health Care Organizations and Facilities.
Middle of Outbreak update.
A number of historic epidemiology researchers, like myself, have stated that more than three years is a lengthy stay for a pandemic event. The ways that yellow fever and cholera tended to stay, and re-emerge, was in two or three year clusters during the late 1700s and 1800s. Each had varying numbers of years apart between their cycles, a source for our reasoning.
The first tendency is to look at past epidemic history and try to assign some sort of natural…
Posted by Brian Altonen, MPH, MS under Uncategorized Comments Off on Returns . . . on Investments
Patience helps.
In health care research, we engage in projects that we usually want to see immediate benefits from.
Those benefits include the completion of a project, then witnessing, documenting and “proving” any changes it is responsible for, then seeing these results published in the literature, either something as simple as a news story or article about your work, or the publication of presenting your results in a public and/or professional media, or the printing of a complete review of your work, either by yourself or by a colleague who appreciated it, and who became the first individual to employ what you have discovered.
I have certainly experienced all of these signs of appreciation for my work over the decades. My work on history of plant medicine put me on the television screen as far back as the early 1980s, in the largest newspaper at the time in Long Island, NY, and in innumerable books, newsletters, monthly mailings, education materials devoted to some aspect of local medical history, in New York, and of all places, Oregon, where I spent 20 years building my repertoire in accomplishments, working as a professional and university professor who called his specialty “Medical Botanist and Historian”, for 20+ years.
It was in 1994 when I decided to switch my focus from teaching plant chemistry in a university chemistry department as my specialty, and researching medical history as my second specialty on the side, to studying the underlying geography of these things in life. Interestingly, I went in geography and spatial analysis because of my theories about how and why plants formed their unique chemical products. This theory of mine remains active in the field of phytochemistry. I needn’t search the web far to find individuals, scholars or not, employing one of more of my various theories about how plants form their useful chemicals, or why they do, or how these products came to be and undergo change as a part of the human geography evolution ecology theme, or how and why some become popular before others–the nature of human philosophy and logic, and how medicine relies so heavily upon these relationships we define, for what we learned and “know.”
I came up with theories for how and why plants evolved cancer drugs for example. Easier to understand is the theory as to how plants learn to divert certain chemical pathways in new directions, so as to convert their common chemicals in one specific group, into a new type of chemical formed when two uniquely evolved pathways get merged, into one, and for the first time produce a chemical novelty, important to their survival, yet more important to mankind, or their local ecosystem.
So, all of this thinking and intellectual reasoning was applied to plant medicines and most other ethnobotanical products, and then to a unique interpretation of this theory in relation to what plants existed in certain places, leading finally to my interest in the use of geography and spatial analysis to look at these concepts. One could use topography and spatial technology to map out plants in an area prone to wildfires, like I did for the Tillamook burn area in Oregon; one could then apply that to the chemistry of plants that might aid or even make the plants of that region exceptionally prone to initiating and then effectively spreading wildfires over time. With spatial analysis, and combined plant chemistry geography studies, I could see and write about the parallels that existed between this small part of Oregon, and the much more aggressive wildfire areas seen elsewhere around the world–the main one was in China, due to the “Yang” aspects of the mountains with forests, according to their local philosophers/geographers. Chemically and environmentally speaking, according to a geographer’s or spatial analyst’s mindset, this reasoning did have unique meteorological based reasons as well.
Then came my interest in how certain disease causing insects could survive in only certain places, and the pathogens they might harbor. Hanta Virus, Lyme Disease, “Malaria”, were famous diseases, for which I could learn this use of spatial analysis and geographic information systems, GIS.
At the time, I was working out a concept for which I could write my required thesis about. My mentor was kind of a ‘Jack of all trades’ in his field. He was the one who convinced me to apply to Portland State for my work in Geography–“not more of that pure science!” he would say to me. “You have to see the entire picture!”
The second forte of this professor. Larry W. Price, was medical geography. His most unusual, popular book, was also famous worldwide–Mountains and Man. He wrote the “bible” for today’s athletes, who were most devoted to tackling the high elevation parts of the world. He recommended I think about medical geography, and forwarded me to some famous writers on this subject who were “geographers”, not epidemiologists or ecologists.
Medical Geographers kept me out of the scientific realms enough to begin to think about other interpretations of health and disease, and the human environment. The added that “social Darwinist” aspect to the field of epidemiology research, which, to tell you the truth, I really wanted to stay as far away from as possible at the time. It’s interesting to study human behavior, sociology, sociocultural aspects of health. It’s another thing to study things you do not normally think about when learning science, at least back then. The Marxist interpretation of human behaviors and foodways for examples, and how capitalism is the cause for terrible modern diseases of the heart, lungs, various solid organs, and all those tissues that develop cancer today. What they hay!?
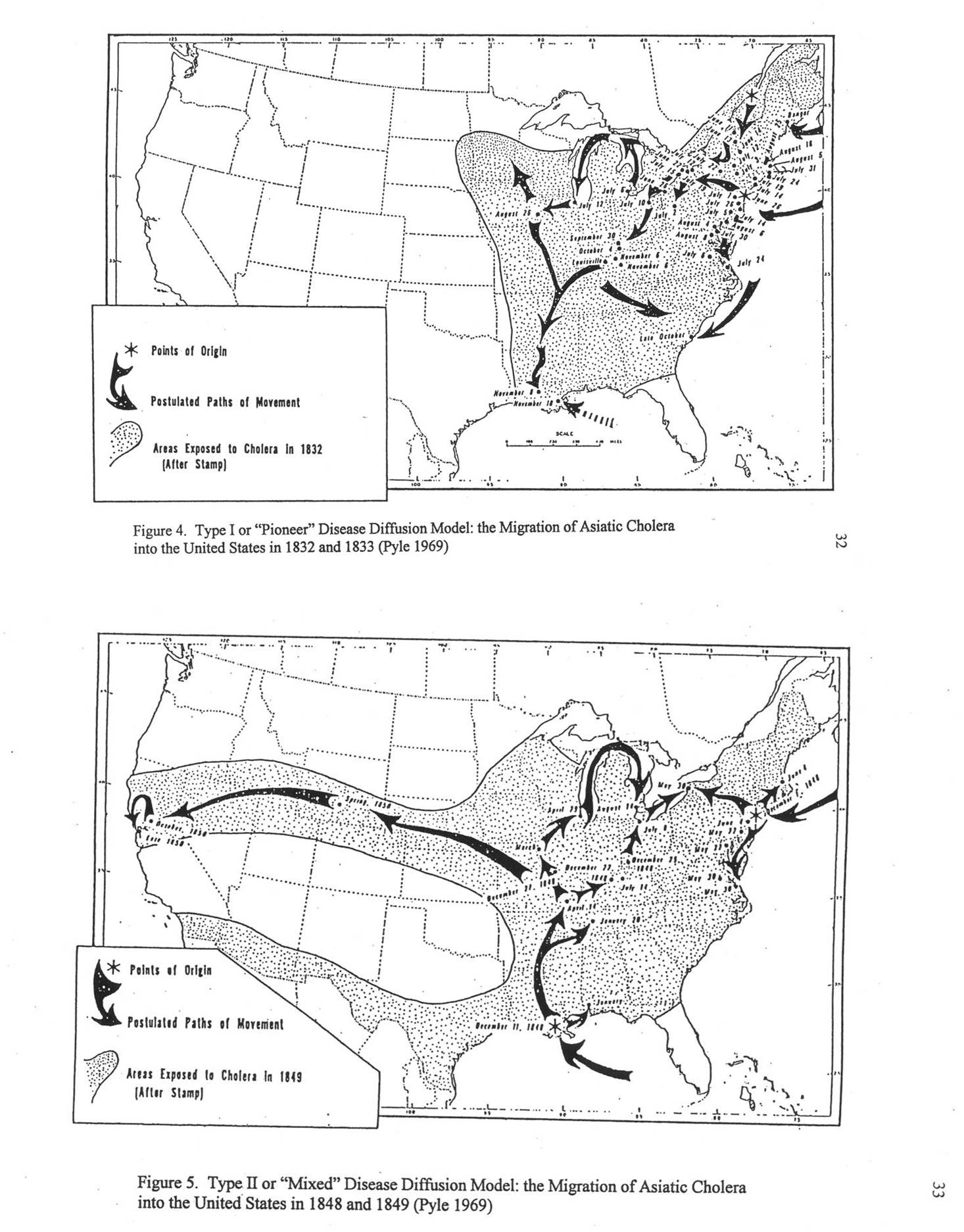
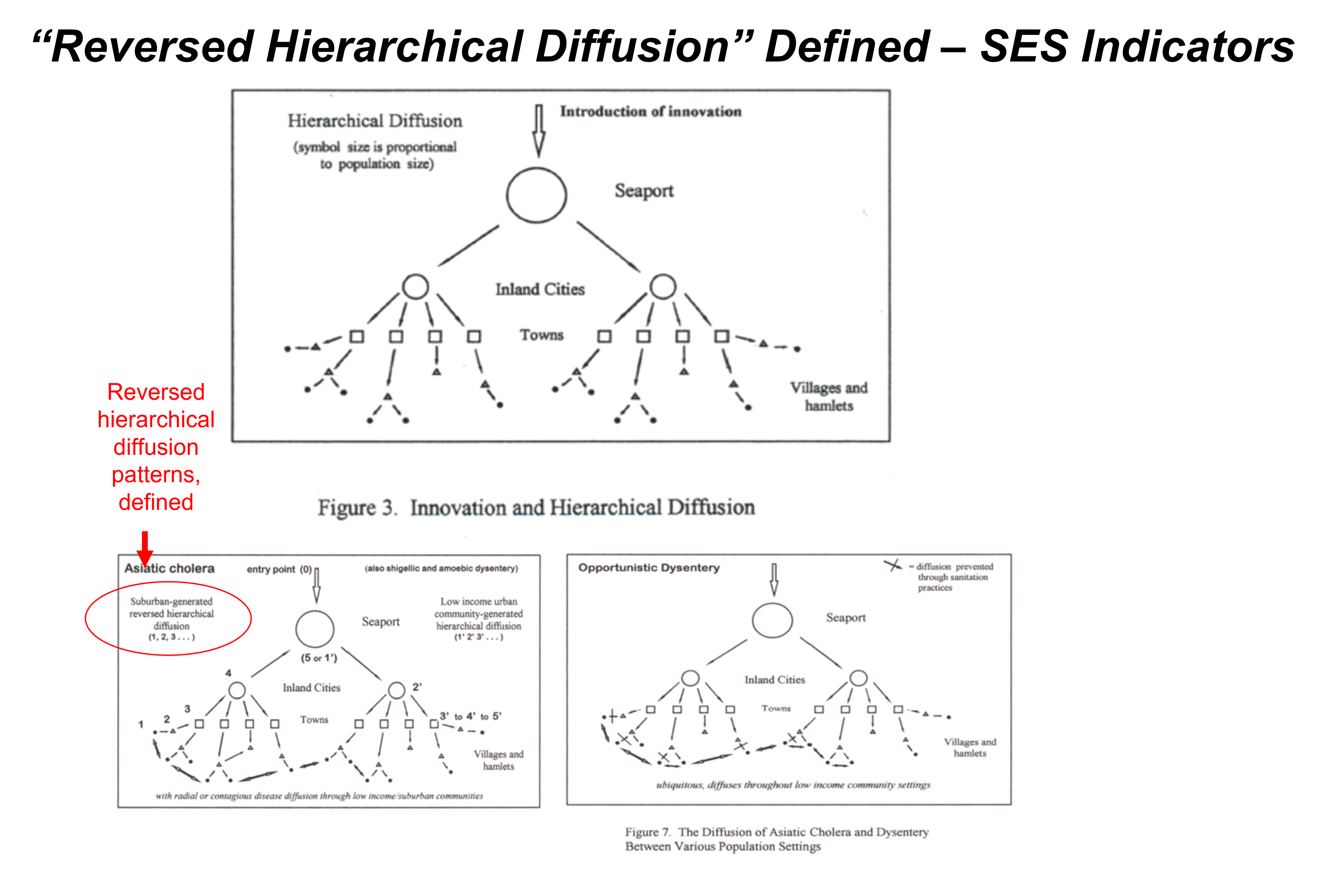
The early socialist interpretations of disease patterns and behavior are exactly what we need to consider when interpreting disease patterns today–which is what we do in medical geography. My review of the other interpretations of things have to do with epidemiology, which I learned twenty years earlier after several years of medical schooling, enabled me to develop another view of what they traditionally taught in medicine. This was my impetus for studying the epidemics along the Oregon Trail, in the way that medical geographers interpreted its outbreaks during the early to mid-1800s, as the disease made its way into the United States, and then across to the Great Plains, and finally partway along the trail heading towards Oregon. ‘Why did it stop? Or didn’t it really stop?’ These were the unanswered questions in the literature about Oregon Trail history, and in the medical writings for the time, from about 1839 to 1859. My goal was to go through as many historical writings as I could about Cholera on the Oregon Trail, define which of these were Asiatic Cholera and which were simply several diarrhea, or dysentery (amoebic or not), or opportunistic dysentery, or some other fever-generating, dehydrating, sometimes fatal disease brought on by the fatiguing nature of traditional overland journeys.
Disproving the complete diffusion of Asiatic Cholera westward along the trail wasn’t hard to do. But defining what caused the cases of diarrhea and occasional deaths required a thorough review of cholera-like diseases–like I mentioned in my defense of my thesis, August 2000, my study is more appropriately called, “the Geography of Diarrhea”, a section I had to write up for the Appendix of my work.
Present at the defense of my thesis were two colleagues. One was a pathologist, genetic engineer who worked on pathogens at the local CDC lab in the basement of the chemical building where I taught classes on phytochemistry, for twenty years. The other was my future colleague at the time who was deeply interested in the possible use of a full GIS for disease research. Our next three projects we received grants for as a team at the University, School of Community Health, were all devoted to disease ecology and GIS, environmental science and cancer, and socioeconomics and public health, all using GIS.
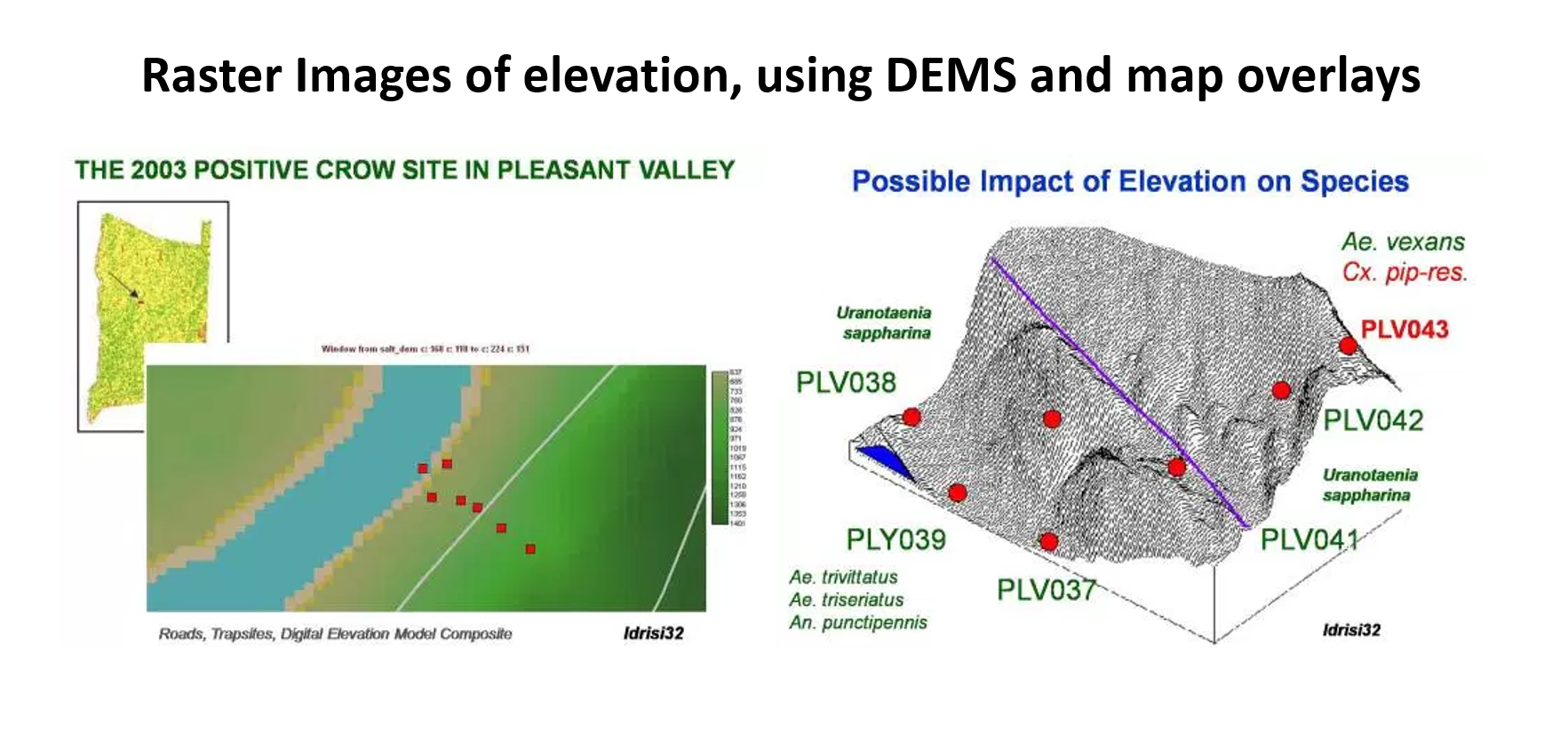
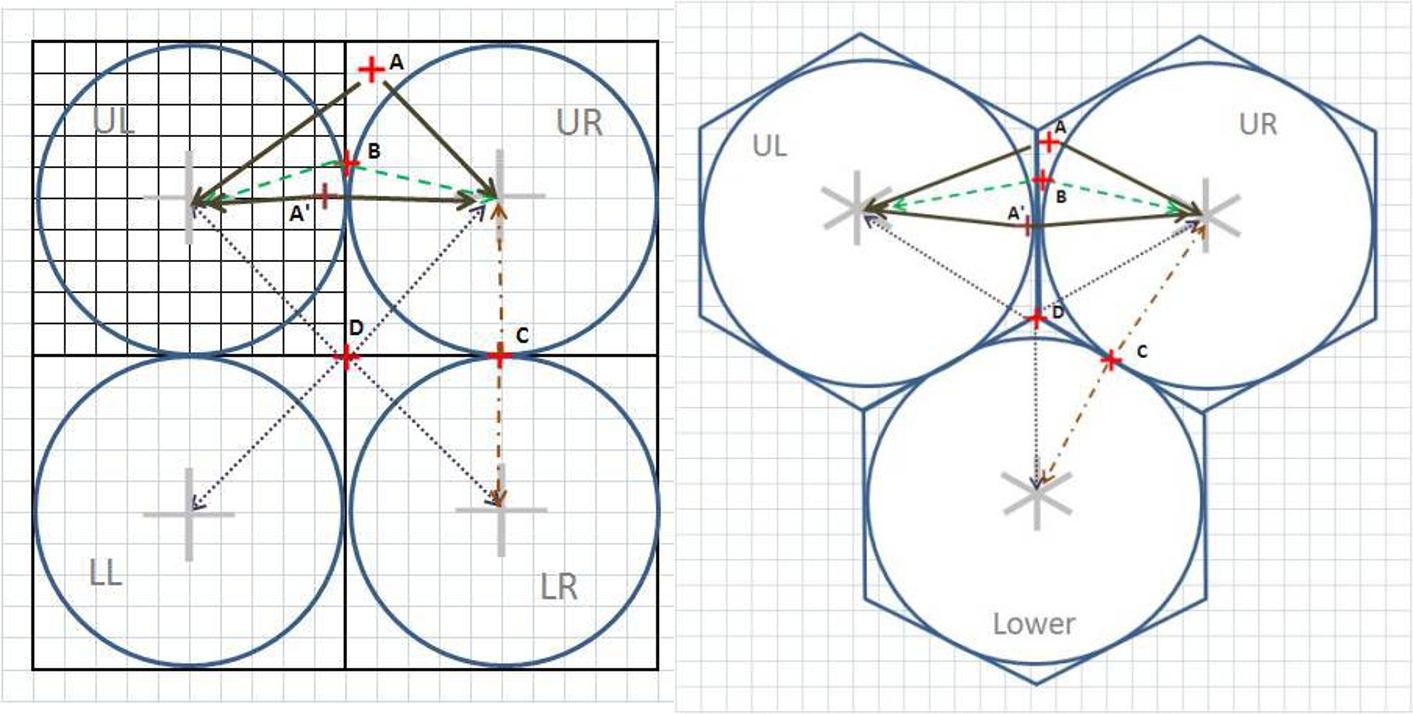
When west nile struck this country in late 1999/early 2000, we had initiated out lyme disease ecology project. Next came the more successful grant funded study on environmental chemistry, exposure to benzene at Superfund sites, and my development of a series of methods to explore the chemistry of these well documented chemical release sites, and to explore the content of each setting, relative to numbers of local cancer cases being documented in the state’s new disease registry. In this project, winter of 2005/6, I saw the need to replace square grid analysis with hexagonal grid analysis, and so developed the math needed to identify the points needed to construct a beehive/hexgrid display on my basemaps. I did the math to demonstrate how and why this math produced a more accurate centroid-specific map for which to analyze spatial units with (instead of the moving circles windows, which only defined “hot spots” one circle at a time).
As a number of my other pages review, I developed this methodology at the national level, covering the entire U.S., using a database that detailed the health histories of anywhere from 40 to 90 million people in the US. The base data for this database was zip codes. I developed the first national maps as zip code area maps of US statistics, and since ICDs were included in this database, I focused that work on ICDs, ICD groups, and any combinations of ICDs one could pull together, in order to map out where disease, for example from Japan or China, were found in the U.S.; how west nile was distributed relative to the two mountain ranges, on a per zip code basis, where certain sociocultural or human behavior diagnoses tended to cluster, like in certain rural versus heavily populated urban settings. This later was converted to a hexgrid mapping algorithm that I developed. (But the zipcodes maps tend to be more visually pleasing and applicable to real life intervention programs).
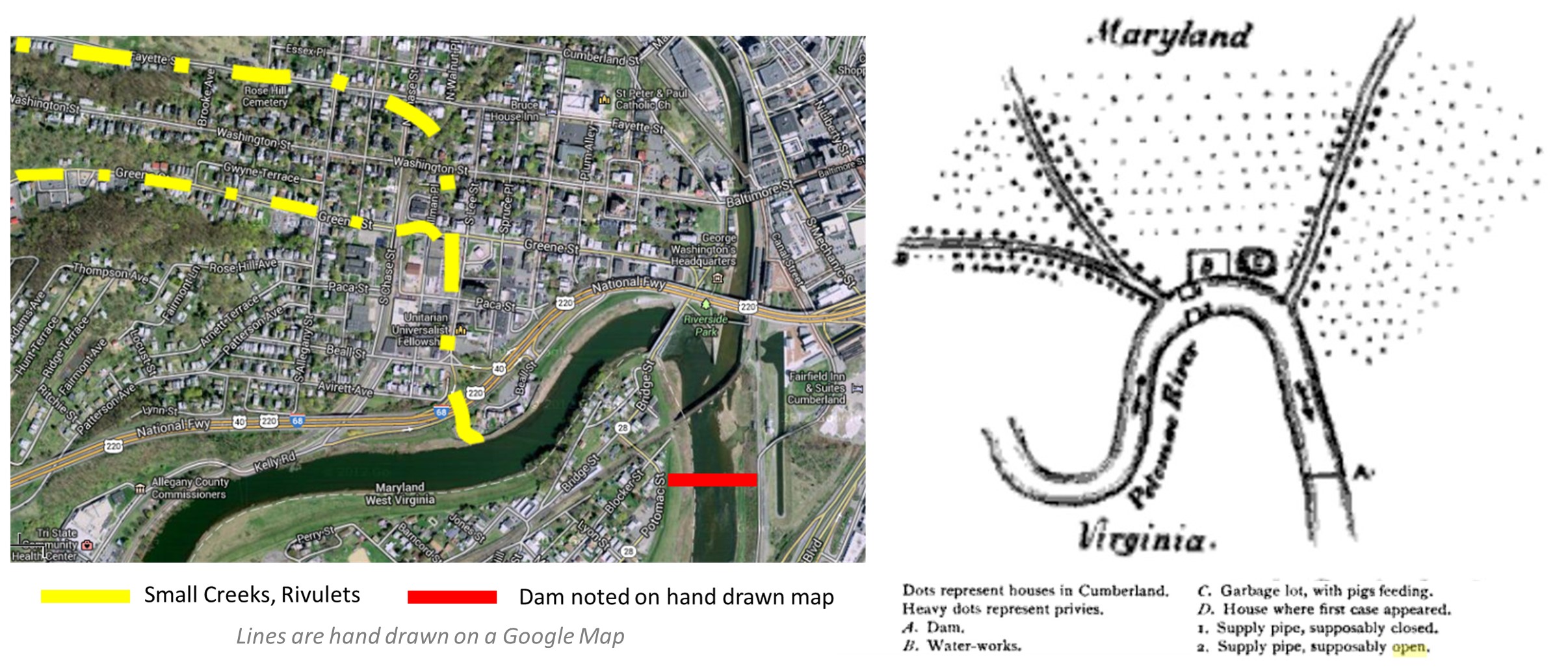
My recent work has enabled me to develop this work to a smaller area level–the neighborhood or street level, if I want to.
So, what are my returns of investments?
You can look at the development of these return s as simple “OCD”–obsessive compulsiveness–in other words, it ain’t over until its over.
The most amazing example of this happening pertains to the twenty years it took for me to first remember, and second know how to go back to a decades old research question, when the answer to that question finally appear in the literature. This event is when the source for a local New York physicians 1763 recipe of an alchemy nature was uncovered by a scholar researching very old manuscripts in Oxford around 1990. That opened the door to my continuation and near finalization of understanding the decade by decade history of medicine in New York, from about 1600 to 1850.
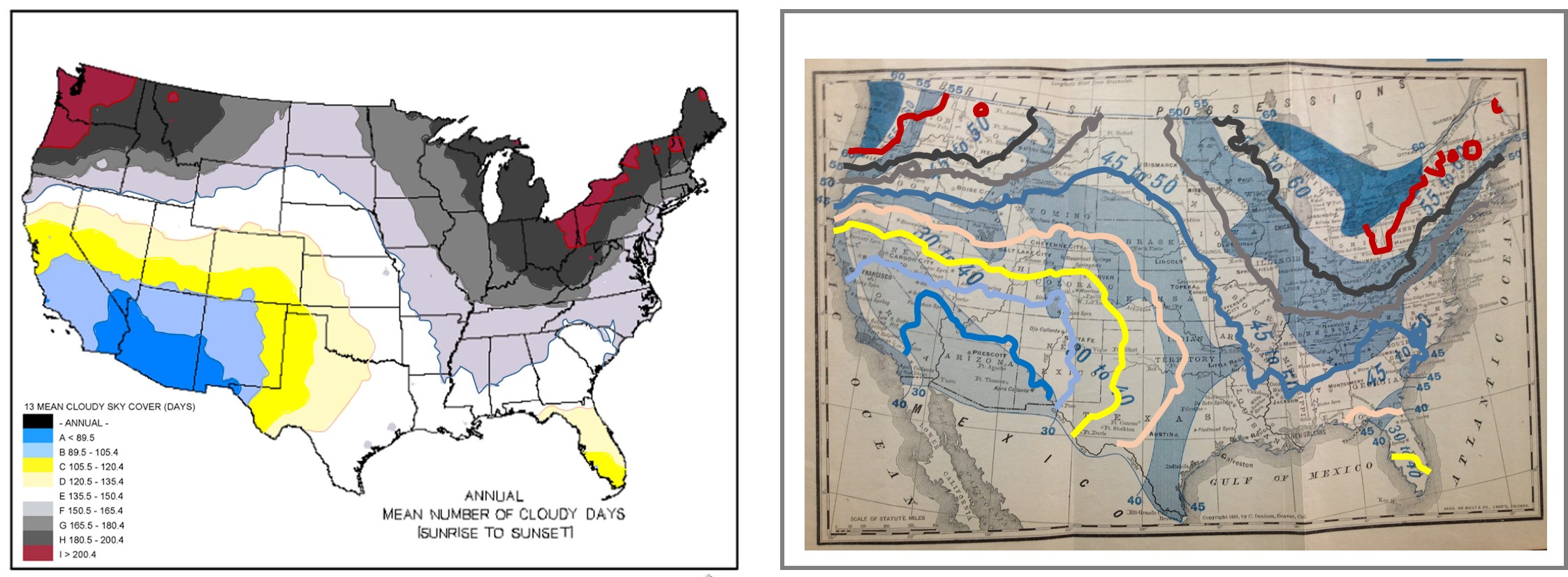
My luck with uncovering the original copies of the old medical geography maps of the world was a second set of discoveries helping me through my research endeavors. In particular, a lot of maps were published in local medical journals, or as their own essays by the same publisher, and these booklets were very common to the mid 19th century. Reviewing these maps provided important insight into how diseases were interpreted topographically, climatically, latitudinally.