(c) 2006, 2010 Brian Altonen
HEDIS-related Prescription Drug Use Measures
Introduction
During the winter of 2004/5, I developed a method to review the national script database known as the National NCPDP Pharmacy Database. This project was developed simply to identify moderate to high risk asthmatics based on the counts of asthma/copd scripts per year, and to develop a way to monitor average costs per script per dose per day per individual on the medicaid program. this hopes was to monitor these costs over a period in order to develop a program that would popularize internal pharmacy use, where costs per script were lower, in place of the typical local pharmacy. This evaluation of the data revealed several other issues pertaining to cost, a number of these having to do with several of the PIP/QIA activities I was engaged in.
The purpose of this review is to define the methods of analyzing large pharmaceutical datasets. For the projects defining the need for this review, script information was reviewed and compared on a quarterly basis, resulting in summaries extending over the past 12 months or longer. This dataset was also used to evaluate script histories as they pertained to a number of HEDIS-related measures, such as the use of certain medications by patients with diabetes, hypertension, hyperlipidemia, moderate to severe asthma, chronic behavioral health conditions, chronic infectious disease, etc. The National NCPDP Pharmacy Database provided me with datasets as lengthy as several hundred million rows, depending upon how the data was requested, and how subgrouping methods were used to subdivide and reanalayze prescription drug data.
The NCPDP database offers about nearly 100 methods to subcategorize your prescription data when you are requesting summaries of your query results. These subgroups divide the drugs down into classes based on their pharmacological activity, the physiologic system they influence, their NCD based categories, their various numeric identifier, etc. The broadest classification of these drugs used in NCPDP consisted of 12 to 15 groupings with group names provided in text form; the largest subclassification program involving word textform broke this information down into nearly 500 subclassifications. Following a number of attempts to better understand these various subclass routines, it was determined that best classification systems to use fo many studies seemed to have between 100 to 250 subclasses. This kept the new datasets produced using these queries fairly detailed, but not so exceedingly lengthy as to increase the runtime or work effort needed to make the best use of this data. In the end, a number of methods of applying subclasses for the drugs related to PIP/QIA work ranged were developed, producing several million script-related summaries and counts per query.
It was this form of the data that enabled me to define a use of this information for evaluating HEDIS like information as it related to script data. These measures typically included well documented HEDIS measures with one or more components of the work based primarily upon script counts and types. This included measures like determining whether or not a particular form of medicine was administered to a patient, whether or not a particular type of medication was avoided due to its history of overprescribing, or whether or not a given script was underprescribed or underutilized due to non-compliant patient activities.. In the end, about 25 HEDIS or HEDIS-like measures were identified and evaluated for potential use of script data. This review provides the background needed for researchers to define various ways to make better use of an otherwise underutilized database with high potential for application to PIPs, QIAs and HEDIS QA projects.
A Review of the Methodology
The following methodologies were described for comparing in-house methods of monitoring population health and non-provider/non-health care service methods of monitoring population health. The first method illustrated below is the standard method by which HEDIS and NCQA steps are taken to carry out Quality Assurance reviews. This is a pretty simplified method of detailing the actual steps taken in program to develop algorithms for accurately carrying out reveiws of particular patient populations. It essentially demonstrates the order of steps taken when defining the health of each individual within a database.
When we compare the in-house method of reviewing medical data to a non-institutional method of review, we notice that the focus has to be primarily on the script history, from which a medical status is defined for each individual found in the datasets provided. The task then become trying to merge this information with other information sources available within an outside corporate work setting, focusing primarily upon claims records instead of clinical records.

One of the most effective ways to develop this research program is to abide by the standards and/or guidelines already established for performing such analyses, modifying these methods whenever the need arises in order to produce a project fairly similar to HEDIS methods already approved for such uses in a general sense, with internally define additional steps taken to be certain of the new methodology to be developed.
The following is a complete list of the HEDIS measures established for 2010.




A number of HEDIS measures have potential application to the development of methods for monitoring prescription activity, using a methodology focus on script counts and amounts, in conjunction with medical hostory data provided by claims documents that include ICD codes in their entries. Those studies most related to this approach for monitoring physician-patient script performance are summarized in the following table:

Notice there are two avenues taken to evaluating script use in relation to HEDIS measured clinical events. There is the proactive method of evaluating individuals, in which medications and activities engaged in are designed to improve QOL and reduce chances for morbidity due to a particular illness. There is also the reactive method of utilizing drugs for medical reasons that can be monitored, activities which involve the misuse and abuse of prescription drugs, along with the underutilization or skipping of doses for certain medication due to passive non-compliance reasons or intentional non-compliance reasons including voluntary avoidance such as deliberately skipping a psychiatric medication. An additional use for these types of measures in need of review pertains to illness-related procedures engaged in for maintenance and preventive purposes, such as monitoring blood glucose levels on a regular basis, or the frequency of use of nebulizers to assist in reducing severe asthma related events. Another example of such a study included a review of nutritional supplement use by pregnant women, as a measure added to a HEDIS-related activity focused on pre-natal/post-partum care quality.
Such uses for prescription data have broad applications to already present HEDIS-related internal studies already put in place. A number of these HEDIS-related activities have at times been considered “optional treatments”, that is to say they are not a necessary part of any standard HEDIS/NCQA measure, but are often included in HEDIS/NEQA measures. Example of these include reviewing whether or not a patient obtained a prescription to assist in the cessation of smoking or taking a medication designed to treat some chronic disease or condition with well-documented long term financial and QOL consequences, such as insomnia, GERD, fibromyalgia, alcoholism, MS, RA, lower back pain, and numerous other chronic medical conditions of health related problems.
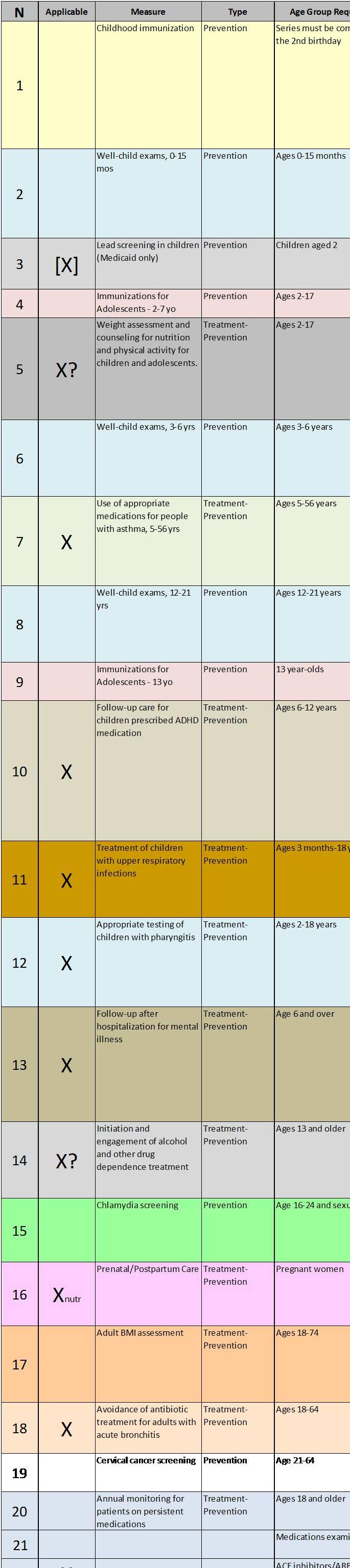
The following figure depicts the age ranges for all 2010 HEDIS measures. The x axis represents age in one year increments (range 0-100), with blue bars representing the years of age during which a patient eligible for a given HEDIS study. The name of study is noted in the second column on the left. The first column of data indicates whether the HEDIS measure may be considered primarily preventive in nature, such as a breast cancer screening measure, or a measure that represents a combination of therapeutic/reactive and preventive medical events (i.e. diabetes studies test number of visits, HgA1c>7.5, yes/no for ophthalmology visit, yes/no home monitoring practices, htn present, htn medication in use, whether patient is insulin dependent or not, etc.).

The bottom most graph illustrates the numbers of HEDIS measures by age, on a per year basis (red line), accompanied by a count of the numbers of measures with some sort of script data relationship. Notice the patient population of <18 years of age is the hardest group to obtain a large number of HEDIS-related measures for. Any review of scripts history for the purposes of performing HEDIS-like or HEDIS-related should therefore focus more upon this particular high risk age group. Through a review of the entire script history of a Medicaid, Medicare, and employee health population back in 2005 (N_total = 65K-67K , 200M+ scripts), the best way to evaluate these patients and their health status using prescription data required the use of a standardized recoding proccess for the claims dataset, in combination with lengthy reviews of other data sources pertaining to demographics data. The potential exists for developing an adequate number of measures involving all age groups in the given population. A stronger emphasis needs to be places on the one low presence study group, patients <18 yo.
Conclusion
Approximately 25 very specific HEDIS-related measures were identified that can be related to population health prescription data. These measures can be supplemented by 15 to 25 other measures of similar methodology to evaluate other aspects of population health non monitored by the general HEDIS-based series of measures. These measures are on occasion also performed automatically as a part of the automated HEDIS measuring system, such as a number of general measures focused of prevalence of a variety of infectious diseases. One additional measure was defined elsewhere in my review on this topic: individual <18 years old, especially children 10 to 18, could be monitored for STD-related matters. Whether or not this can be evaluated pharmacologically in uncertain. Another pharmacological method of evaluating this age group may have simply to do with use of prescription antibiotics, with this analysis broken down into subparts based on the chemical classes (generations) for each of these of scripts provided. In the case of chronic disease management, there are a number of chronic diseases with well-defined drug protocols. These too could be monitored. Another important preventable issue that could be better managed through evaluations of script data pertains to post-op iatrogenic complications, in particular infection onset involving Staph-resistant strains and Antibacterial-resistant Clostridium. Since many of the drugs used for these types of infections are often high cost, methods of evaluating this particular public health problem could result in substantial reduction in overall costs.
In sum, there are a number of Post-HEDIS avenues to take when supplementing the HEDIS-based review methods with new and inventive methods for analyzing prescription drug use in order to identify potentially high-risk patient types and reduce to overuse of high cost methods for treating particular disease victim types. A number of avenues taken in the past can be reviewed and presented on this particular topic during my next series of reviews of past notes. The most important way to develop such a series of research questions is to apply a method used to evaluate case or claims data in order to identify the reasons for the most visits to a given health care setting, broken down by various age groups. In 2005/6 this was engaged in and tested, leading to the development and testing of a disease/visit monitoring system that could be run automatically based on monthly updated intranet data. In the end this project was not implemented, but it helped provide a much-needed understanding of how epidemiological events are recorded and happen for various populations and age groups. The goal of this 300+ disease/ICD-based monitoring program was to identify illness categories that could be assessed regularly to see if the numbers of visits are increasing for some unknown or unexpected reason. This epidemiological method can also be employed to some extent using claims and prescription drug data.

{kind=link}