
Giovanni Maria Lancisi (26 October 1654 – 20 January 1720),
Samuel Latham Mitchill (August 20, 1764 – September 7, 1831)
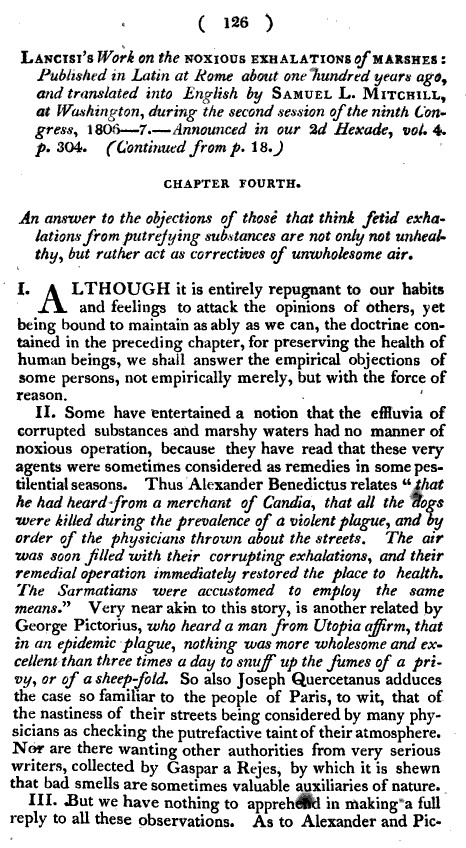
With this essay Giovanni Maria Lancisi became one of the chief initiators of disease theory as it related to climate and weather, latitude temperature and humidity, and ultimately medical geography. Any scientist or physician well read in the classics during the late 1700s would be familiar with Lancisi’s work. Some of the late eighteenth century political leaders and settlers of this country were familiar with it due to the insights it provided into historical epidemics like the plague that struck much of Europe the century before, and the fever epidemics generated on board ships that were passing through the tropics. Those who were interested in settling the New World would be most interested in Lancisi’s work due to the fluctuations in climate, humidity, rainfall and landforms that existed within foreign settings. Those who were interested in exploring and Lancisi’s writings were typically engaged for political reasons, and being familiar with Lancisi’s work gave them the advantage to knowing where the healthiest lands to claim, the health places to settle could be found.
Lancisi’s essay is based pretty much on a very simple paradigm about the cause for disease–the discomforting environment of a marshy region due to its humid air and insects was the source for whatever plague or fever ailed a particular region. Contemporary historians who are unfamiliar with the traditional writings like those of Lancisi will typically relate some of the terminology that developed due to Lancisi’s writings to the modern interpretations of these words. Malaria for example, whenever we read, makes us think of a specific disease type, with a specific treatment, and a specific way in which deaths and recovery ensue. Yet back in the 18th century, the modern definition for ‘malaria’ and its equivalents was not this way. Then the term malaria referred to febrile diseases noted to occur in ‘mal aere” settings, places with bad air. That bad air stank, was too humid, had a vile feel about it due to its acidity or tendency to make us cough, and did everything possible to us to make our throat feel tight, to draw the air out of us and make us feel fatiqued and even apoplectic. No matter what the true cause for the dreaded, unhealthy living setting was, the cause for the disease it forced upon us was the same–malaria, not the mosquito like the malaria of modern times.
This article details much of the philosophy Lancisi created for malaria, miasma and effluvium to become common disease related adages. Unfortunately this series of writings appear to be incomplete, although in terms of content they are not. It may be missing its last section due to lack of publication, for a potential next article in the series cannot be found. So suffice it to say, Lancisi’s work provides us with some important insights into how disease and the environment were defined relative to each other, and how these observations can be used to predict a given area’s disease patterns. During the first half century of colonial New York medical history, Lancisi’s philosophy prevailed in much of the medicine being practiced, whether that practice be directed towards the patient and his/her microcosm, or more robust in form with an added focus on the macrocosm.
An example of the influence of Lancisi’s work on North American medicine came during the 1720s to 1750s when New York Governor Cadwallader Colden referred to it in his description of the health of the Hudson Valley. This would be one of several paradigms used to practice medicine during those decades, and once the war began, it became a major driving force on the new philosophies for disease then being generated. We see Lancisi’s theory have its greatest impact once it is published in the early American Medical journals edited by Benjamin Rush of Philadelphia and Samuel Mitchell of New York City. Such an influence began around 1795 to 1797, as both of the medical scholars took center stage in their careers as politicians, physicians and social leaders in Pennsylvania and New York respectively. But over the next few years, as more diseases began struck the United States, one of these two major supporters of Lancisi, Dr. Mitchell, became a Wernerian, someone heavily devoted to the total geographical viewpoint of natural history and geological theory combined, with the basic concepts of disease derived from this group’s teachings. Dr. Rush in Philadelphia did not rely so much on the Natural History paradigms for diseases as he did the roles of human lifestyle and behavior on disease and its development. Due to this major difference in their philosophies, both Rush and Mitchell would be at odds with each other for years to come.
This publication of a translation of Lancisi’s Latin essay we can not only take to be a political move, or an intellectual statement of Benjamin Rush, but also one of his strongest statements made for this region based on the Wernerian philosophy of the evolution or creation of diseases. Over the next few years, Mitchell developed a number of other theories for disease that at times appear to be offshoots of Lancisi’s philosophy. As Benjamin Rush continued to develop his own theories related to his experiences in Philadelphia, and the experiences of his neighbors with epidemic diseases throughout Philadelphia, he developed a perspective on nature and disease that was quite different from that of Mitchell. This article didn’t help at all in resolving that issue, but it did help Mitchell make a name for himself in terms of popularizing some old disease concepts and bringing up to par with the belief systems for the time.
.
………………………………………………………………………………………………………….
.

.

.

.
.
.

.

.

.

.
.
.
.
.
.

.

.
.
.

.

.

.

.

.

.
.
.

.
.
.

.

.
.

.
.
So far, no continuation of this article was found.
.
.
