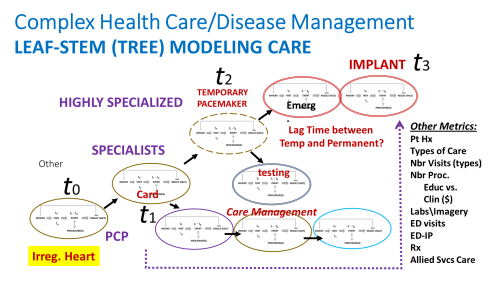
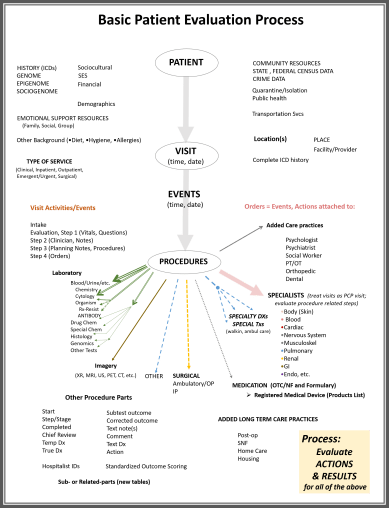
Applying my method for modeling care to cases, we can begin to develop a method for evaluating the complete quality of care a person receives throughout his or her lifespan.
This method is made simpler by evaluating all of the processes of care by relying upon methods that break down the care in different parts –defined by the meaning and purpose of the care–such as regular visits, versus emergent care, versus hospital-based need, and/or the need for special surgical needs (to name a few). Some databases are designed to facilitate that method of subclassifying all of the care services.
By looking at the care processes using these groupings, and then assessing the care by the age of the victim and determining if the care is preventive, palliative, remedial, or reactionary, we can learn a lot about the health care process. Are certain institutions or care givers more likely to work at the latter end of the listing just provided? Are they primarily preventive healthcare givers, or reactionary and palliative or remedial in nature? By applying this to how perform their services for each health condition, we can determine how effective a healthcare system, institution, facility, program, or practitioner is when it comes to meeting the needs of their patients who are becoming older, evolving new risks over time, predictable at times due to the nature of health in comparable patients enrolled in the program(s).
These next few case examples are of these theoretical patients. They are receiving the same baseline care from their primary care practitioners (PCP)s, but are experiencing different health conditions and medical experiences within the care system due to their differences.
It is assumed for the moment the each patient’s manner of receiving and affording healthcare doesn’t change throughout his/her life. So the transition from medicaid to medicare at 65 years of age, or the changing of insurance coverage once a kid turns 18 (plus or minus with Obamacare), are not applied to this model. Likewise, a patient’s change in coverage expected for changes in career status are not, for the moment, considered in this method for modeling care. (But believe me, the inclusion of these changes in life will be added to this model over the next few months.)
So, only the major health or disease problems are looked at. Each of these, as described elsewhere, consist of processes that are provided by the physician as a standard part of the healthcare process, and are not included in the billing of care. Other parts of the care process are billed, like the labs, use of most of the diagnostic testing equipment (xrays, MRIs, etc), engagement in the use of certain medical equipment, the cost for medications, etc.).
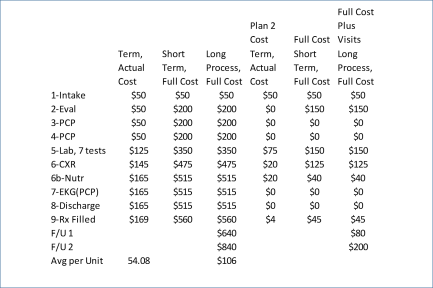
Example of assigning costs for theoretical cost analyses. These are the procedures engaged in as part of a standard PCP visit, for preventive care, in the form of an annual visit, followed up by two lab-related visits and a renewal of medications.
Therefore, one part of this evaluation method being developed enables an analyst to compare care processes to which costs are assigned and billed, against those which lack cost and are provided for “free”–such as giving a patient educational materials, making recommendations about diet, taking the vital signs of the patient, providing a reference to another clinic–none of these should be charged to the patient, and are generally considered part of the standard primary care process for the patients presence or stay within the facility (during a doctor visit or while lying in the hospital bed).
The special procedures, however, do have costs attached to them. Evaluating this care model I developed, we can look at cost-related procedures versus unbilled activities, to see how “rich” the entire care process is, with regard to the processes the clinicians opt to engage in (or try to save money by not including in their care process). This method may also be used to detect MDs that favor certain processes over others, due to procedure type and name, and/or cost (i.e. avoiding the less expensive PET scan in exchange for ordering an MRI or CABG process).
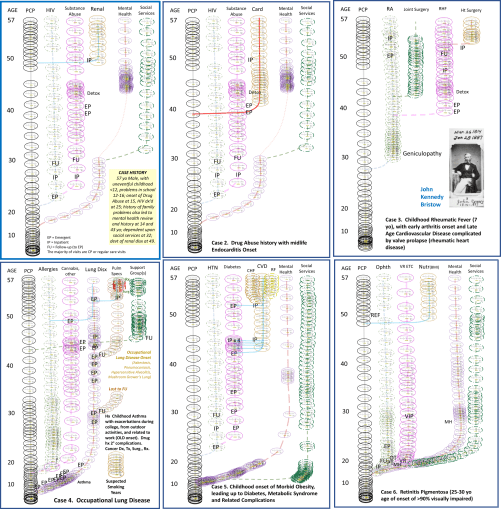
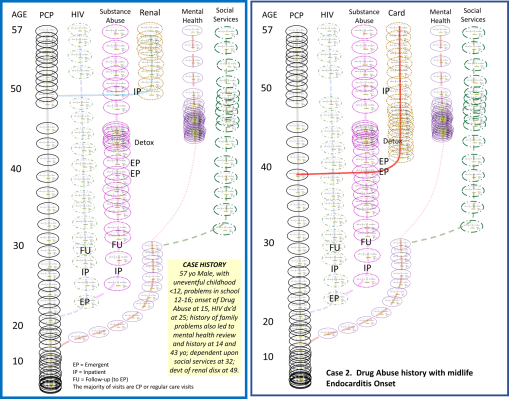
The first example above is of the HIV case I presented a month or two ago. Instead of renal complications, this patient experiences endocarditis onset in his/her forties due to the use of unsterilized needles. These two scenarios have different onsets of complications at different ages, involving different organ systems. One research question to ask regarding this scenario is:
- Which of the two possible experiences will cost the patient more?
- Assuming that otherwise the two health care experiences are the same, where will the costs differ?
- Which one of the two may have post-procedural processes that cost the patient more?
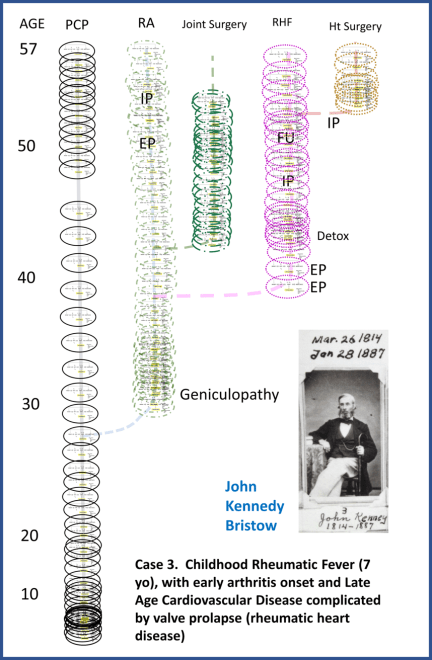
Note: For the above scenario, the case is historical, but the theoretical application is modern–the heart surgery was of course not available for Dr. John Kennedy Bristow at the time. For more on his life, see the pages I posted on him elsewhere on this website.
This next scenario is of a nineteenth century physician I biographed about 25 years ago. His entire life’s medical history could be evaluated due to the records he kept, which are in possession of the Oregon Historical Society. He experienced rheumatic fever as a child, and this fever ultimately had long term effects upon his health as he aged. His changes in occupation, and his notes as a physician about his health, enabled me to produce the above simplified time chart of his life health experience. This will be evaluated on a future page. For now, this is meant to serve as another example of graphing or depicting a patient’s lifelong health experience. (He died at 83; for this presentation he will be reviewed at the age of 57.)


These next two cases are of a patient who unfortunately suffered a number of pulmonary related complications in life. The second patient is facing the consequences of a high BMI at a very young life.
The figures demonstrate the difference experiences the two cases had over the years. Each one of the ovals is a visit (or set of visits and procedures), with a cost attached to it. Each branch in the healthcare process pertains to a different ongoing health issue. Some of these issues engaged only clinicians. Others engaged the mental health staff. Still others involved the special services made available to patients who experience some sort of handicapping effect of their conditions.
The pulmonary case is a reflection of several types of individuals I worked with during my stay in the Pacific Northwest during its peak Old Growth Forest years. The pulmonary condition defined by the local geography was a form of Occupational Lung Disease, in the form of Hypersensitivity-induced Alveolitis, due to the sequiterpene lactone (SQL) rich liverworts growing on old growth forest trees. Tree cutters who cut the trees along its trunk and base were exposed to dust generated by this plant, which often covered the tree bark of the oldest trees. By inhaling it, they exposed their upper and lower respiratory passage to the powder, and the SQLs released by it. The result was a combined obstructive-, chemically-induced autoimmune form of pulmonary disease, that resulted in the swelling of the surfaces of bronchioles and alveoli. (for more, see my page on this.)

For a young child with asthma conditions experienced at school, for example as a result of exercise, growing up in this area may expose the child unnecessarily to this environmental risk factor capable of causing severe chronic obstructive pulmonary disease problems during the later life. Young workers, unaware of these potential long term consequences, increase their risk further by obtaining fulltime work in this exact industry (due to the rareness of other occupations for certain regions), and/or by engaging in either tobacco or cannabis smoking activities, thereby further exposing their lungs to potentially irritating inhalants. The above model depicts what we’d expect a typical Pacific NW lumberjack, with a history of asthma or COPD at midage due to lifelong smoking, to experience were he to be employed in tree felling, or even in the cutting of raw wood into lumber, with or without adequate respiratory gear.


The next case, a child with morbid obesity developed at a very young age, has several factors to be concerned with, which in turn effect how that child’s care may be evaluated and monitored. First of all, there may be a genetic reason for this problem that needs to be evaluated. Second, family history, family members, and family-promoted lifestyle may be a factor in defining how and why the child became morbidly obese during the elementary school years. Third, social and community related behaviors generated in response to his or her appearances and medical status may also be partially at fault for this state, determinable by engaging the child in a psychological assessment, and perhaps later, assistance by a nutrition specialist.
The final factors ultimately determining the child’s potential lifespan depending upon the other consequences of this obesity, defined by what is currently termed “metabolic syndrome” related obesity and the subsequent engagement of other organs and organ systems, ranging from the vascular system due to the onset of hyperlipidemia and hypertension, to the onset of heart disease, gall bladder disease, pancreatic disease (including pancreatitis and obesity-induced, formerly “adult-onset” diabetes). These in turn may also be linked to renal failure, loss of vision, and peripheral neuropathy, loss of circulation, and loss of distal appendages due to gangrene.
Both of the above conditions demonstrate how problems experienced as children during the elementary school can have serious consequences on lifespan and quality of life during the later decades. Each of these patients experienced a unique pathway that is in fact fairly common to many patients in the U.S.


These last two cases, for this review, are chronic conditions with lifelong implications. Both are of real people.
The first is a female with retinitis pigmentosa identified during her mid-teen years. This genetically-based disease is the first of its kind diagnosed for her family. During her later teen and potential-college years, it impacted her decision making regarding career choice. She went to college and earned a bachelors degree followed by a terminal degree in the allied health sciences. She then toured the world, learned a variety of complementary health philosophies and practices, spent three years at a retreat, and then returned blind to commence her work in healthcare. She experienced few other problems due to her health or physical state, but required considerable assistance at the social services and physical/occupational therapy levels. As a result of aging, physiological changes impacted her health slightly.
The second is a person who experienced some health conditions that possibly led to the onset of seizures during the preteen middle school years and the diagnosis of epilepsy by 7th grade. This impacted employability and career choice, leading the person to attend college for a bachelors and terminal degree. Epilepsy related problems began at midlife, during the immediate pre-career years, leading to the need for a variety of medical and allied health services, and social services. Ultimately, the problem was alleviated, enabling the person to return to the workforce and experience health problems common to aging in those with a separate family history of older age disease.
The exercise in understanding this method of organizing an analysis of a patients total lifetime, healthcare experience, is to consider the numbers and costs for specific groups of events or experiences, for each of the primary health problems noted by the titles at the top of each set of healthcare operations or events.
These are simplified examples. They exclude old old age related events and the impacts of aging once the age of 65 is reached and the patient becomes eligible for Medicare coverage, and perhaps special housing (long term care, assisted living) where healthcare services are available as needed.
Each visit has a cost attached to it, as does each billable procedure, each operation, and each billable action that is needed to engage in a diagnosis or improvement in quality of life/lifespan for a patient. Theoretical costs can be assigned to each step and each branch in this model. More branches can then be added to evaluate the minor differences in health care, such as those who undergo organ replacement, the initiation of dialysis care, or any other unique process not commonly considered when total cost is the concern for prediction modeling.
More of these examples of ICDs and their costs are currently being developed. This model may be used to evaluate any healthcare processes or programs engaged in long term care management. It may also be used to serve in prediction modeling, of cost, or expected outcomes, for given patient experiences before and during the healthcare process.