2016
Yearly Archive
May 3, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on The Gate Theory & “Herd Effects”
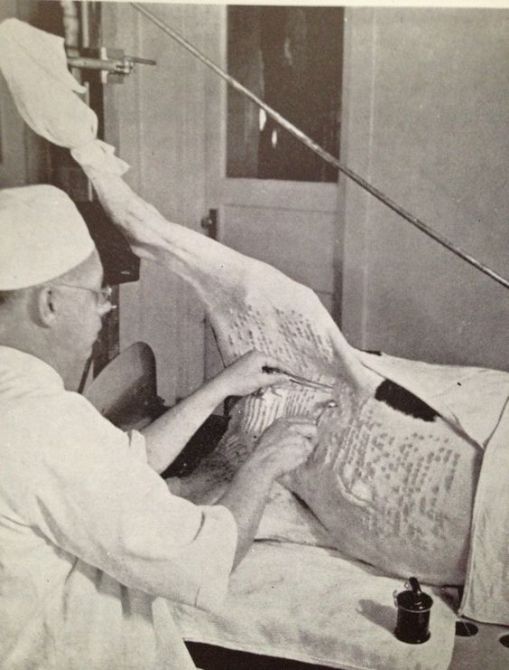
Figure: From my old Pharmacognosy text by Evans, ca. 1940s. The first vaccine ever developed used “kine pox” (the serum extracted or scraped away from a cow with pox infection in the skin.) This process for manufacturing vaccines for the Pox maintained the use of the cow into the mid 20th century. This is how the pox was extracted from cattle during the 1940s. Whether the cow in this picture was bred to be “hairless” (reduced hair) or is just very cleanly shaven is uncertain.
Reading the news story about the Harvard Mumps outbreak in the dorm–there is really just one line you have to walk away remembering from this story:
[Quote] ” . . . people in college dorms often share living spaces with dozens of people, giving them more opportunities to be exposed to the virus, either on surfaces or through contact with other people, Adalja said. Although being vaccinated against mumps can prevent a person from getting sick if he or she has been exposed to lower levels of the virus, for people living in dorms, vaccination may not be enough to ward off an infection, he said.
“The exposure that they have to mumps is so high in these situations that it overcomes the ability of the vaccine to protect them,” Adalja told Live Science. “It may be that, in these special situations, a much higher level of antibodies [against mumps] is needed to keep the virus at bay,” Adalja said.”
[END QUOTE]
Wait a minute . . . wasn’t being vaccinated supposed to have a “herd effect”? This would mean that if all the college students in the dorms are vaccinated, we needn’t worry.
See http://www.foxnews.com/health/2016/05/02/mumps-outbreak-at-harvard-why-do-vaccinated-people-get-sick.html

OLYMPUS DIGITAL CAMERA
A portrait of a past mentor of mine, Dr. Daniel Fox. An MD at SUNY Stony Brook and expert Medical Historian, he was a major influence on much of my work. He removed from SUSB around 1989 for a Chief Editor position with the Milbank Quarterly, a medical journal devoted to the federal programs that define the healthcare system and provide rules and regulations in the establishment of the current managed care system, the development of HMOs, and the establishment of many of the Federal programs devoted to health, such as Medicare and Medicaid.
The “HERD EFFECT” provides a very false sense of security to people in medicine, in particular those who contest my past three years of reminding people that 1) theories are perceptions, not facts or truths, 2) theories are good some of the time, not all of the time, and area based on the culture of the places they are born, where the definitive observations are made, and 3) theories in medicine are, in many cases, just as good now as they were back then (remember the lancet?).
The purpose of theory is guide us into understanding a phenomenon we are observing. A person into innovation and change works with multiple theories, multiple options, multiple routes to take in the analysis. A genius is a skeptic of theories, because all theories require skeptics. In medicine, it was the skeptics who decided the theory of four humours was off, or that the alkaline theory of blood and disease so common around 1790, did take into account the chemistry of the blood, but made some false conclusions.
We should be thankful that theory got replaced, right? It was replaced by the nervous energy based theory of the body, which enables scientists to argue sensibly about how life was an process totally derived from natural energy, and the “medical electricity” was the panacea of the future. And in a few years it was the future, people changed their minds about older ideologies in medicine, decided the old time teachings were out of date, and that the theory of disease and how to cure it had to somehow be replaced by more welcoming philosophies.
The discovery of the vaccination using kine pox serum, and the nearly synchronous discovery of the magical powers of homeopathy is not coincidentally proven around the same time as vaccines for any different reasons. The two were derived from the same theory, and took different paths in the philosophical synthesis and use in medicine. Franz Anton Mesmer would be steadily arguing with Volta and Hahnemann, each contesting the other “experts'” claims, not realizing in a decade too, they too would not longer completely correct, that their ideology would have to be changed to be practiced, again and again and again, until doctors finally got it right.
Allopathy’s gate theory of pain still remains a basic idea that we are taught in introductory nervous system courses. The herd effect is taught as a lesson and a rule, but it should be hypothesis, less in value than a theory, and in today’s classes used as a reminder of a theory that this ideology or philosophy medicine relied so heavily upon is failing. It is not a theory any more, and to mention it as your guiding lines of reasoning in the discussion of the failure of infectious disease vaccination programs, enables those who see failure happening to point to you as the cause–you and your old, out of date theory.
Medicine is no longer like it used to be when the philosophy of “Herd Effect” was born. We are more observant, and needs to use the imagination less to know when the events that ensue and the theory that supposed explains them, are a mismatch.
The above statement – – – “The exposure that they have to mumps is so high in these situations that it overcomes the ability of the vaccine to protect them,” – – – is an excuse for a failed theory. It demonstrates lack of acceptance of being wrong. Physicians and medicine are not humble. They hate to admit they are wrong when they are. But in the end, such a stubbornness only embarasses the profession further.
The younger generations, going to college as premeds, are either with you or against you in allopathy when your theory fails to hold its ground once changes happen. Patients, students, shouldn’t be assumed to be part of some great Pavlovian experiment that medicine is engaged in, mesmerizing you until you either given up and accept what is claimed, or are somehow tricked into believing that the gold leaflet they wrote this “Truth’ upon has to be correct, because of who wrote it, not the work and evidence developed to prove it is still true.
It is very easy to eliminate this problem. Open the gate and let the new theories in.
April 23, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Most Popular Pages
My top pages in recent months are as follows.
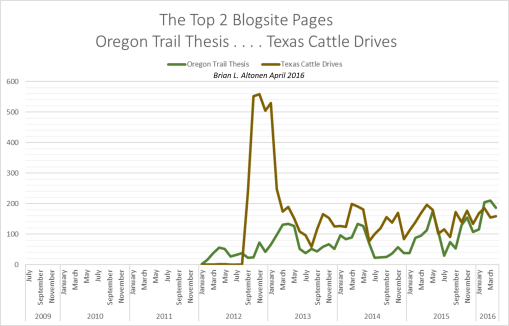
The large response to posting the Texas Cattle Drives page a few years ago has leveled out to the amounts displayed in the graph. Review of my page on the Oregon Trail thesis, demonstrating how to use mapping to investigate a historical outbreak, is my second most popular page. (There is also a blog site with the thesis and sections of work not included in the thesis for review.)
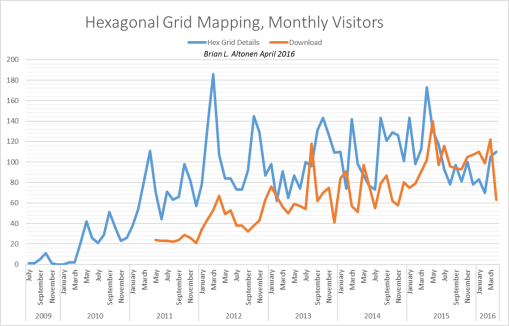
I am most interested in the hexagonal grid mapping site and its download page for the excel file I used to produce my first hex grid maps. This methodology is perhaps the most important addition to medical GISing techniques that I decided to undertake around winter of 2004, a technique which has not been fully appreciated as of yet. My argument for its value focuses primarily on the use of this method to reduce errors in data mapping and analyses.
I am due to develop the hex grid algorithms in several other formats for people to incorporate into their repertoire. I have to develop the SAS and perhaps SQL formulas for it. These will be employed within the next year to evaluate urban density patterns for medical research.
April 3, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Managed Care and Medical GIS Surveillance, 2016

At What Level is Your Managed Care Program GIS-Savvy and Literate?-
For a couple of years I have been pointing out where the managed care profession lies in terms of its skillset when analyzing population health.
Most managed care companies left nearly half their potential behind when they ignored the advancements in GIS that developed over the past ten years. These changes in computer hardware and software, information technology, electronic medical records, data warehouse development, exceptionally large storage areas for long term medical records, made it possible for the research of 10 to 15 years of medical data to suddenly be accomplished by individuals like myself. With the right expertise in data mining and aggregation, the goal of producing GIS applicable findings is now possible. In a single day, several dozen diagnoses, research questions, spatial analyses can be performed at a moment’s notice. This past week along, I averaged more than 100 analyses per day using some of the most gratifying algorithms I developed for risk prediction and defining individual patient health, healthcare related needs.
It is important to note that insurance companies initiated the idea of mapping health, back in the 1860s and early 1870s. They stopped utilizing this means for evaluating health when the bacteria theory erupted, diverting the attention of many epidemiologists from the environmental setting, to the home setting and environment immediately next to the patient’s body, school, playground, party sites, meeting rooms, and workplaces.
The image at top depicts the status we are at in managed care when it comes to GIS utilization. It depicts the common behaviors seen in the managed care field, the level of accomplishment healthcare programs have reached when it comes to reaching their marketing and business potentials.
On a scale of 1 to 10, I place our system at 5.5, almost 6. That is to say we focus on retrospective analyses and information production and display for the most part. We rarely use spatial modeling to make predictions about our programs, its financial growth, its patient population, the local community health-related changes. We do not utilize grid mapping techniques, nor prediction modeling, nor quarterly spatial display of our services and finances, nor economic and quality of service assessment programs to score and improve our projects.
To many, taking the chance that well over half of them may have little impact or fail remains a major deterrent. Knowing the field your are in, and where and how to start such an exploratory process, is also a skillset lacking in upper level management.
But the advantage to employing an aggressive spatial surveillance and prevention-minded medical GIS is seeing the impacts of those few successes financially and healthwise. Chances are, if you evaluate 50 to 300 features of population health, design your surveillance system such that it allows you to engage in well targeted intervention programs, you make it possible for good news stories to be generated for your program by the end of each and every year.
The following are potential uses for medical GIS-HIT, which is why I keep the score for where managed care unexcitably low, and why the level of potential growth this business experienced at embarassing levels.
All of the others professions in healthcare have developed more rapidly and completely that managed care, regarding the use of EMR data. While programs still struggle to get their EMRs working, experts in GIS working in managed care are taking their data and doing hundreds of times more analyses and reporting, than simple meaningful use report writing can achieve.
For much more, see nationalpopulationhealthgrid.com

March 26, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on The value of 3D Mapping (and Algorithms)

Over the last 6 or 7 years I have been “showing off” this algorithm I designed nearly a decade ago, longer in terms of copyright and intellectual property rights claims.
This way of modeling disease patterns is a direct product of my first studies of spatial data, which ironically focused on remote sensing and the value of raster imagery before I was able to see the value of a standard point-line-arc or point-line-polygon geographic information system (i.e. the ESRI and MapInfo GIS products from the mid 90s).
When I developed my first algorithms, they were for differentiating land use patterns, in particular regarding vegetation types and the patterns changing “browns” and “greens” they produced in the various early Landsat and AVHRR imagery then available for research. I came up with/developed and tested some unique algorithms for overlaying trend surface models to identify important edges to overland diffusion processes, such as for a migrating animal bearing disease, or a pathogen capable of spreading as wind-blown materials. I even used these to study the nature of very large repeated forest fires developed due to a combination of climatic, meteorologic, topographic and phytochemical (resin index) features. These algorithms were used to exaggerate 3D differences, converting them from linear to logarithmic in order to depict the most important “hot spots.”
Later I found a use for these algorithms in evaluating population density, public health related features. The same algorithms that defined edges for conifer rich regions in the mountains could be used to define religious, cultural, age pattern density, environmental disease, elevation, traffic flow, and sociocultural disease type edges. The edge of outbreak and outbreak susceptible areas can be defined quite easily using mixed 2D and 3D modeling.
You can also overlay certain features on some of these diagrams that can be developed in the right SAS programming (not at all requiring SAS GIS). These features include risk area patterns, critical p lines demonstrating the edge of a break out area, points depicting where the event peak is relative to local police and fire stations, a hospital, an emergency care facility, a specialty clinic in charge with specific public health concerns.
The amazing thing is that today, with the current technology, without ArcGIS, QGIS, Cognos, Tableau, these maps can be produce, in record amounts per day. All of the 45-60 Meaningful use (MU) metrics can be evaluated several ways (by facility, by race, by ethnicity, by clinic, by provider, by provider type, as percent performance) in a single run of the program, using the right macros.
In a regular Data Warehouse, it takes a day or more to develop the macro from scratch. But then, once it is finished, it is written such that it can be applied to other metrics. The process for using a macro-based process for running your daily ED evaluation or weekly MU review, cost analysis, enables up to 2 or 3 hundred tests to be run in less than two hours. In terms of 3D modeling, producing multiple images of the same result, depicting the same finding but at different rotational angles, it takes a few minutes more to produce several maps, a half hour more to produce hundreds of them.
What takes the most time right now at this end for mapping diseases and health / visit behavior is the time to pull the data (it sometimes take just as long, a half hour to a few hours, times 5 or 10 on occasion).

On a good day, I have found that one can spend 3 or 4 hours writing up the logic, the sql and SAS needed to pull the data and reassess it, resort it, count it out, in such a way as to produce your numbers. Add another half hour to merge this with your overall population data for comparisons (i.e. for incidence/prevalence measures), and if necessary link as well any additional spatial data required by your facility for the areas to be assessed (i.e. pull in zip code data for: facility, special location, and even patient residence for proximity to care measures).
A great program in managed care, that implements GIS and spatial analysis, is productive in 3 months at the demographic, basic numbers level. It should be producing spatial data (maps or the likes thereof) in 4 to 6 months. Depending upon the software used for GIS (which is not required so far), another month or two is needed to develop the actual GIS tool process for a standard coarsely mapped zipcode or county (even census block or clock group) based system.
- A GIS based managed care system should be able to engage in meaningful use related activities such as:
- location analysis of 0-2 yo immunization completion findings,
- develop of a clustering algorithm for mapping asthma and COPD patients,
- engaging in a study of relationships to completion of well visit requirements relative to facility types and service hours
- mapping suicide attempt rates (V and Ecodes), as an age-gender-race metric
- developing comparative studies of cancer risk testing rates at the socioeconomic level,
- evaluating STD spatial distribution relative to age group and ethnicity
- documenting diabetes prevalence rates for specific zip code defined areas
- documenting the distribution of spouse abuse events in EMR derived by Ecodes information
- relating SES and median income to costly chronic disease medication timely refill statistics
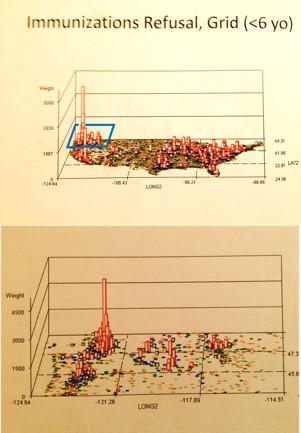
- producing areal maps of immunization refusal family clusters based upon Vcodes
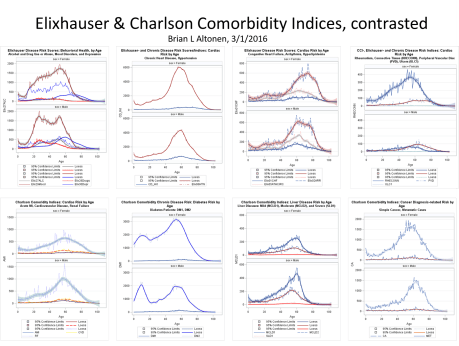
- mapping zip code or retirement facility specific overall health risk in 3D, based upon Charlson comorbidity (CCI), Elixhauser comorbidity and federal Chronic Disease Management algorithms.
There are three major stages or series of processes required to develop a spatial GIS for managed care. I have identified these as EMR, Spatial, and then GIS stages.
The EMR Stage is the development of data into a usable form for spatial analyses. Nearly all managed care facilities have the goal of reaching this stage in their development. A few programs even implement some form of Cognos, Tableau, ESRI tool, QGIS, or the like, for information mapping. Information mapping is different from Spatial Analytics mapping.
There are a number of places that engage in pseudo-spatial mapping. They analyze data by simple areal and point features (EpiINFO / EpiMAP style of work), don’t actually engage in spatial analysis, but spatially present their findings. Some even use these products to design special needs or intervention programs. If a pre-post evaluation is performed, the spatial process is well on its way to being implemented as a standard part for a Managed Care program.
One level above this pseudo-spatial analysis is using spatial techniques with a spatial purpose. Like developing a spatial data program that utilizes zip codes to define areal risks based upon age-health features, and then using the spatial process to define cluster areas or predict where the next clusters of cases will emerge, such as new diabetes patients over 65 or more cases of toxic lead paint exposure in low income urban settings.
Proactive use of spatial methods in an essential part of the true spatial analysis routine. Reactive or retroactive spatial evaluation are simply that–a review of the past, but without a particularly well defined reason other than to better understand an event. In the west nile example I engaged in more than 10 years ago and posted, I used GIS (but spatial processes) to evaluate west nile clusters of positive testing hosts and vectors, then set traps to prove that a local vector existed at the nidus of spatial centroid of that area, and then used that area to demonstrate that the mosquito carrying this disease could survive the following winter; which it did, enabling me to come up with the first early Spring positive testing sample. (I have a page or two posted on this.)
In sum, the spatial process of spatial analytics development within a managed care system involves understanding and employing your spatial formulas, even though your company may not be regularly using a GIS to meet its requirements.
Spatial techniques may also, incidentally, be used to evaluate SES, demographics, marketing, cost performance, fund raising program success, public interaction of the healthcare program or facility with the local populations. Spatial evaluations of this sort are often requested, but often by engaging outside resources to provide the mapping and analytics required, due to the cost of the staff and hardware associated with this form of productivity.
Spatial analysis at the institution. health care level is reached when data is functional and used by a facility, from its EMR warehouse. These uses includes areal analyses of some sort, engaged in regular, and as part of occasional or once only programs such as for a grant funded research. Forward thinking is also required for a spatial analysis program to truly be engaged. This means that production at the next stages need to be ongoing, with regular presentations provided at times to inform the right people. Presentations at local meetings and conferences are also essential to making the program stable, ongoing, able to discover more areas of interest in need of research, more groups of people and npos that can benefit from continuing the program, and more followers at the production and performance level, including other workers with similar skillsets and their own unique spatial analysis abilities.
The third stage, or GIS stage, of this setting, occurs when an actual GIS is incorporated into this process, not just for demonstrating results in a report, but for use in analyzing specific questions, completing analyses that cannot be easily performed in the spatial tools that do not map (prediction programs that calculate probability, but don’t map; SAS generated tables and charts, but not maps). Two forms of GIS are traditionally recognized as applicable to healthcare–the line-vector and the raster system. Both should be available to the managed care system and be used for spatial databasing, operations development (testing and designing algorithms specific to your program), presentation (at managerial on down to public levels), prediction modeling, and producing final summaries or atlases depicting your program’s spatial results, for the annual report required of most healthcare systems.
At another site I am working on the details of all of the reporting that can and should be done by a managed care combined EMR-GIS/spatial analysis program (a small part of my dissertation work.)
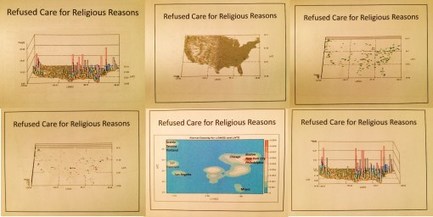
At several locations I posted examples of many the above mentioned products. (I’ll also try to post some examples here).
[Note: I also have a survey posted at SurveyMonkey, querying those engaged in managed care or GIS and health about their experiences in this field.
Participation in this survey is of course appreciated from this end; it abides by IRB requirements; no personal info is divulged; it exists only due to my work as a leader in this specific epidemiology/population health specialty. Please visit it at https://www.surveymonkey.com/r/JW88X3F ]
This slideshow requires JavaScript.
March 8, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on Learn Disease Mapping
To GIS students: Invest in Medical GIS
The Trump Healthcare plan will no doubt provide opportunities for growth and change. But the same opportunities could be argued for any new healthcare plan that is proposed over the next 18 months.
We fall for the same tricks every time the healthcare systems appears to be a failure. One of these tricks is condemning the recent past, while making promises for the weeks and months ahead.
Does anyone remember when Clinton and Gore were running for president? What was it that the two of them offered to the American people? What they offered was not any different from what we are still trying to establish today. Since that run for presidency, there have been no successes made in the attempted improvement of healthcare insurance programs available.
The common cause for all of these failed presidencies and laws passed regarding health care (the HITECH Act for example) are the same–the insurance companies. You cannot reform health care without reforming the insurance company, the role of the insurance company, how it should managed healthcare insurance, and how it needs to either bow out of the health insurance industry (hard for some, since that is all they do), or come up with a plan that they are willing to take responsibility for, and follow.
The common thread to the slowly maturing failures of health maintenance organizations since Nixon signed them into existence, is equivalent to that of Presidents Ford, Carter, Reagan, Bushes 1 and 2, etc. etc, etc. The common thread is the health insurance industry, an industry with too little competitions, too much merging allowed, too much regional pseudomonopoly-like settings.
Trump’s idea of allowing citizens to produce and managed their own medical savings accounts in theory makes sense, that is assuming we did not treat them like we treat the family’s educational account established for kids. That money must not be allowed to be pulled for anything but for what it was originally intended, and that money should be treated like money put away for retirement–it must never be taxed.
The way disease and health mapping come into play here is at the clinical and, believe it or not, the insurance industry level, maps can be used to reduce the cost of anything and everything pertaining to the rising cost of care. Yet, why don’t these industries use maps to surveil their patients or members–the source of their revenue?
The health insurance industry and many health administration people haven’t an inkling of an idea on how to read a medical topology map. They don’t know how to interpret statistics (not simple reported information in the form numbers, actual p values and Chi-squares used to determine statistical significance). These businesses do have statisticians capable of understanding the basic non-spatial ways of developing statistical insights. But these same businesses do not know or understand the steps required to develop spatial statistical information.
This means that in order to be ahead in the healthcare profession, you have to learn spatial statistics, not simple t-Test, ANOVAs, Chi Squared methods or even survival plotting. You have to know and work with theoretically, and with the ability to develop new protocols in health statistics methods, using spatial data. GIS is the main way to convert any non-quantifiable measure into a quantifiable measure, by relating the measure events or things to each other over time and space. If children in one zip code use a specific swear word with sexual innuendos, and that term they use is very different from the terms used by another place, because another culture is there, you can document the publishing of the swear words as graffiti, and analyze their relationships to each other, and to the types of churches that exist in the same neighborhood, not to mention measures of race, ethnicity, average age, average history of income, or citizenship.
Does the current plan for improving our healthcare system make it possible for more attention to be paid to previously ignored social and cultural events with meaning? Is healthcare more than just the patient-doctor-billing agent (collectors) relationship? Is it possible to make sense of each and every event that happens, good or bad, moral or immoral, culturally correct versus politically correct? GIS tells use the answers to these questions. It takes second to apply GIS to billing data, to determine where physicians are prescribing more drugs than expected, or being paid much more than would be predicted for a given area with specific population derived predicted healthcare needs.
Obamacare was developed to improve upon the HIT system that exists, encourage or force programs to commit to developing an HIT. The Obamaplan also had the idea of monitoring performance of healthcare systems and businesses.
The Obamacare system has lost its race because the wrong directions were taken by the entire system and its administration. No attempts are made to make the insurance companies more liable for their laziness, malfeasance and malpractice. And if there is an insurance company you have that your are wondering about, if that insurance is a large scale company with other affiliates in the country, then that company is probably one of the dozens I analyzed to see how inefficient the companies can be, how skill-less they are becoming, and how incapable they are of seeing into the future of the healthcare industry. They are still living as reactionary businesses, not proactive preventive healthcare focused businesses.
So, to make GIS work for your job as a technician looking for work in the healthcare insurance industry, the best thing to do is to look into how this is being done, in managed care. This site I am putting together on Managed Care Innovations, will allow those who are “literate in healthcare statistics” to do just that, not the insurance companies (stuck in their way), but the newcomers to this field. A lot of my methods are there–but you have to be able to interpret programming language to determine how it can be done quite effectively.
There are a series of requirements for establishing an HIT system so that it is capable of developing into an HIT-GIS workstation. There are a series of large scale metrics that have to be accomplishable in a system. Since 2006 I have worked with agencies that report on thousands of metrics in some way shape or form, not just the 40 to 60 required for meaningful use. Systems and technology savvy IT managers, directors and statistical experts can produce two or three thousand metrics per years–they can analyze all of the patients for unhealthy lifestyle, poor genetic history, multiple chronic disease mortality and morbidity indices. They can analyze the congenital conditions, and relate culture and place to costs and losses in revenue. They can evaluate the culture of their patient load, and know where people are most likely to engage in spouse abuse, illegal surgical practices entered into EMRs in the form of specific ICDs, places where exposure to the environment might be causing learning disorders in children, or hampering the performance of patients in terms of engaging in preventive health activities.
March 7, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on What about Trump’s Healthcare Plan?
(From https://www.donaldjtrump.com/positions/healthcare-reform)
HEALTHCARE REFORM TO MAKE AMERICA GREAT AGAIN
Is this plan crazy?
My guess is a lot of people are going to take little to no look at this plan, and immediately verbalize their opinions about, even recommendations against it.
The sources for resistance to such a plan, at this point in time, is where the U.S. stands in regard to the presidential race.
A year or so ago, I was still supporting the Obamaplan rather steadily and daily in my postings on LinkedIn, ScoopIt!, and even this site.
This changed when the news was out on the use of penalty fees for patients – – – or should I say potential and returning patients — to hesitate about filing due to concerns about hidden costs, accrued on a per need basis, such as co-pays. The penalty fee was recommended for those who failed to commit to a plan, or failed to sign up for one when that was the expectation.
Most people don’t file for insurance due to limited incomes, even those from the middle class. Myself included, the costs for adding my name to an insurer’s program, in addition to the amount I would probably have to pay when I went for care, especially emergent care, puts patients in a position where the impact is the same no matter what decision you make, about pre-paying or pay once the need arises.
But still, the worst part about the Obamaplan is that it penalizes every one involved in health care, from the patient to the physician and nurse, to the administrators and hospital staff who have to make up for losses accrued when patients, insured or not, cannot comply with the rise in health care that the Obamaplan resulted in.
That one good thing about the Obamaplan is that is covered a significant number of people who were a month or two earlier uninsured. But that really isn’t worth the amount of members lost in healthcare plans due to the costs involved. And it certainly doesn’t make up for when insurance companies and states decide to bow out of the Obamacare plan, like North Carolina did, in order to avoid having to deal with the problems inherent to its operation at the insurance company level, the health care facility level, the billing agency level, the collection agency level, . . . and oh yeah, the patient level.
When a plan doesn’t care who it impacts and turns into a victim of change, that plan is not at all democratic or “American” in nature. It is totalitarian or oligarchic like in nature–it only benefits the few programs in charge of these operations. It only benefits the patients and administrators who don’t have to subscribe to this “New Deal.”
In 2015, New York City had 1.4 million patients enrolled in a medicare/medicaid program. Due to the Obamaplan, in less than 6 months, this membership dropped to 1.25-1.33 million, depending upon your definitions. That is a 0.o7 to 0.15 million drop in insured patients–or in real numbers, a drop of 70,000 to 150,000 patients in half a year. The Obamaplan is not intended to increase enrollment. It is intended to change enrollment. The cost accrued by the patients who did depart their previous plan, may now be uninsured, and cost the newly insured more for healthcare by the end of a year.
So relating this to the Trump plan, the goal of the Trump plan is a generic one, plainly stated, focusing on the most important parts of healthcare that all os us like to complain about. The Trump claim is as follows: “to create sound public policy that will broaden healthcare access, make healthcare more affordable and improve the quality of the care available to all Americans.”
The next section is a description of seven attributes to this program meant to improve the healthcare system, as it exists now. As follows . . .
[Begin Quote]
*********************************************************
Congress must act. Our elected representatives in the House and Senate must:
- Completely repeal Obamacare. Our elected representatives must eliminate the individual mandate. No person should be required to buy insurance unless he or she wants to.
- Modify existing law that inhibits the sale of health insurance across state lines. As long as the plan purchased complies with state requirements, any vendor ought to be able to offer insurance in any state. By allowing full competition in this market, insurance costs will go down and consumer satisfaction will go up.
- Allow individuals to fully deduct health insurance premium payments from their tax returns under the current tax system. Businesses are allowed to take these deductions so why wouldn’t Congress allow individuals the same exemptions? As we allow the free market to provide insurance coverage opportunities to companies and individuals, we must also make sure that no one slips through the cracks simply because they cannot afford insurance. We must review basic options for Medicaid and work with states to ensure that those who want healthcare coverage can have it.
- Allow individuals to use Health Savings Accounts (HSAs). Contributions into HSAs should be tax-free and should be allowed to accumulate. These accounts would become part of the estate of the individual and could be passed on to heirs without fear of any death penalty. These plans should be particularly attractive to young people who are healthy and can afford high-deductible insurance plans. These funds can be used by any member of a family without penalty. The flexibility and security provided by HSAs will be of great benefit to all who participate.
- Require price transparency from all healthcare providers, especially doctors and healthcare organizations like clinics and hospitals. Individuals should be able to shop to find the best prices for procedures, exams or any other medical-related procedure.
- Block-grant Medicaid to the states. Nearly every state already offers benefits beyond what is required in the current Medicaid structure. The state governments know their people best and can manage the administration of Medicaid far better without federal overhead. States will have the incentives to seek out and eliminate fraud, waste and abuse to preserve our precious resources.
- Remove barriers to entry into free markets for drug providers that offer safe, reliable and cheaper products. Congress will need the courage to step away from the special interests and do what is right for America. Though the pharmaceutical industry is in the private sector, drug companies provide a public service. Allowing consumers access to imported, safe and dependable drugs from overseas will bring more options to consumers.
********************************************************
[END QUOTE]
Entitlement 1. We’ll begin by skipping this first order, except for a brief comment. People have a choice about whether to pay for care or not. There is a problem with this ideology for, which is if employers decide to no longer give in to providing some form of health insurance as part of the employment process, that the current markets out there will turn into haves and have-not industries. Big businesses will reward employees with healthcare coverage. Minimum wage or low wage businesses will hire, but make its workers poorer if they have to pay for health insurance on their own.
Entitlement 2. Remove the cross-state border issues with healthcare. This is a new one to me, having worked in healthcare, medicaid and medicare claims related issues. Sure, there are problems with obtaining insurance from your federally subsidized and funded state agency–like Medicaid and Medicare. And programs that cover people in this way, always make it more expensive for you to receive care from an out of state facility. Even more, if you obtain care from an unapproved facility, provider, company, without preapproval, this care could very well cost more as well. The cross-state borders concern may help certain people receiving certain forms of care. In places like NY, where people may cross over to Connecticut to receive better care due to the location of an Acute Care hospital, this problem theoretically already exists. Yet it has not hampered upstate NY care that much. I would need to see more details about what interstate care this clause pertains to. More important perhaps would be a similar clause allowing patients to travel for less expensive care, by engaging in the now rapidly growing medical tourism industry. I would rather have my colonoscopy performed for $1,000 instead of $5,000 to $7,500, and on a nice Caribbean Island rather than is a grimy urban neighborhood, where the hospital or facility is surrounded by everlasting construction events and hazards, and inadequate parking space.
Entitlement 3. Allow individuals to deduct health related costs from their annual income tax returns. Not at all contestable. This should have been there from the beginning. The government has to either choose to pay for your healthcare entirely, and tax your full income, or deduct what you have to pay as a matter of governmental choice.
Entitlement 4. Health Savings Accounts–why do these opportunities keep returning? It is the choice of the agency providing them that is responsible for this decision. The company is irresponsible with this potential healthcare insurance option. This is also like that option you have, that comes and goes, of putting some money aside that is pulled from your paycheck, for miscellaneous health expenses. You lose it if you don’t use it up by the end of the year.
Entitlement 5. Price transparency. This is where I can get personal about all of this. A procedure performed on a medicaid patient, that costs $350, will inevitably cost a patient covered by some form of commercial insurance two or three times as much. The low cost for the medicaid patient is because the government only covered a little under 50% of the billed amount, and the healthcare facility/insurance company usually is expected to accept this drop in payment. So they make up for the medicaid, unemployed and disabled patient induced losses in income by doing something one step short of deliberately overbilling those who can afford to pay. What’s worse about this aspect of healthcare billing habits is that a single procedure can have many different costs for the many different parts and programs in the U.S. Costs for care are not defined as having to be within a given range, or for a specified amount. Potential costs for opting for a healthcare service should be transparent to the patient population. People like myself, who analyze and company the different BCBS’s and United *** insurance agencies, can determine where overbilling is being performed strategically, at the agency level. How else can we compare the cost for a procedure nationally, if we continue to accept these varying differences in billing strategies and amounts. Such inconsistent pricing makes it impossible to safely evaluate the cost for healthcare and the Big Data level. I use my own price sheet to review and compare these plans.
Entitlement 6. Block Grants. Nothing completely new here. Not like this hasn’t been done before. The thing to do is make block-grant required. For some states, this means we go back a few years, or generations, in terms of how the state managed its patients. The history of this type of payment plan is already in place, due to Medicaid and Medicare. We use Block Grant like options as well for other things we do, such a develop new schools, or determine where to invest in certain infrastructure requirements in decomposing urban settings. IF not for the failure of that last use of clock grants, we could argue that this method could work very often.
Entitlement 7. Remove barriers for the marketing of healthcare. As usual, that is always a good option, but it can result in a unique set of have and have nots. Some form of care is essential, and overcharging for it is an issue. It’s like saying the poor cannot have the best surgery, only the quick fix. There are already a lot of rules an regulations about invention, marketing, testing of new products. There is nothing new inferred by Trump’s plan regarding the expected rules to remain in effect regarding patient safety. Trump’s proposals will not cause another Thalidomide tragedy to erupt. Pharmaceutical industries are the cause for their own demise, or lack of success with their products, as the controversies behind certain unproven medications continue to show. This issue has to be evaluated more strategically, and with more detail. The one form of healthcare that needs to be added, once again, is the medical tourist industry option, for expensive processes, but maybe for alternative means of cultural healthcare processes as well. (It’s up to you if you want the Brazilian shaman to heal your Pinta or Chiclero’s Ear, or the African medicine man to treat your African American heritage induced genetically-derived cardiomegaly.)
So what’s Missing?
I’ll review that next.
February 6, 2016
Posted by Brian Altonen, MPH, MS under Uncategorized
Comments Off on What Florida is doing to stop the Zika virus

Florida’s hot, humid climate puts its 20 million residents at risk — along with millions more tourists
Sourced through Scoop.it from: www.cbsnews.com
It is one week into February. For New York that means we are5 or 6 weeks away from paying close attention to the first mosquitoes. The first pests are those that successfully overwintered. This spring will be full of those pests, because this winter has managed to steer clear of too many El Nino-La Nina effects. It has snowed only once up in my county, and been miserably cold for just a week or two.
But the first adults to re-emerge from their winter hibernation should be carrying much, we hope. There haven’t been too many positive testing cases with West Nile and Chikungunya like we feared late last summer.
So weather and climate determine when the first southern disease bearers will impact this part of the States. Whereas Aedes aegypti is the vector epidemiologists have to watch to the south, Anopheles are the pests we may have to pay close attention to up here, perhaps Aedes.
So where do the Aedes mosquitoes penetrate the US with their tropical diseases?
I mapped the answer to this questions years ago. See https://www.youtube.com/watch?v=eHyehbfOwFo
West Nile is a related disease; but it rapidly migrated across this country ecologically. Can Zika virus do the same? This video is of the success that West Nile had crossing this country in just a few years: https://www.youtube.com/watch?v=VKtREeEtkaY
The way Mosquito Viral Encephalitis is distributed in this country is at : https://www.youtube.com/watch?v=YGu_hY_r0Ko
It shows where the Dengue is brought into the US by Aedes, via people. NY is the center for possible in-migration of the disease by infected people. Whereas Florida, Louisiana, and numerous southern states riddles with mosquitoes are how it will enter this country ecologically.
I produced a rich resource on how to evaluate mosquito-vectored diseases using GIS. I developed a method for ecologically profiling places, to determine where these critters are most likely to run rampant, and where they will mathematically cause to most chaos to ensue and the likelihood for unexpected diseases to penetrate the local wetlands and swamp-ridden areas.
The following is how I used a light sensing device to develop a better ecological understanding of mosquitoes, in relation to land use patterns and ecological vegetation-domain status: https://brianaltonenmph.com/west-nile/west-nile-surveillance-2/
Remote sensing tells us plenty about an ecosystem and whether or not it has the features to develop a stable ecosystem for vectored diseases to survive. See https://brianaltonenmph.com/west-nile/6-remote-sensing/
My study of species for these vectors: https://brianaltonenmph.com/west-nile/vectors/
My vegetation survey derived plant ecology study: https://brianaltonenmph.com/west-nile/3a-west-nile-surveillance-1/
My surveillance of cases: https://brianaltonenmph.com/west-nile/case-related-surveillance/
My method of assigning risk to areas: https://brianaltonenmph.com/west-nile/assigning-risk/
My review of topography, landform and vector patterns (won an award for this): https://brianaltonenmph.com/west-nile/topography/
My NLCD grid mapping method of evaluating vector and host distributions: https://brianaltonenmph.com/west-nile/nlcd-grid-mapping-and-west-nile/
My introductory page on how to do this monitoring of diseases using a GIS, with plenty of pages to follow, is https://brianaltonenmph.com/west-nile/
My award winning west nile ecology poster, 2006: https://brianaltonenmph.com/about/west-nile-ecology-poster-session-at-2006-esri-conference-denver-co/
I posted numerous videos of zoonotic disease behaviors in the US based on 1998-2012 EHRs (the past 15 years), at https://www.youtube.com/playlist?list=PLWrApErk5byYvO6ZHvDzgzmPqOGs1WI9B
and
https://www.youtube.com/playlist?list=PLWrApErk5byZnE0bWUqdfH4CYVmnETLg6
FOR STARTERS . . .
See on Scoop.it – Medical GIS Guide
« Previous Page
