JULY 4, 2014. Ebola News and Information Updates.
Source: uk.news.yahoo.com
July 14, 2014. The long term predictions for Ebola are not overly surprising.
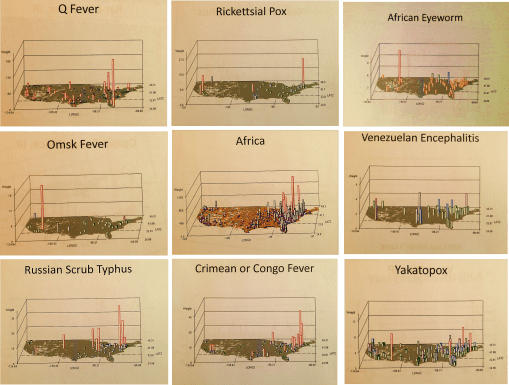
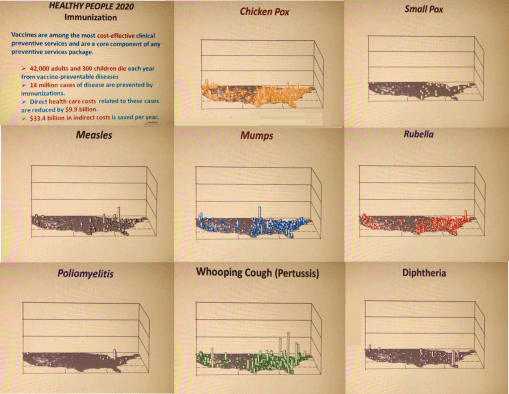
A fairly realistic view of outbreaks like those for Ebola rely upon the assumption that these outbreaks are primarily of natural and human ecological in nature. In the long run this can means that they are more difficult to suppress than a disease diffusion process that lacks a natural ecological component, and is dependent mostly upon just people interacting with other people, mostly in human occupied places.
We learn about future disease patterns for a disease from other countries by looking at how similar diseases behaved in the past. The behaviors of west nile for example to date have been very much like those of the early 19th century yellow fever. The diffusion processes for the recent outbreaks from the Caribbean of Chikungunya are very similar to vector-host relationships, climate of origin and diffusion by transportation for the 19th century typhoid fever. As for Ebola, . . .
these few observations beg the question: If we apply to this same logic to Ebola, relying upon matchable natural and human ecological matching disease patterns, what might we come up with?
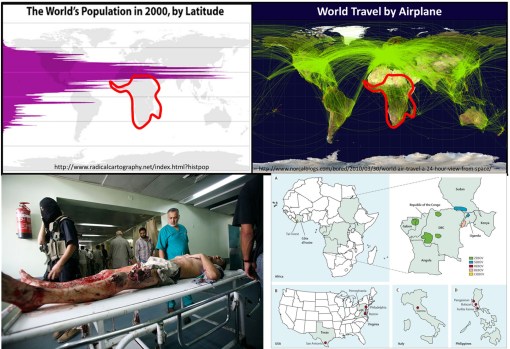
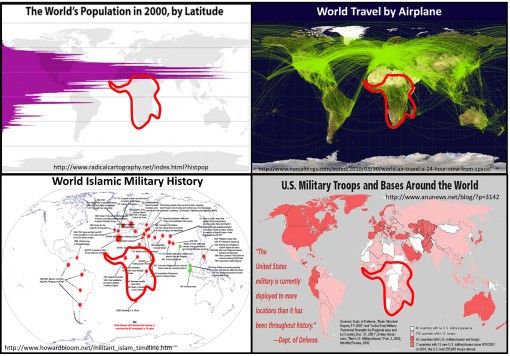
Current speculation is we are still far from the opportunity for a diffusion of Ebola to other parts of the world. Ebola’s zoonotic behaviors suggest a limited "metazoonotic" region (according to Pavlovsky’s and Voronov’s definitions) for the time being. Until the host-vector ecology is somehow changed, or its genetically defined tendencies to survive based on interactions with nature change, the "metaecology" of host, vector, organism and combinations thereof remain the limiting factor(s).
EBOLA LINKS/UPDATES:
UK NEWS. (July 3). W. African Ebola epidemic ‘likely to last months’, says UN. At https://uk.news.yahoo.com/w-african-ebola-epidemic-likely-last-months-says-185447906.html#fakodRB
CBS News (July 2). Ebola rages through West Africa, with no signs of stopping. At http://www.cbsnews.com/news/west-africa-struggles-to-fight-off-ebola/
The Guardian. (July 2). Monica Mark. Fear and ignorance as ebola ‘out of control’ in parts of west Africa. At http://www.theguardian.com/world/2014/jul/02/-sp-ebola-out-of-control-west-africa
ALJAZEERA. (July 2).
Ghana hosts crisis talks as Ebola toll rises.Ministers from 11 African nations meet to plan "drastic action" as death toll from haemorrhagic fever reaches 467.
THE TELEGRAPH. Mike Pflanz. (July 3). Ebola ‘out of control’ in West Africa as health workers rush to trace 1,500 possible victims. Fear, mistrust of Western medicine and difficulties reaching remote areas mean hundreds of potentially infected people have not yet been found. At http://www.telegraph.co.uk/news/worldnews/africaandindianocean/guinea/10942598/Ebola-out-of-control-in-West-Africa-as-health-workers-rush-to-trace-1500-possible-victims.html
CNN NEWS. Laura Smith-Spark. (July 3). Ebola virus: Can nations stop deadliest ever outbreak from spreading? At
http://www.cnn.com/2014/07/03/health/ebola-outbreak-west-africa/
BBC NEWS. (July 3). Ebola outbreak: West African states agree strategy. At http://www.bbc.com/news/world-africa-28156263
CBC NEWS. Daniel Schwartz. (July 4). Ebola epidemic unlikely to spread beyond Africa. Deadliest outbreak of the disease still a challenge to contain. At http://www.cbc.ca/news/health/ebola-epidemic-unlikely-to-spread-beyond-africa-1.2695879
CHIKUNGUNGYA. LINKS/UPDATES:
European Centre for Disease Control and Prevention. Chikungunya. http://www.ecdc.europa.eu/en/healthtopics/chikungunya_fever/pages/index.aspx
Eric M. Leroy, Dieudoné Nkoghe, Benjamin Ollomo, Chimène Nze-Nkogue, Pierre Becquart, Gilda Grard, Xavier Pourrut, Rémi N. Charrel, Grégory Moureau, Angélique Ndjoyi-Mbiguino, and Xavier de Lamballerie. (2007). Concurrent Chikungunya and Dengue Virus Infections during Simultaneous Outbreaks, Gabon, 2007
Emerging Infectious Diseases. Volume 15, Number 4—April 2009. At
http://wwwnc.cdc.gov/eid/article/15/4/08-0664_article
NBC News – MAGGIE FOX. Bugs at Your July 4th BBQ? Beware of Chikungunya and West Nile. At
MICHAELEEN DOUCLEFF. Chikun-What? A New Mosquito-Borne Virus Lands In The U.S. At http://www.npr.org/blogs/health/2014/07/03/327760854/chikun-what-a-new-mosquito-borne-virus-lands-in-the-u-s
For more on the Russian philosophy of disease ecology, by Evgenii Nikanorovich Pavlovsky (1884-1965), and A. Georgy Voronov, see:
—my thesis, Overview at http://wp.me/Puh6r-3HT, or full project and supplement chapters, not published except on the web, detailing the history of the medical geography and disease ecology fields, at http://oregontrailcholera.wordpress.com/
—my webpage and dedication to , "Zoonosis and Russian Medical Geography", at https://brianaltonenmph.com/gis/historical-disease-maps/zoonoses/
or, the following classical reference:
—Human Diseases with Natural Foci. (Abstract/Description for purchase) 1963. At: http://www.cabdirect.org/abstracts/19642702411.html;jsessionid=05B0F21042EF4956C63AE975AC35B36D