See on Scoop.it – Episurveillance
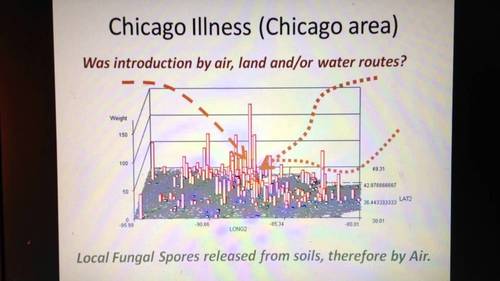
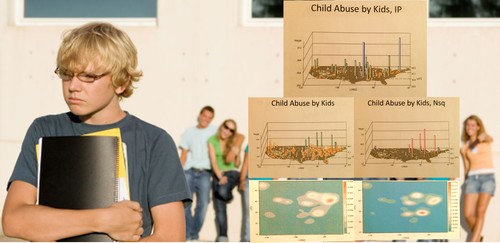
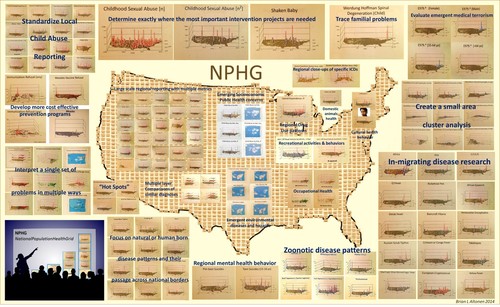
Outside the CDC and other epidemiological and public health work environments, other programs can monitor and report on their vectored diseases patterns. The most rapid way to analyze any ecological, population base, or culturally and socioeconomically based disease pattern is by grid mapping.
Grids have been criticized in the past because they are not exact. Current systems can manage the small area grids and map results incredibly fast and with an incredibly high resolution less than the spatial error contribution. These systems need not be GIS, but can include standard Big Data sets up designed for SAS (not SAS-GIS) and SQL. Adding GIS also means your are also adding a tremendous amount of work due to whatever programming (“tweaking of the maps”) is involved. This also increases the cost for producing and maintaining an effective surveillance system, and it can increase the likelihood that researchers’ or presenters’ bias and presentation error could impact your work.
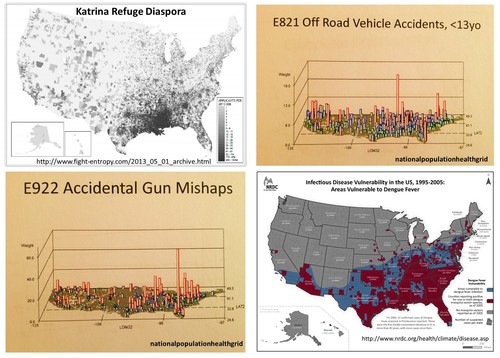
One can accomplish the same using Teradata. It takes just 10-20 minutes to map a total of 2400 25 mile areas, representing the outcomes for the entire U.S., up to 1000 maps per data run, 24k per day, for one analyst. [See NPHG pages for more.]
Chikungunya Cases Double in CaribbeanNBCNews.com-Jun 5, 2014… Vincent and the Grenadines, and Saint Maarten),” they wrote in theCDC’s … “As of May 30, 2014, a total of 103,018 suspected and 4,406 … Officials have been cautioning that the virus could become established in the U.S. …Mosquito-Borne Chikungunya Virus Spreads in the Americas
Medscape-Jun 6, 2014 The next mosquito-borne infection you might want to start worrying …
Washington Post-Jun 5, 2014 Chikungunya Cases Increase in the Americas
Guardian Liberty Voice-Jun 7, 2014 Mosquito-borne chikungunya cases double in Caribbean
WXIA-TV-Jun 5, 2014 Mosquito-borne virus a public health nuisance
In-Depth-San Jose Mercury News-Jun 4, 2014