Nearly 10 years ago (time flies!), I performed extensive research on the in-migration of diseases from Africa and other continents and large countries, completing that project more than five years ago.
I identified more than 100 diseases that can be easily monitored, continuously, by a managed care program. I used this project to demonstrate that if the ICDs of these diseases are placed into a single search tool for EMS, and the resulting “hits” assigned locations based upon their latitude and longitude, that plenty of leads can be found about how diseases migrate into this country, not to mention how people behave. Ebola is one of those diseases I mapped.
Sourced through Scoop.it from: www.newsweek.com
Now, with the possibility of sexual transmission of Ebola, living and working in the vicinity of one of the non-compliant healthcare providers to bring Ebola into this country, these events made me recall my years in medical school, during the early to mid 1980s, when AIDs had yet to receive a formal name, and when the first research into HIV and AIDs migration and sexual transmission patterns came to be, as one of my mentors was forced to leave his position as administrator of the medical school, due to his refusal to publicly refer to the university officials’ desire to link the new epidemic coming to be to a small community located in and about Queens.
Now granted, the organisms behind AIDs and Ebola are very different. What happened in New York and later California may not be at all like what happened 30 years ago in the U.S. In an evolutionary sense, as well as a physiological and adaptive one, the organisms responsible for each are very different, although the routes of transmission, sexual behavior, may not be as different as we’d like to think.
What HIV taught us is that carrying and disease and spreading it elsewhere around the world can become a long, drawn out event, enabling the organism to mutate, survive better, change from a rapidly fatal pathogen to a wandering one in search for new hosts.
It will be interesting to see if people behave like they did between 1985 and 1986, and 1986 and 1988, when leaders in my medical communities in NY and later OR tried to lay blame on specific ethnic groups for the introduction of a new disease to specific communities in Long Island where I did my rounds on the hospital floor, and still later in specific parts of California, the second time through.
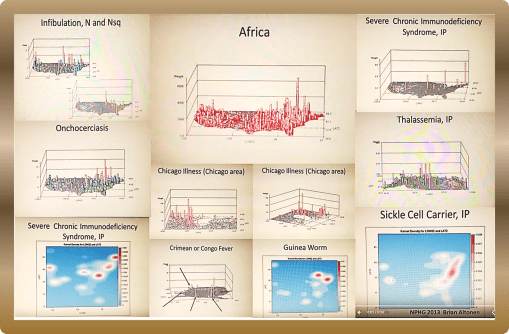
To understand how African diseases impact this country, back then, in African, and in the U.S., begin by reviewing my work of the Geography of African Diseases that I produced years ago from a large national health dataset . . .
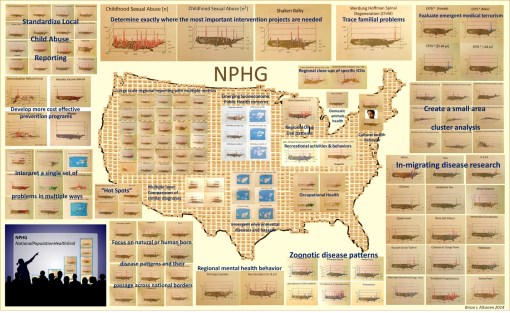
My method of developing the first videos to display the national distribution of these diseases, individually as well as as a collective, appears much like a GIS, but it was produced without GIS software. I designed my own algorithm for this 3D mapping methodology eons ago.
Begin with:
VIDEOS of the NPHG Product include:
African Diseases
https://www.youtube.com/watch?v=qi-fXinlTjE
Geophagia as an African behavior:
https://www.linkedin.com/grp/post/2601248-5936505909034364929
African Eye Worm
https://www.youtube.com/watch?v=dSP6tOQs-RQ
Obscure African Cardiomyopathy:
https://www.youtube.com/watch?v=hSj78VNYMbY
Bejel:
https://www.youtube.com/watch?v=RI9Z0HXZFUg
Guinea Worm
https://www.youtube.com/watch?v=YwSnpT7hAI8
Crimean or Congo Fever
https://www.youtube.com/watch?v=YWuMBOdB08k
Elephantiasis
https://www.youtube.com/watch?v=Uc6zvqutU3g&list=PLWrApErk5bybFfsOWTXWjlwvIM7D4d6-h&index=22
Assorted Videos in a row:
https://www.youtube.com/watch?v=x4VR1rf6C78&list=PLWrApErk5bybFfsOWTXWjlwvIM7D4d6-h&index=20
Ebola
https://www.youtube.com/watch?v=RfvUQfYLlvM
AIDS/Severe Chronic Immune Deficiency
https://www.youtube.com/watch?v=IIQh7bLpgZs
Noma Page
https://brianaltonenmph.com/gis/population-health-surveillance/production-examples/528-1-noma/
POSTINGS in ScoopIt! about Ebola, each a lesson in itself:
Pages on the Geography of Ebola:
and Mapping the Outbreak of Ebola:
http://www.scoop.it/t/episurveillance/p/4039425741/2015/03/18/ebola-mapping-the-outbreak
http://www.scoop.it/t/global-health-care/p/4034141340/2014/12/24/ebola-mapping-the-outbreak
See on Scoop.it – Medical GIS Guide