See on Scoop.it – National Population Health Grid
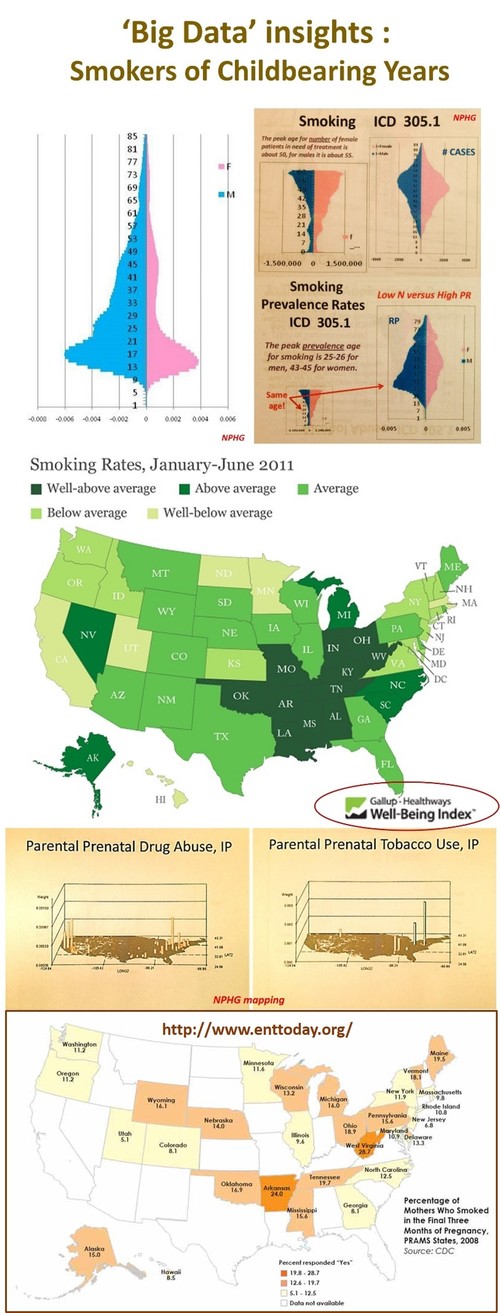
Insights into the national studies on smoking rates and exposure risks. Including a review of the findings of “Sensorineural Hearing Loss Linked to In-Utero Second-Hand Smoke Exposure”, an article published in Archives Otolaryngology Head & Neck Surg. (2011;137:655-662) and summarized on EntToday — October 2013. Last Figure contained in this article is “Percentage of Mothers Who Smoked in the Final Three Months of Pregnancy, PRAMS States, 2008.” Source: CDC..
There has been a substantial change in smoking rates over the past few decades, but two public health issues still deserve our attention. The first is the racial and gender discrepancies in smoking rates. Regarding race or ethnicity, young adult African Americans have higher rates of smoking into their 30’s than caucasians, who appear to reach a peak in their mid 20s. When we compare prevalence rates for one year age bands between genders for either group, it is not unusual to find the number of female smokers documented in EMRs to continue to increase in number until they reach their midlife years (around 45), whereas male smokers peak about 15 to 20 years earlier.
.
The second major finding with smoking still in need of aggressive education and prevention programs are the smoking habits of pregnant women. The two maps of drug abuse and tobacco use show the peak areas in this country, based upon a spatial evaluation of the national data (NPHG project). The last map in this set (and the LINK for this image) is about how smoking results in sensorineural loss of deficits in newly born children.
.
According to a study published last October,
.
–"[T]he overall prevalence of maternal smoking during the last three months of pregnancy at 12.8 percent in the participating states, ranging from a low of 5.1 percent in Utah to 28.7 percent in West Virginia" (see map).
.
–"[B]abies born to women who smoke while pregnant have a higher risk of premature birth and low birth weight and an increased risk of sudden infant death syndrome (SIDS), cleft lip or palate, asthma, obesity and cognitive deficits, among other injuries."
.
–New findings show an association between sensorineural hearing loss (SNHL) in adolescents and secondhand smoke (SHS) exposure (Arch Otolaryngol Head Neck Surg. 2011;137:655-662). The authors for this report linked SHS exposure in prenatals and newborns to health conditions or risks such as SIDS, asthma, respiratory tract disorders, cognitive and behavioral problems, and the increased risk of otitis media.
See on www.enttoday.org